The Subthalamic Nucleus Influences Visuospatial
Attention in Humans
Barbara Schmalbach, Veronika Günther, Jan Raethjen,
Stefanie Wailke, Daniela Falk, Günther Deuschl,
and Karsten Witt
D
o
w
N
l
o
UN
D
e
D
F
R
o
M
Astratto
■ Spatial attention is a lateralized feature of the human brain.
Whereas the role of cortical areas of the nondominant hemi-
sphere on spatial attention has been investigated in detail, IL
impact of the BG, and more precisely the subthalamic nucleus,
on signs and symptoms of spatial attention is not well under-
stood. Here we used unilateral deep brain stimulation of the
subthalamic nucleus to reversibly, specifically, and intraindividu-
ally modify the neuronal BG outflow and its consequences on
signs and symptoms of visuospatial attention in patients suffer-
ing from Parkinson disease. We tested 13 patients with Parkinson
disease and chronic deep brain stimulation in three stimulation
settings: unilateral right and left deep brain stimulation of the
subthalamic nucleus as well as bilateral deep brain stimulation
of the subthalamic nucleus. In all three stimulation settings, IL
patients viewed a set of pictures while an eye-tracker system
recorded eye movements. During the exploration of the visual
stimuli, we analyzed the time spent in each visual hemispace, COME
well as the number, duration, amplitude, peak velocity, accelera-
tion peak, and speed of saccades. In the unilateral left-sided stim-
ulation setting, patients show a shorter ipsilateral exploration
time of the extrapersonal space, whereas number, duration, E
speed of saccades did not differ between the different stimula-
tion settings. These results demonstrated reduced visuospatial
attention toward the side contralateral to the right subthalamic
nucleus that was not being stimulated in a unilateral left-sided
stimulation. Turning on the right stimulator, the reduced visuo-
spatial attention vanished. These results support the involve-
ment of the subthalamic nucleus in modulating spatial
Attenzione. Therefore, the subthalamic nucleus is part of the sub-
cortical network that subserves spatial attention. ■
INTRODUCTION
Hemispatial neglect is a condition that is characterized by
a failure to explore the side of space contralateral to the
lesion and to react or respond to stimuli or subjects located
on this side (Karnath, Himmelbach, & Rorden, 2002). Per-
sistent neglect is often the consequence of a right parietal
(Mort et al., 2003) or right superior temporal lesion com-
monly seen after stroke (Karnath, Ferber, & Himmelbach,
2001). But neglect may also occur after lesions in other
brain areas such as the frontal lobe or subcortical structures
(Committeri et al., 2007; Mort et al., 2003). In chronic
neglect patients, lesions restricted to the right BG or
thalamus have been reported to induce neglect as well
(Karnath et al., 2002). Within the BG, the right putamen
and caudate nucleus have been identified to be crucial
structures associated with spatial neglect (Karnath et al.,
2002). But studies investigating the impact of BG on
neglect demonstrate heterogeneous and even contradic-
tory results because lesion studies on spatial neglect after
stroke use different lesion-mapping techniques and the
accuracy involved in investigating merely BG nuclei differs
Christian Albrecht University, Kiel, Germany
© 2014 Istituto di Tecnologia del Massachussetts
according to the mapping methods. Only a minority of
studies have also mapped the integrity of white matter
tracks, such as the superior longitudinal fasciculus, Quello
takes its course adjacent to the BG (Karnath, Rennig,
Johannsen, & Rorden, 2011). Tuttavia, a BG lesion may
also affect neighboring white matter tracts potentially
involved in the neural network of spatial attention.
Deep brain stimulation (DBS) of the subthalamic
nucleus (STN) is an established therapy in advanced stages
of Parkinson disease (PD; Deuschl et al., 2006). Although
the mechanisms of bilateral STN-DBS are not well under-
stood, DBS is believed to interfere with increased output
from the BG and thereby to improve the functions of their
target structures (Bergman, Wichmann, & DeLong, 1990).
Previous studies have used acute effects of STN-DBS as a
tool to reversibly and intraindividually modify the activity
in BG circuits (Schroeder et al., 2002). Whereas bilateral
STN-DBS has been studied more frequently, unilateral
stimulation can also be tested under experimental con-
ditions by turning on one DBS electrode at a time. Under
unilateral stimulation of the left STN, PD patients have
shown mild but significant neglect behavior, neglecting
left-sided stimuli (Witt, Kopper, Deuschl, & Krack, 2006).
Tuttavia, in this study, we used a motor task that measured
Journal of Cognitive Neuroscience 26:3, pag. 543–550
doi:10.1162/jocn_a_00502
l
l
/
/
/
/
j
F
/
T
T
io
T
.
:
/
/
H
T
T
P
:
/
D
/
o
M
w
io
N
T
o
P
UN
R
D
C
e
.
D
S
F
io
R
o
l
M
v
e
H
R
C
P
H
UN
D
io
io
R
R
e
.
C
C
T
.
o
M
M
/
j
e
D
o
tu
C
N
o
/
C
UN
N
R
UN
T
R
io
T
io
C
C
l
e
e
–
P
–
D
P
D
2
F
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
C
7
N
3
_
5
UN
/
_
j
0
o
0
C
5
N
0
2
_
UN
P
_
D
0
0
B
5
sì
0
G
2
tu
.
e
P
S
T
D
o
F
N
B
0
sì
8
S
M
e
IO
P
T
e
M
l
io
B
B
e
R
R
UN
2
R
0
io
2
3
e
S
/
j
F
T
.
/
tu
S
e
R
o
N
1
7
M
UN
sì
2
0
2
1
RT while patients responded to visual cues in the right and
left extrapersonal hemispace. Consequently, the motor
domain, affected by PD and also affected by STN-DBS, era
the major outcome measure. In this study, visual explora-
tion behavior was tested using an eye-tracker system to
measure spatial attention in the ocular motor system, Quale
is less affected in PD. So we tested the hypothesis that the
STN is part of the attentional system managing space orien-
tazione. If so, the laterality of hemispheric specialization
with a superior function of the nondominant hemisphere
on spatial orientation should also be evident in the sub-
cortical nuclei and here, in particular, the STN that was to
be manipulated in the study.
METHODS
Patients
At the University Hospital in Kiel, we examined 13 PD
patients, 3 women and 10 men, 32.5 months (range =
6–100 months) after bilateral electrode implantation in
the STN for chronic DBS. All PD patients fulfilled the brain
bank criteria for PD (Hughes, Daniel, Kilford, & Lees,
1992), and all patients suffered from advanced PD. Patientsʼ
data and clinical characteristics are given in Table 1. None
of the patients had a diagnosis of dementia preoperatively
or postoperatively, and all patients scored ≥24 points on
the Mini-Mental Status Examination (Folstein, Folstein, &
McHugh, 1975) screening test. Preoperatively, there was
Tavolo 1. Demographic Data and Clinical Findings of
PD Patients
Age (years)
Male/female
PD Patients (n = 13)
62.13 ± 8.874 (39–71)
10/3
Disease duration (years)
16.31 ± 6.019 (10–29)
Right-/left-sided disease onset
8/5
Stimulation duration (months)
32.54 ± 27.573 (6–100)
Hoehn & Yahr ON-ON
Hoehn & Yahr OFF-OFF
2.23 ± 0.484 (1.5–3)
3.42 ± 0.703 (2.5–5)
Levodopa equivalence dosage
363.69 ± 218.955 (54–750)
Mini Mental Status Examination
28.62 ± 2.29 (24–30)
Visual acuity test right (%)
Visual acuity test left (%)
Amplitude right ( V)
Amplitude left ( V)
Pulse duration (μsec)
Frequency (Hz)
73.85 ± 15.021 (50–100)
72.31 ± 16.909 (50–100)
3.02 ± 0.804 (1.1–4.1)
3.05 ± 0.736 (2.0–4.5)
62.31 ± 8.32 (60–90)
167.31 ± 27.13 (130–210)
Data are given as absolute values or mean (range) and ±SD.
a predominance of motor symptoms on the left side
for five patients and on the right side for eight patients.
The neurological examination excluded strabismus and
deficits in the visual field. All patients had normal vision
or corrected-to-normal vision, and none of the patients
complained of diplopic images. The stimulating electrodes
(Medtronic, Minneapolis, MN) were implanted using
stereotactic MRI-based targeting and intraoperative electro-
physiology with microrecording and microstimulation
as previously described (Schrader, Hamel, Weinert, &
Mehdorn, 2002). For the determination of the position of
the electrode contacts, we used our stereotactic targeting
software (Brainlab, Feldkirchen, Germany). After placing
the AC–PC line (anterior commissure and posterior com-
missure) on the postoperative MRI, we determined the
position of the four electrode contacts by assigning the cen-
ter of the corresponding artifact. The stereotactic coordi-
nates of the active contacts in relation to the mid-AC–PC
point were marked on the corresponding normalized
horizontal sections of the Schaltenbrand-Wahren Atlas
(Schaltenbrand & Wahren, 1977). The preoperative MRI
did not show any large vessel infarction, and an MRI after
surgery excluded complications such as cerebral hemor-
rage. Patients were tested in a dopaminergic ON state. A
the time of testing, patients received an average levodopa
equivalent daily dosage of 363.7 mg. The protocol was
approved by the ethics committee at Christian Albrecht
University Kiel, and all patients gave informed consent.
Test Procedure
Each patient was tested in three stimulation conditions
in a double-blinded design: right electrode ON and left
electrode OFF (right ON/left OFF), right electrode OFF
and left electrode ON (right OFF/left ON), and both elec-
trodes ON (right ON/left ON). The order of the stimulation
conditions in which the patient was tested was randomly
assigned to every patient. Identical stimulation parameters
as for chronic DBS were used. All patients had unipolar
stimulation. The neurological motor examination (Unified
Parkinson Disease Rating Scale part III, UPDRS III) E
test procedure began at least 30 min after changing the
stimulation condition when a stable clinical status was
achieved. The examiner performing the motor evaluation
and the examiner testing spatial neglect were blinded to
the stimulation settings and the results of the motor eval-
uazione, rispettivamente. To quantify the degree of motor
symptom asymmetry, the left and right score sums of the
unilateral UPDRS III items (20–26) were calculated. Dopo
the motor examination, the patient was presented with
a set of pictures, whereas the patientʼs eye position and
movement were recorded by an eye-tracking system.
Stimulus Material
Forty-two visual stimuli were selected from the International
Affective Picture System (IAPS; Lang, Bradley, & Cuthbert,
544
Journal of Cognitive Neuroscience
Volume 26, Numero 3
D
o
w
N
l
o
UN
D
e
D
F
R
o
M
l
l
/
/
/
/
j
F
/
T
T
io
T
.
:
/
/
H
T
T
P
:
/
D
/
o
M
w
io
N
T
o
P
UN
R
D
C
e
.
D
S
F
io
R
o
l
M
v
e
H
R
C
P
H
UN
D
io
io
R
R
e
.
C
C
T
.
o
M
M
/
j
e
D
o
tu
C
N
o
/
C
UN
N
R
UN
T
R
io
T
io
C
C
l
e
e
–
P
–
D
P
D
2
F
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
C
7
N
3
_
5
UN
/
_
j
0
o
0
C
5
N
0
2
_
UN
P
_
D
0
0
B
5
sì
0
G
2
tu
.
e
P
S
T
D
o
F
N
B
0
sì
8
S
M
e
IO
P
T
e
M
l
io
B
B
e
R
R
UN
2
R
0
io
2
3
e
S
/
j
/
T
F
.
tu
S
e
R
o
N
1
7
M
UN
sì
2
0
2
1
2008). The visual stimuli were complex pictures represent-
ing objects, people, landscapes, and scenes of life. IL
pleasure level ranged from 4.5 A 5.5, and the level of
arousal was varied from 1 A 9 to increase patientsʼ alertness.
We selected an additional 21 landscape pictures from pri-
vate material. These were reflected vertically in the middle
of the picture (mirrored pictures). Using all 63 pictures,
we created three picture sets consisting of 21 randomly
assigned pictures, each of which 7 were mirrored and
14 were derived from IAPS. Every patient saw each of
these three randomly ordered picture sets only once and
presented in a pseudorandom order with regard to the
three different stimulation conditions, questo è, some pa-
tients began by viewing picture set 1 in the condition
right ON/left OFF and other patients began with picture
set 1 in the condition right OFF/left ON. By avoiding a
fixed order of picture sets, we minimized the risk that
the results were affected by the pictures themselves that
might have had asymmetrical eye-catching regions. Pic-
tures were displayed on a color monitor (24 in., resolution
1024 × 760, vertical refresh 70 Hz). The patients sat 87 cm
in front of the monitor (corresponding to vertical angle of
vision of 28.05° and a horizontal angle of vision of 21.5°) In
a dimly illuminated room. The monitor was connected to
a personal computer equipped with E-Prime presentation
software (Psychological Software Tools, Inc., Sharpsburg,
PAPÀ) triggered by the eye-tracking system.
Eye-tracking Recordings
The head position was stabilized with the eye-tracker
inbuilt chin and forehead rest. In every stimulation set-
ting, the system was recalibrated with a 13-point grid.
Fixation and eye movements were recorded monocularly
from the left eye with an infrared video-based eye tracker
(IView-X Hi-Speed 1250, SMI GmbH, Munich, Germany)
at a sampling rate of 500 Hz and an instrument spatial
resolution of 0.01° while patients viewed the pictures
binocularly. Patients started each 21-picture session by fix-
ating on a cross at the center of the screen for calibration.
Tuttavia, after this, patients were told that they were free
to look anywhere on the screen at the beginning of every
subsequent picture to evaluate the pictures afterwards.
Instantaneous eye position was tracked by an apparatus-
mounted camera (sensomotoric instruments) close to the
patientʼs left eye. The patientʼs gaze position was shown
on the experimenterʼs screen to monitor the patientʼs status
and the quality of the data. Each visual stimulus was on the
screen for 10 sec, so viewing one picture set took 210 sec.
After observation of each picture, patients rated emotional
valence and arousal using the 9-point Self-assessment
Manikin Scale (Lang et al., 2008). This task served as moti-
vation for detailed observation of the picture.
Eye recordings were classified into three categories.
“Fixation duration” was defined as the time between two
saccades with a minimal 80-msec rest of eye movements.
“Saccades” were defined as any movements of the eye,
and “blinks” were defined as the time duration that no
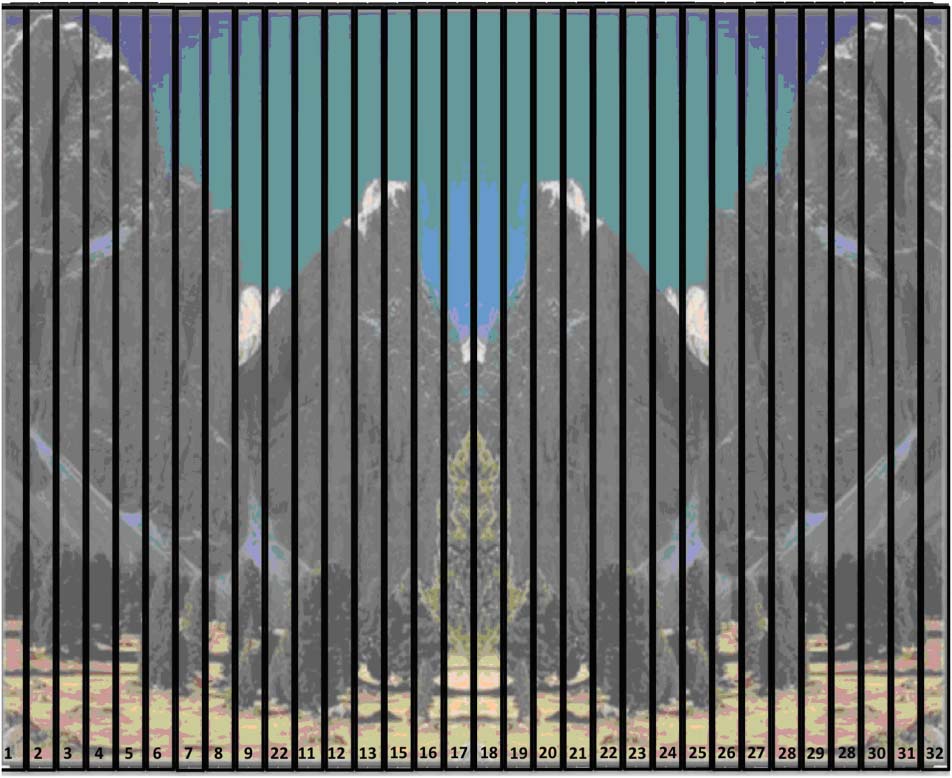
eye data were available. For analysis, the computer screen
was divided into 32 vertical areas of interest (AOIs), E
sequential numbers were assigned to these from left to
right (Figura 1). The fixation duration was summed for
each AOI. Inoltre, we subtracted the fixation dura-
tion of each AOI of the stimulation right ON/left OFF
and right OFF/left ON from the “baseline condition” right
ON/left ON and summed up these differences for the
right and left hemispaces. Saccades were analyzed for the
number of saccades, saccade amplitude, duration, peak
velocity, and acceleration peak. This was carried out sepa-
rately for left- and right-sided saccades at every stimulation
setting.
Statistical Analysis
The Wilcoxon signed-rank test was used to determine the
stimulation settings (stimulation voltage, frequency pulse
width and amplitude of the right versus left electrodes).
UPDRS total and subscores were analyzed using Kruskal–
Wallis tests on account of the nonparametric distribution
of the data. Given significant differences between stimula-
tion settings, Mann–Whitney U tests were performed for
a pairwise comparison between specific stimulation set-
tings. Recording times of the eye-tracking experiment
were analyzed using a repeated-measures ANOVA with
the within-subject factor Stimulation Setting. The fixation
duration recorded by the eye-tracker was summed for the
left (AOI 1–16) and right (AOI 17–32) hemispace for each
stimulation setting separately and then compared using
t tests for dependent samples. For a more detailed analysis
of the fixation duration in relation to each AOI, we tested
the relevance of the changes in fixation duration caused
D
o
w
N
l
o
UN
D
e
D
F
R
o
M
l
l
/
/
/
/
j
F
/
T
T
io
T
.
:
/
/
H
T
T
P
:
/
D
/
o
M
w
io
N
T
o
P
UN
R
D
C
e
.
D
S
F
io
R
o
l
M
v
e
H
R
C
P
H
UN
D
io
io
R
R
e
.
C
C
T
.
o
M
M
/
j
e
D
o
tu
C
N
o
/
C
UN
N
R
UN
T
R
io
T
io
C
C
l
e
e
–
P
–
D
P
D
2
F
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
C
7
N
3
_
5
UN
/
_
j
0
o
0
C
5
N
0
2
_
UN
P
_
D
0
0
B
5
sì
0
G
2
tu
.
e
P
S
T
D
o
F
N
B
0
sì
8
S
M
e
IO
P
T
e
M
l
io
B
B
e
R
R
UN
2
R
0
io
2
3
e
S
/
j
.
T
/
F
tu
S
e
R
o
N
1
7
M
UN
sì
2
0
2
1
Figura 1. For analysis, the computer screen was divided into
32 vertical AOIs, and sequential numbers were assigned to these
from left to right.
Schmalbach et al.
545
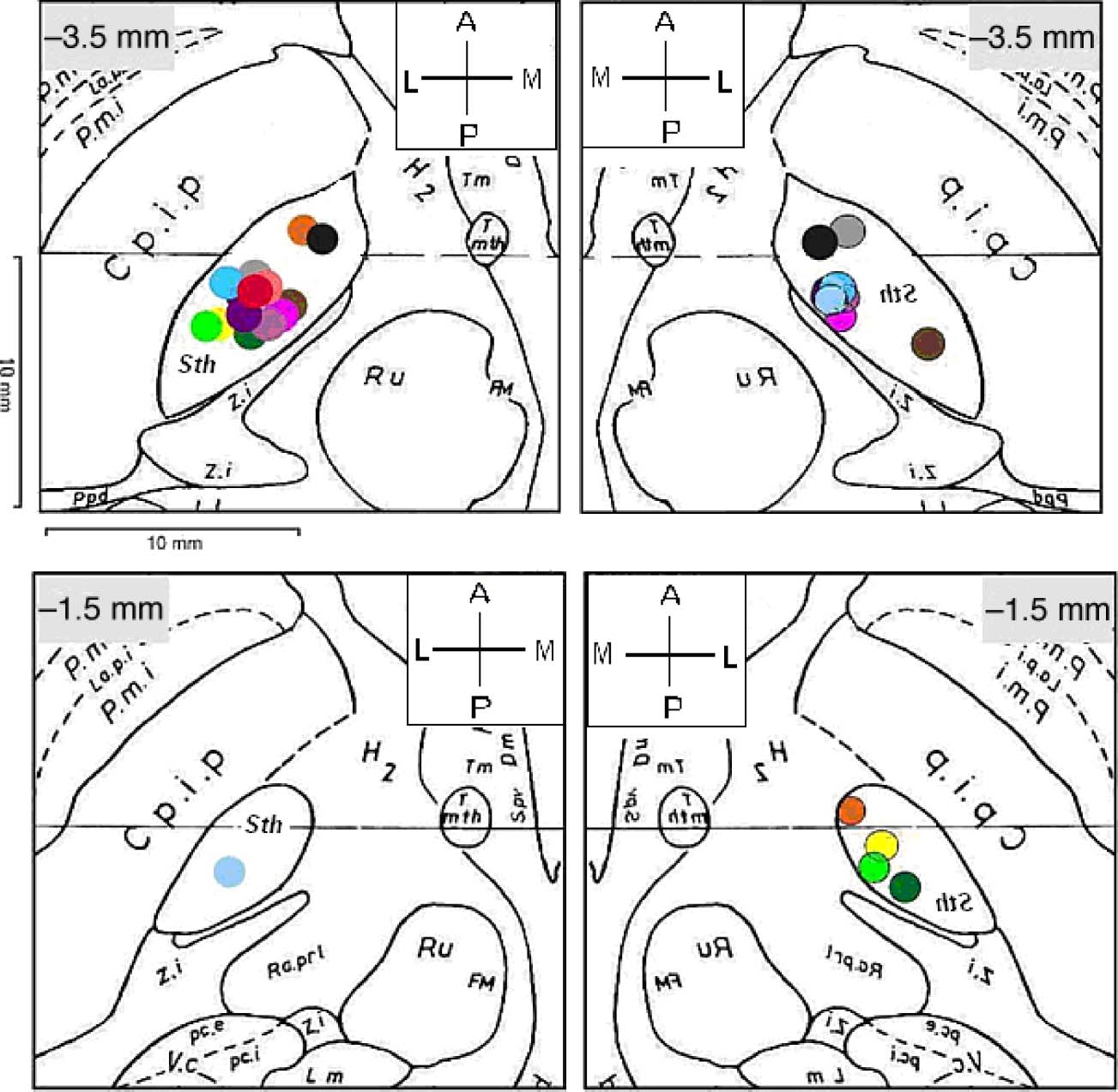
Figura 2. Schematic
representation of the location
of active electrode contacts
used for stimulation during the
study over a series of two axial
sections of the Schaltenbtand
and Wahren atlas (A = anterior;
M = medial; P = posterior;
L = lateral). Left, left brain
contacts; right, right brain
contacts. Negative numbers
on the graphs represent
millimeters inferior from
the midcommissural point.
Cp.i.p. = Crus posterior of the
internal capsula; RU = nucleus
ruber or red nucleus; Ra.
pr1 = preleminiscal radiation;
Sth = subthalamic nucleus;
V.c. = nucleus ventrocaudalis;
z.i. = zona incerta.
by changes in the stimulation setting using the reliable
change index (RCI) in every AOI. The fixation duration
in each AOI of the three conditions was summed up. IL
fixation duration of each AOI was compared between stim-
ulation settings. The RCI for the stimulation condition
right ON/left OFF was calculated using the formula RCI =
(fixation duration in the right ON/left OFF stimulation
setting − fixation duration in the right ON/left ON stimula-
tion setting)/SDdiff, where SDdiff is the standard error of
the difference score (Frerichs & Tuokko, 2006). In analogy,
RCI of the right OFF/left ON stimulation setting was cal-
culated for each AOI. Upper and lower cutoff values of
Tavolo 2. Results of the Neurological Examination (UPDRS Total and Subscores) in Three Stimulation Settings
Right ON/Left ON (n = 13) Right ON/Left OFF (n = 13) Right OFF/Left ON (n = 13) χ2
UPDRS III Total
UPDRS, righta
UPDRS, lefta
UPDRS axial
UPDRS tremor
UPDRS rigor
UPDRS akinesia
UPDRS bradykinesia
UPDRS postural instability
26.31 ± 6.54
5.77 ± 2.62
6.77 ± 3.06
13.62 ± 4.07
0.77 ± 1.36
0.77 ± 1.09c
14.08 ± 5.41
2.00 ± 0.91
6.54 ± 2.96
33.62 ± 7.38
11.77 ± 3.94b
8.69 ± 4.84b
13.46 ± 3.15
2.92 ± 3.55
3.92 ± 2.57
16.31 ± 5.48
2.00 ± 0.71
6.54 ± 1.85
33.08 ± 8.85
7.23 ± 3.06b
12.92 ± 5.22b
12.92 ± 3.84
2.92 ± 2.96
3.85 ± 2.08c
15.77 ± 5.31
2.00 ± 0.71
6.46 ± 2.40
Data are given in mean ± SD.
aSum of unilateral items of the UPDRS (Items 20–26).
bSignificant differences between stimulation setting right ON/left OFF and right OFF/left ON ( P < .03).
cSignificant differences between stimulation setting right ON/left ON and right OFF/left ON: p < .0001.
p
.068
.002
.005
.78
.094
5.36
12.71
10.51
0.50
4.73
17.32 <.001
0.96
0.05
0.12
.62
.97
.94
546
Journal of Cognitive Neuroscience
Volume 26, Number 3
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
c
7
n
3
_
5
a
/
_
j
0
o
0
c
5
n
0
2
_
a
p
_
d
0
0
b
5
y
0
g
2
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
t
/
f
.
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
1.645 or −1.645, respectively, indicated reliable change.
To avoid multiple testing, only AOIs showing a reliable
change triggered a separate t test between stimulation
settings. In addition, we subtracted the fixation duration
of each AOI of the stimulation right ON/left OFF and right
OFF/left ON from the “baseline condition” right ON/left
ON and summed up these differences for the right and
left hemispaces.
RESULTS
There was no significant difference between the stimula-
tion settings when comparing the right and left electrodes
with regard to stimulation voltage, frequency, and pulse
width (Table 1). Figure 2 shows the position of the active
electrode contacts.
Motor Score
Total UPDRS motor scores significantly improved under
STN stimulation. The unilateral items showed significant
changes in the degree of symptom asymmetry ( p < .03).
The stimulation setting right ON/left OFF significantly
improved left-sided motor functions, and the stimulation
setting right OFF/left ON significantly improved right-
sided motor functions (see Table 2).
Analysis of the Eye Recordings
Average total recording times per patient and stimulation
setting did not significantly differ between stimulation
settings (right ON/left ON: 182.3 sec; right ON/left OFF:
171.4 sec; and right OFF/left ON: 173.9 sec; one-way
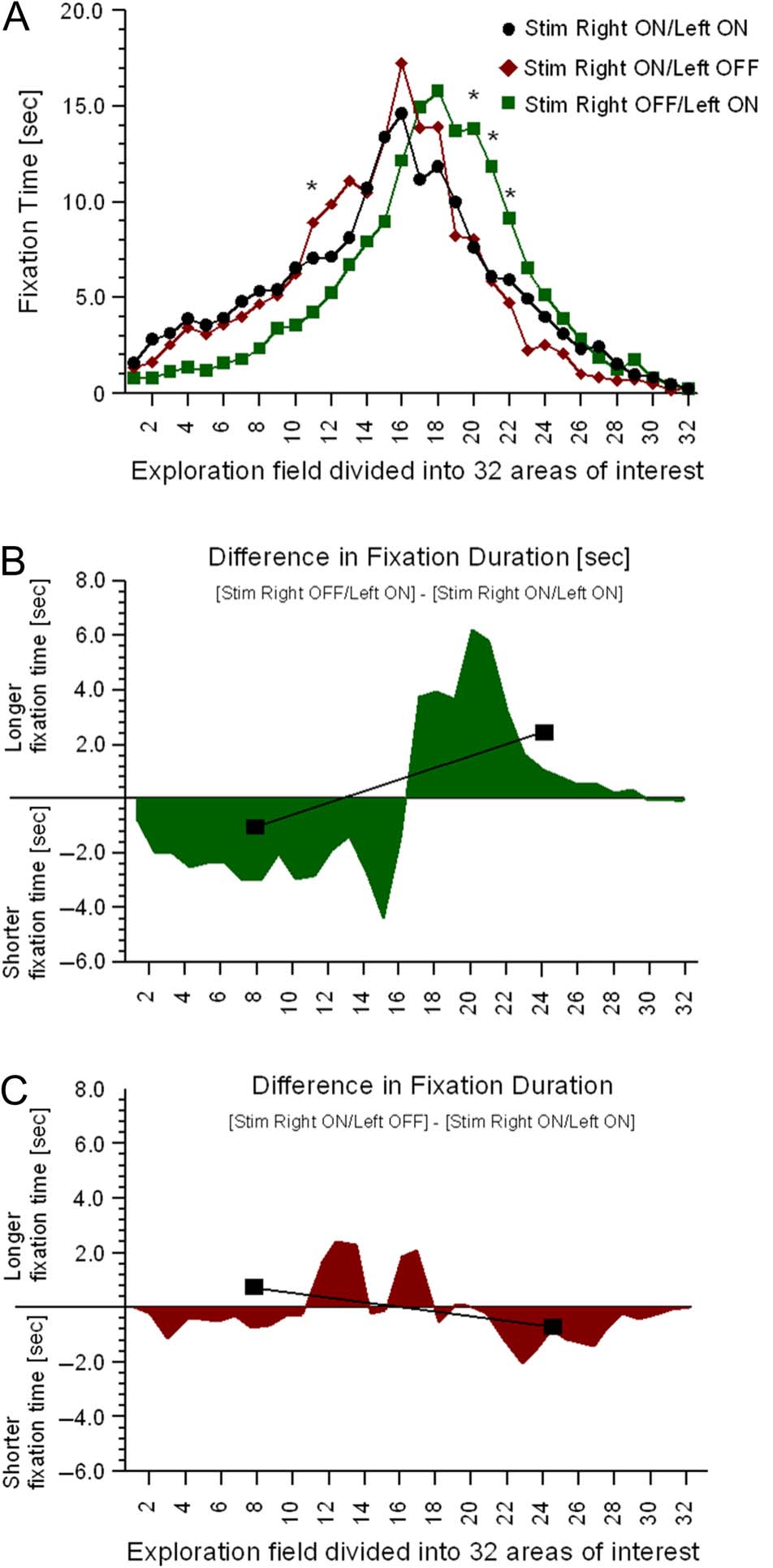
ANOVA: p > .4). Fixation durations of each stimula-
tion setting are displayed in Figure 3A. An ANOVA for
repeated-measures including the within-subject factor Time
Spent in the right or left hemispace and the within-
subject factor Stimulation Setting showed significant inter-
action effect (F = 3.6, p = .038). In the stimulation
setting right OFF/left ON, patients significantly fixated
on the left side of the hemispace for shorter periods of
time (67.3 sec, SD = 44.4 sec [area under the curve
AOI 1–16]; Figure 3A) compared with the stimulation
setting right ON/left ON (107.0 sec, SD = 40.1, t = 2.4,
p = .023) and the stimulation setting right ON/left OFF
(106.4 sec, t = 2.5, p = .019). There was a trend for longer
fixation duration in the stimulation setting right OFF/left
ON for the right hemispace (106.6 sec, SD = 60.2 [area
under the curve AOI 17–32]; Figure 3A) compared with
the stimulation setting right ON/left OFF (65.0 sec, SD =
47.8, t = −1.9, p = .06) and no significant differences
compared with the right ON/left ON setting (75.3 sec,
SD = 52.4, p > .2). RCIs greater than 1.6 existed only in
the comparison between the stimulation settings right
ON/left ON and right OFF/left ON in AOI 11, 20, 21, E
22. Post hoc analysis demonstrated significantly shorter
Figura 3. (UN) Fixation durations are illustrated for each stimulation
setting ((cid:129)= right ON/left ON stimulation; ♦ = right ON/left OFF
stimulation; ▪ = right OFF/left ON stimulation). The exploration field
is separated into 32 vertical ROIs (* displays significant differences
between unilateral right-side stimulation and unilateral left-side
stimulation). Bilateral symmetrical stimulation (right ON/left ON
stimulation) was used as the baseline condition. (B) The difference in
fixation duration between stimulation right OFF/left ON and stimulation
right ON/left ON. (C) The difference in fixation duration between right
ON/left OFF and stimulation right ON/left ON. The gray bar indicates the
difference in interaction effect of unilateral stimulation in comparison
with bilateral stimulation.
fixation duration in AOI 11 for the right OFF/left ON set-
ting and significantly longer fixation duration in AOI 20,
21, E 22 compared with the right ON/left ON stimulation
setting ( P < .05 for all comparisons; see Figure 3A).
Further analysis of the hemispace of fixation duration on
Schmalbach et al.
547
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
c
7
n
3
_
5
a
/
_
j
0
o
0
c
5
n
0
2
_
a
p
_
d
0
0
b
5
y
0
g
2
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
f
.
t
/
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
nonmirrored and mirrored pictures did not reveal any
significant differences and no RCIs more or less than 1.6.
In conclusion, patients spent less time in the left hemi-
space in the right OFF/left ON stimulation condition and
demonstrated a trend toward longer fixation duration in
the right OFF/left ON condition to the right-sided hemi-
space compared with the right ON/left OFF stimulation
condition. Using the bilateral stimulation setting right
ON/left ON as a baseline condition, both AOIs of the
right ON/left OFF and the AOI of the right OFF/left ON
condition were subtracted from the AOI of this baseline
condition (Figure 3B and C). An ANOVA including the
within-subject factor “time spent in the right or left hemi-
space” and the “within-subject factor stimulation setting”
(changes from right ON/left ON to right OFF/left ON and
right ON/left OFF) showed a significant interaction (F =
3.98, p = .048; Figure 3B and C). A t test demonstrated
significantly longer exploration of the right hemispace in
the right OFF/left ON stimulation setting (T = 3.75, p =
.03), but a nonsignificant t test in the right ON/left OFF
stimulation setting demonstrated no significant changes
from baseline (right ON/left ON). To explore the effect
of motor symptom asymmetry on visual exploration,
patients were divided into groups of patients with a right-
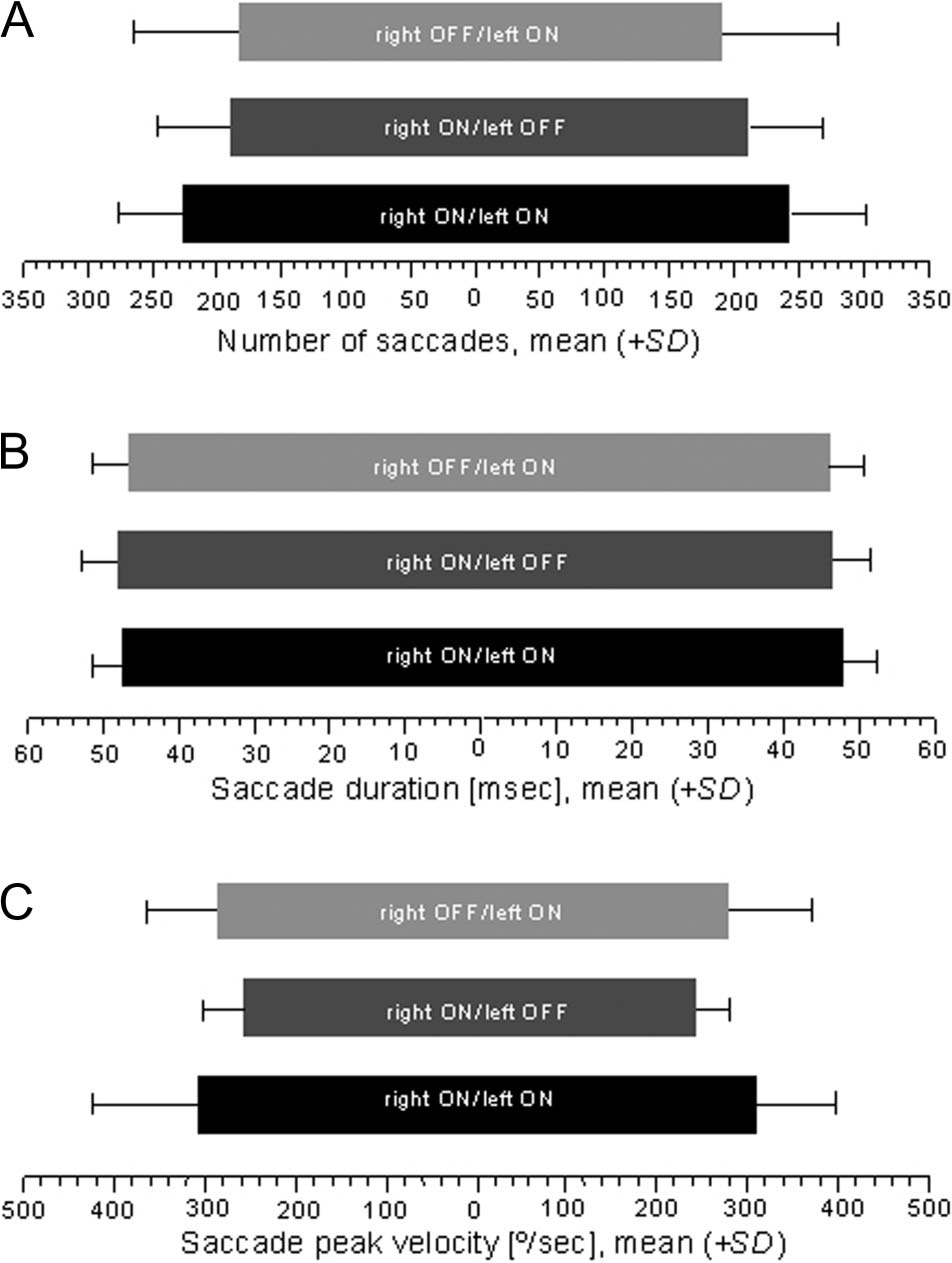
Figure 4. Saccade parameters are shown for right- and left-sided
saccades: (A) number of saccades, (B) saccade duration, and
(C) peak velocity. Data are given in mean (±SD).
lateralized or a left-lateralized symptom. An ANOVA analy-
sis included the Onset Side as between-subject variable
and the Stimulation Condition as within-subject variable
revealed no significant effect of the factor Onset Side. Sin-
gle significant differences were found between right and
left-lateralized onset of PD motor symptoms.
The Kolmogorov–Smirnov test showed a normal dis-
tribution of saccadic eye parameters (number of saccades,
saccade amplitude, duration, peak velocity, acceleration
peak). Right- and left-sided saccadic parameters were
tested using ANOVA, including the between-subject factor
Stimulation Setting. Statistical analysis did not reveal any
significant differences ( p > .11 for all comparisons; Fig-
ure 4). We furthermore correlated the changes in the
UPDRS score and changes in eye recordings (saccade
duration, amplitude, and peak velocity) and did not find
significant correlations. Inoltre, the analysis of the
subjective arousal ratings of the IAPS picture set showed
no significant differences of arousal scores related to
stimulation conditions ( p > .78).
DISCUSSION
Our patients showed a shift of spatial attention in the
right OFF/left ON stimulation setting compared with the
other stimulation settings. This imbalance in attentional
recourses in this stimulation setting includes an increase
in attention of right-sided stimuli and a reduced atten-
tion of left-sided stimuli. This imbalance in attentional
resources is also seen in patients suffering from neglect
after right hemispheral lesions (Karnath, Niemeier, &
Dichgans, 1998). Tuttavia, the magnitude of this shift is
much smaller in our patients. These results support the
role of the STN in modulating spatial attention. The right
OFF/left ON stimulation setting resembles the situation
of a unilateral nigrostriatal lesion on the right side at the
level of the BG. Switching off STN stimulation on the right
side increases BG outflow on the right and inhibits cortical
projections of the corticosubcortical loops (Limousin et al.,
1997). In parallel, the Parkinsonian signs worsened on
the left side of the body. The left-sided STN stimulation
inhibits the influence of the indirect BG pathway and
consecutively releases cortical activation. This stimulation
setting clinically resembles a left-sided hemiparkinsonism
with an imbalance in BG tone. The net effect of an increased
activation of the STN in the indirect pathway (the so-called
no-go way) is an inhibition of movements and also cogni-
tive aspects (Frank, Samanta, Moustafa, & Sherman, 2007;
Frank, 2006). The inhibitory effect of electric stimulation
of the STN inhibits the net effect of the indirect pathway
(Ballanger et al., 2009), so the direct BG pathway that
provides the “global go” is more influential ( Volkmann,
Daniels, & Witt, 2010). Switching off one side of the bilat-
eral stimulation (per esempio., right OFF/left ON), the stimulation
ON condition of the left side partially restores BG func-
tion and the OFF condition on the right side does not
influence the pathological changes of the BG circuits
548
Journal of Cognitive Neuroscience
Volume 26, Numero 3
D
o
w
N
l
o
UN
D
e
D
F
R
o
M
l
l
/
/
/
/
j
F
/
T
T
io
T
.
:
/
/
H
T
T
P
:
/
D
/
o
M
w
io
N
T
o
P
UN
R
D
C
e
.
D
S
F
io
R
o
l
M
v
e
H
R
C
P
H
UN
D
io
io
R
R
e
.
C
C
T
.
o
M
M
/
j
e
D
o
tu
C
N
o
/
C
UN
N
R
UN
T
R
io
T
io
C
C
l
e
e
–
P
–
D
P
D
2
F
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
C
7
N
3
_
5
UN
/
_
j
0
o
0
C
5
N
0
2
_
UN
P
_
D
0
0
B
5
sì
0
G
2
tu
.
e
P
S
T
D
o
F
N
B
0
sì
8
S
M
e
IO
P
T
e
M
l
io
B
B
e
R
R
UN
2
R
0
io
2
3
e
S
/
j
T
F
/
.
tu
S
e
R
o
N
1
7
M
UN
sì
2
0
2
1
(neglecting a small lesion effect of the electrode in the
STN area; Mann et al., 2009). The result of a decrease in
exploration time of the left hemispace in the right OFF/
left ON condition can be interpreted in such a way that
switching off the right stimulator critically affects the atten-
tional system of the right hemisphere. So the stimulated
left side might be less important for this bias in explora-
zione. The reduced visuospatial attention of left-sided space
in the unilateral left-sided stimulation setting is in line with
previous studies demonstrating mild signs and symptoms of
reduced visuospatial attention in left-sided hemiparkinson
patients and, hence, in patients with a pathology in the
right BG (Ebersbach et al., 1996). Our results further show
that by switching on the stimulation of the right STN,
symptoms of reduced visuospatial attention vanished. Questo
finding indicates that the right STN is part of the network
subserving spatial attention.
Signs and symptoms of neglect can be found after right
and left hemispheric damage, but right-sided neglect
after left hemispheric damage is often mild and lasts only
a short time, which might explain the lack of reduced
visuospatial attention after unilateral right-sided STN stim-
ulation in our eye-tracking experiment. The right hemi-
spheric dominance of the attentional system might be
the consequence of hemispheric specialization after
language development.
An STN lesion might influence spatial orientation in two
principal ways: The STN has efferents to the putamen and
the head of the caudate nucleus, which are subcortical
structures that are involved in perceptual spatial orienta-
tion in humans (Karnath et al., 2002). Damage to these
structures in the right hemisphere can lead to consider-
able signs and symptoms of neglect. Inoltre, IL
STN might influence spatial orientation via projections to
the ACC of the right hemisphere. Imaging studies exam-
ining visual attention showed an activation of the right
anterior cingulate gyrus, the intraparietal sulcus of the
right posterior parietal cortex, and the mesial and lateral
premotor cortices (Nobre et al., 1997). The STN is con-
nected to the ACC by means of subcortico-cortical circuits
(Hamani, Saint-Cyr, Fraser, Kaplitt, & Lozano, 2004). STN-
DBS seems to modulate ACC activity in a task-specific
maniera (Schroeder et al., 2002; Limousin et al., 1997).
Apart from an influence on motor function and spatial
orientation, the STN, as the BG in general, also has an
impact on oculomotor functions, as animal studies have
revealed (Nambu, Takada, Inase, & Tokuno, 1996). IL
clinical relevance is that PD patients have deficits in the
initiation of voluntary saccades, their memory-guided
saccades are hypometric, and latencies and error rates of
antisaccades are increased (Vermersch et al., 1994). STN-
DBS can positively influence the initiation of both reflexive
and volitional saccades in PD (Yugeta et al., 2010). Further-
more, unilateral right or left STN-DBS has been known to
induce contralateral gaze deviation (Sauleau et al., 2008).
Tuttavia, three facts argue against the assumption that
our results are the effect of an alteration in the oculomotor
system. Primo, conjungate eye deviations after unilateral
STN stimulation were not detected in our patients on
clinical evaluation in the different stimulation settings.
Secondo, the analysis of the number, duration, amplitude,
peak velocity, and acceleration peak of saccades did not
reveal any significant differences between the stimulation
settings. Third, we did not find any significant correlation
between the changes in the UPDRS scores and changes
in eye recordings. Inoltre, if unilateral right or left STN
stimulation produced an imbalance in the oculomotor
system leading to a contralateral ocular deviation, a change
in visual exploration behavior should be detectable in
both the right OFF/left ON and in the rightON/left OFF
stimulation setting. In our patients, Tuttavia, an asym-
metry in visual attention was detected after left-sided
stimulation. Testing patients in an ON medication condi-
zione, we also have to discuss possible masking effects that
might explain differences between oculomotor changes
as reported by others ( Yugeta et al., 2010). Tuttavia,
previous studies examined the oculomotor changes after
unilateral STN-DBS using a memory-guided saccade de-
sign, whereas our study examined free exploration of pic-
tures, which might also explain the differences between
our results and the results of previous studies.
There are two major limitations in our study. Patients
were not tested in a stimulation condition in which both
electrodes were turned off (right OFF/left OFF) as a con-
trol situation. Nor were they tested after a withdrawal of
dopaminergic medication. Both conditions would have
been very difficult for the patients to tolerate because
of severe motor symptoms. Consequently, it would not
only have limited recruitment but also have influenced
the results because most patients would not have been
able to finish the test battery. Tuttavia, these limitations
do not attenuate the gist of our study, demonstrating the
impact of the STN on space orientation.
In conclusion, our results prove earlier assumptions
that unilateral STN-DBS leads to a disturbance in the ex-
ploratory component of spatial orientation and therefore
changes exploration behavior in space. These changes
in visuospatial attention are rather small but detectable
when analyzing visual exploration behavior.
Ringraziamenti
This work was supported by an intramural grant of the Christian
Albrecht University Kiel.
Reprint requests should be sent to Karsten Witt, Department of
Neurology, Universitätsklinikum Schleswig-Holstein, Città universitaria
Kiel, Arnold-Heller-Strasse 3, Haus 41, 24105 Kiel, Germany, O
via e-mail: k.witt@neurologie.uni-kiel.de.
REFERENCES
Ballanger, B., van Eimeren, T., Moro, E., Lozano, UN. M.,
Hamani, C., Boulinguez, P., et al. (2009). Stimulation of
the subthalamic nucleus and impulsivity: Release your
horses. Annals of Neurology, 66, 817–824.
Schmalbach et al.
549
D
o
w
N
l
o
UN
D
e
D
F
R
o
M
l
l
/
/
/
/
j
F
/
T
T
io
T
.
:
/
/
H
T
T
P
:
/
D
/
o
M
w
io
N
T
o
P
UN
R
D
C
e
.
D
S
F
io
R
o
l
M
v
e
H
R
C
P
H
UN
D
io
io
R
R
e
.
C
C
T
.
o
M
M
/
j
e
D
o
tu
C
N
o
/
C
UN
N
R
UN
T
R
io
T
io
C
C
l
e
e
–
P
–
D
P
D
2
F
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
C
7
N
3
_
5
UN
/
_
j
0
o
0
C
5
N
0
2
_
UN
P
_
D
0
0
B
5
sì
0
G
2
tu
.
e
P
S
T
D
o
F
N
B
0
sì
8
S
M
e
IO
P
T
e
M
l
io
B
B
e
R
R
UN
2
R
0
io
2
3
e
S
/
j
.
/
F
T
tu
S
e
R
o
N
1
7
M
UN
sì
2
0
2
1
Bergman, H., Wichmann, T., & DeLong, M. R. (1990).
Reversal of experimental parkinsonism by lesions of
the subthalamic nucleus. Scienza, 249, 1436–1438.
Committeri, G., Pitzalis, S., Galati, G., Patria, F., Pelle, G.,
Sabatini, U., et al. (2007). Neural bases of personal and
extrapersonal neglect in humans. Brain, 130, 431–441.
Deuschl, G., Schade-Brittinger, C., Krack, P., Volkmann, J.,
Schafer, H., Botzel, K., et al. (2006). A randomized trial
of deep-brain stimulation for Parkinsonʼs disease.
The New England Journal of Medicine, 355, 896–908.
Ebersbach, G., Trottenberg, T., Hattig, H., Schelosky, L.,
Schrag, A., & Poewe, W. (1996). Directional bias of initial
visual exploration. A symptom of neglect in Parkinsonʼs
disease. Brain, 119, 79–87.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975).
“Mini-mental state.” A practical method for grading the
cognitive state of patients for the clinician. Journal of
Psychiatric Research, 12, 189–198.
Frank, M. J. (2006). Hold your horses: A dynamic computational
role for the subthalamic nucleus in decision making.
Neural Networks, 19, 1120–1136.
Frank, M. J., Samanta, J., Moustafa, UN. A., & Sherman, S. J.
(2007). Hold your horses: Impulsivity, deep brain
stimulation, and medication in parkinsonism. Scienza,
318, 1309–1312.
Frerichs, R. J., & Tuokko, H. UN. (2006). Reliable change
scores and their relation to perceived change in memory:
Implications for the diagnosis of mild cognitive impairment.
Archives of Clinical Neuropsychology, 21, 109–115.
Hamani, C., Saint-Cyr, J. A., Fraser, J., Kaplitt, M., & Lozano,
UN. M. (2004). The subthalamic nucleus in the context of
movement disorders. Brain, 127, 4–20.
Hughes, UN. J., Daniel, S. E., Kilford, L., & Lees, UN. J. (1992).
Accuracy of clinical diagnosis of idiopathic Parkinsonʼs
disease: A clinico-pathological study of 100 cases. Journal
of Neurology, Neurosurgery and Psychiatry, 55, 181–184.
Karnath, H. O., Ferber, S., & Himmelbach, M. (2001). Spatial
awareness is a function of the temporal not the posterior
parietal lobe. Nature, 411, 950–953.
Karnath, H. O., Himmelbach, M., & Rorden, C. (2002). IL
subcortical anatomy of human spatial neglect: Putamen,
caudate nucleus and pulvinar. Brain, 125, 350–360.
Karnath, H. O., Niemeier, M., & Dichgans, J. (1998). Spazio
exploration in neglect. Brain, 121, 2357–2367.
Karnath, H. O., Rennig, J., Johannsen, L., & Rorden, C.
(2011). The anatomy underlying acute versus chronic
spatial neglect: A longitudinal study. Brain, 134, 903–912.
Lang, P. J., Bradley, M. M., & Cuthbert, B. N. (2008). Internazionale
Affective Picture System (IPAS): Instructions manual and
affective ratings. Technical Report A-8. Gainesville: University of
Florida.
Limousin, P., Greene, J., Pollak, P., Rothwell, J., Benabid,
UN. L., & Frackowiak, R. (1997). Changes in cerebral activity
pattern due to subthalamic nucleus or internal pallidum
stimulation in Parkinsonʼs disease. Annals of Neurology,
42, 283–291.
Mann, J. M., Foote, K. D., Garvan, C. W., Fernandez, H. H.,
Jacobson, C. E. T., Rodriguez, R. L., et al. (2009). Brain
penetration effects of microelectrodes and DBS leads
in STN or GPi. Journal of Neurology, Neurosurgery,
and Psychiatry, 80, 794–797.
Mort, D. J., Malhotra, P., Mannan, S. K., Rorden, C., Pambakian, A.,
Kennard, C., et al. (2003). The anatomy of visual neglect.
Brain, 126, 1986–1997.
Nambu, A., Takada, M., Inase, M., & Tokuno, H. (1996). Dual
somatotopical representations in the primate subthalamic
nucleus: Evidence for ordered but reversed body-map
transformations from the primary motor cortex and the
supplementary motor area. Journal of Neuroscience, 16,
2671–2683.
Nobre, UN. C., Sebestyen, G. N., Gitelman, D. R., Mesulam,
M. M., Frackowiak, R. S., & Frith, C. D. (1997). Functional
localization of the system for visuospatial attention using
positron emission tomography. Brain, 120, 515–533.
Sauleau, P., Pollak, P., Krack, P., Courjon, J. H., Vighetto, A.,
Benabid, UN. L., et al. (2008). Subthalamic stimulation
improves orienting gaze movements in Parkinsonʼs
disease. Clinical Neurophysiology, 119, 1857–1863.
Schaltenbrand, G., & Wahren, W. (1977). Atlas of stereotaxy
of the human brain. Stuttgart: Thieme.
Schrader, B., Hamel, W., Weinert, D., & Mehdorn, H. M.
(2002). Documentation of electrode localisation.
Movement Disorders, 17(Suppl. 3), 167–174.
Schroeder, U., Kuehler, A., Haslinger, B., Erhard, P.,
Fogel, W., Tronnier, V. M., et al. (2002). Subthalamic
nucleus stimulation affects striato-anterior cingulate
cortex circuit in a response conflict task: A PET study.
Brain, 125, 1995–2004.
Vermersch, UN. I., Rivaud, S., Vidailhet, M., Bonnet, UN. M.,
Gaymard, B., Agid, Y., et al. (1994). Sequences of
memory-guided saccades in Parkinsonʼs disease [Research
Supporto, Non-U.S. Govʼt]. Annals of Neurology, 35, 487–490.
Volkmann, J., Daniels, C., & Witt, K. (2010). Neuropsychiatric
effects of subthalamic neurostimulation in Parkinson
disease. Nature Reviews Neurology, 6, 487–498.
Witt, K., Kopper, F., Deuschl, G., & Krack, P. (2006).
Subthalamic nucleus influences spatial orientation in
extra-personal space. Movement Disorders, 21, 354–361.
Yugeta, A., Terao, Y., Fukuda, H., Hikosaka, O., Yokochi, F.,
Okiyama, R., et al. (2010). Effects of STN stimulation on
the initiation and inhibition of saccade in Parkinson
disease. Neurology, 74, 743–748.
550
Journal of Cognitive Neuroscience
Volume 26, Numero 3
D
o
w
N
l
o
UN
D
e
D
F
R
o
M
l
l
/
/
/
/
j
F
/
T
T
io
T
.
:
/
/
H
T
T
P
:
/
D
/
o
M
w
io
N
T
o
P
UN
R
D
C
e
.
D
S
F
io
R
o
l
M
v
e
H
R
C
P
H
UN
D
io
io
R
R
e
.
C
C
T
.
o
M
M
/
j
e
D
o
tu
C
N
o
/
C
UN
N
R
UN
T
R
io
T
io
C
C
l
e
e
–
P
–
D
P
D
2
F
6
/
3
2
6
5
/
4
3
3
/
1
5
9
4
4
3
6
/
8
1
1
7
2
8
o
0
C
7
N
3
_
5
UN
/
_
j
0
o
0
C
5
N
0
2
_
UN
P
_
D
0
0
B
5
sì
0
G
2
tu
.
e
P
S
T
D
o
F
N
B
0
sì
8
S
M
e
IO
P
T
e
M
l
io
B
B
e
R
R
UN
2
R
0
io
2
3
e
S
/
j
T
.
F
/
tu
S
e
R
o
N
1
7
M
UN
sì
2
0
2
1