研究
植入颅内电极不影响
附近或地区的尖峰或网络连接
连接的大脑区域
艾琳·C. 康拉德1, 拉塞尔·T. 筱原2,3,4, 詹姆斯·J. 古格1, 安德鲁·Y. 雷维尔5, 三地达斯 1,
乔尔·M. 斯坦6, 埃里克·D. 沼泽1,7, 凯瑟琳A. 戴维斯1*, 和布莱恩·利特1*
1神经内科, 宾夕法尼亚大学, 费城, PA, 美国
2生物统计学系, 流行病学, 和信息学, 宾夕法尼亚大学, 费城, PA, 美国
3宾夕法尼亚大学成像与可视化统计中心, 宾夕法尼亚大学, 费城, PA, 美国
4生物医学图像计算与分析中心, 宾夕法尼亚大学, 费城, PA, 美国
5医学科学家培训计划, 宾夕法尼亚大学, 费城, PA, 美国
6放射科, 宾夕法尼亚大学, 费城, PA, 美国
7儿童神经内科, 费城儿童医院, 费城, PA, 美国
*这些作者的贡献同等.
关键词: 颅内脑电图, 耐药性癫痫, 电极植入, 发作间期尖峰,
功能网络
抽象的
确定植入电极对附近和周围的电图特征的影响
耐药性癫痫患者的大脑区域相连, 我们分析了颅内脑电图
录音来自 10 接受种植修复的耐药性癫痫患者
(放置额外的电极) 在他们住院期间. 我们进行了自动化
尖峰检测和测量的脑电图功能网络. 我们分析了原始电极
在整个脑电图记录过程中保持不变, 我们测量了变化
这些原始电极响应植入的峰值速率和网络连接
新电极. 之前的总体峰值率没有变化- 种植后修复 (t (9) =
0.1, p = 0.95). 尖峰率和连接性分布的围修订变化
电极不大于机会 (蒙特卡罗法, 尖峰: p = 0.40, 连接性:
p = 0.42). 更接近或更多功能连接到修订部位的电极没有更大的
与距离较远或连接较少的电极相比,尖峰率或连接性发生变化. 变化
电极植入周围的电图特征不大于基线
整个颅内记录中发生的波动. 这些发现反对
植入对附近或相连大脑区域的尖峰或网络连接的影响.
作者总结
我们测试了植入颅内电极是否影响发作间期尖峰率或
现有电极的功能连接. 我们发现电图的变化
电极植入后的特征波动不大于基线波动
发生在整个颅内记录中. 我们的结果反对植入效应
附近或相连大脑区域的尖峰或网络连接.
开放访问
杂志
引文: 康拉德, 乙. C。, 筱原,
右. T。, 古格, J. J。, 雷维尔, A. Y。, 这,
S。, 斯坦因, J. M。, 沼泽, 乙. D ., 戴维斯,
K. A。, & 一点, 乙. (2022). 植入
颅内电极不影响
尖峰或网络连接
附近或相连的大脑区域.
网络神经科学, 6(3), 834–849.
https://doi.org/10.1162/netn_a_00248
DOI:
https://doi.org/10.1162/netn_a_00248
支持信息:
https://doi.org/10.1162/netn_a_00248;
https://github.com/erinconrad
/发作间期集线器/树/主要
/植入分析
已收到: 8 十二月 2021
公认: 1 四月 2022
通讯作者:
艾琳·C. 康拉德
erin.conrad2@pennmedicine
.宾夕法尼亚大学
处理编辑器:
莎拉·马尔登
版权: © 2022
麻省理工学院
在知识共享下发布
归因 4.0 国际的
(抄送 4.0) 执照
麻省理工学院出版社
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
/
t
/
e
d
你
n
e
n
A
r
t
我
C
e
–
p
d
我
F
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
A
_
0
0
2
4
8
p
d
.
t
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
测试植入效果
介绍
耐药性癫痫患者 (分布式RE) 可能受益于手术或神经刺激
(法语, 2007; 关等人。, 2011; 维贝等人。, 1999). 颅内脑电图 (脑电图) 监控是
用于指导这些患者的手术计划. 这个过程涉及到颅内植入
电极,然后记录脑电图几天到几周,以评估电临床
癫痫发作的特征以及发作间期活动. 对人类和动物的研究表明
植入电极会产生组织学变化,可能会影响尖峰率和其他大脑
网络特性 (刘等人。, 1999; 莫雷尔, 2011; 波利科夫等人。, 2005; D. A. 孙等人。, 2008;
F. 时间. 孙等人。, 2018; 翁等人。, 2017; 范库伊克等人。, 2007). 临床报告提出了反对意见-
欧洲核子研究中心认为,这种“植入效应”可能会立即开始,并可能影响我们定位的能力
使用颅内记录的癫痫发作发生器 (丰塔斯等人。, 2004; 卡塔里瓦拉等人。, 2001;
科瓦奇等人。, 2014; 罗斯等人。, 2012; 舒尔茨-邦哈格等人。, 2010). 我们的理解
电极植入对脑电图特征的影响受到以下事实的限制:
研究这种效应——颅内电极——与被认为引起这种效应的物质是相同的. 其他
字, 我们无法测量植入前 IEEG 基线.
颅内记录的风险之一是重要大脑区域的采样不足. 为了纠正这个问题,
少数患者在住院期间接受种植修复, 其中阿迪-
植入电极是为了解决最初植入记录中出现的假设-
英格斯 (李等人。, 2014). 这些案例提供了在之前观察 IEEG 的独特机会
植入额外的电极后. 这里我们分析数据来自 10 DRE患者
在术前 IEEG 记录过程中接受种植体修复的患者. 我们测量
发作间期尖峰和功能连接. 我们测量脑电图特征与之前相比的变化-
对整个记录中存在的原始电极进行植入后修正.
下一个, 检验电极植入影响附近或相连大脑的假设
地区, 我们确定是否存在更大的预- 植入后脑电图特征的变化
位于距离种植体修复部位更近或更功能性连接的电极上.
结果
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
/
t
/
e
d
你
n
e
n
A
r
t
我
C
e
–
p
d
我
F
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
A
_
0
0
2
4
8
p
d
.
t
原来的 16 研究的患者, 六名患者在峰值验证步骤中被排除 (五
检测器精度差, 以及一个用于稀疏尖峰的). 患者有异质种植体修复-
目标, 抗癫痫药物 (先进制造商) 变化, 癫痫发作定位, 以及其他临床
数据 (桌子 1). 总脑电图记录的平均持续时间为 16.6 天 (范围 13–26). 一个
平均数 165,061 检测到尖峰 (范围 33,366–364,955; 支持表S1
信息). 跨患者, 最接近修正部位的原始电极平均为
7.4 (标清 6.4) mm距修订站点.
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
与修订地点的接近度的不同衡量标准彼此一致
我们检查了代表不同 Prox 度量的三个变量之间的相关性-
与修正电极的相似性. 对于我们测量的每个原始电极 (A) 到它的距离
最近的修正电极, (乙) 共同尖峰指数 (原始电上的尖峰百分比-
与修改后的电极之一同时出现在时间上非常接近的电极), 和 (C) 这
功能连接 (平均 EEG Pearson 相关系数与修正后的 elec-
特罗德斯). 跨患者, 距离与共尖峰指数呈负相关
(平均值 r = −0.52, 个体患者 Fisher’s r 的 t 检验- 到 z 变换的相关系数:
t(9) = -8.70, p < 0.001). There was also a negative correlation between distance and func-
tional connectivity (mean r = −0.37, t(9) = −4.78, p = 0.001), and a positive correlation
between co-spike index and functional connectivity (mean r = 0.42, t(9) = 3.50, p = 0.007)
Co-spike index:
The proportion of spikes in a given
original electrode that co-occurred
within 50 ms on any revised
electrode. The tendency for original
electrodes to have spikes occur
simultaneously with those on revised
electrodes.
Network Neuroscience
835
t
N
e
w
o
r
k
N
e
u
r
o
s
c
e
n
c
e
i
ID Sex Age
F
1
Revision target
20 Mesial temporal,
peri-lesional
Table 1.
Clinical information.
Peri-revision
ASM changes
Full restart
Seizure localization
Peri-lesional w/
temporal spread
Seizure onset in
added electrodes
Yes
Surgery
ATL
2-year
ILAE
Class 2
Complications
Subdural hematoma
with first implant
42 Multiple frontal
No change
Unclear
No
None
N/A
None
F
F
F
F
F
2
3
4
5
6
7
8
9
10
targets, occipital
(continued
home ASMs)
40
Parietal
Partial restart
Parietal w/
61
Parietal, temporal
neocortical
Paused wean
temporal spread
Temporal neocortical
w/ diffuse spread
46
Inferior frontal,
Full restart
Perisylvian eloquent
temporal neocortical
cortex
57
Amygdala, cingulate,
insula, orbitofrontal
Full restart
Mesial temporal
and orbitofrontal
M
33
Peri-lesional
Partial restart
Diffuse hemispheric
M
42
Peri-lesional
No change
Mesial temporal
(off all ASMs)
and peri-lesional
F
F
37
Temporal neocortical
Partial restart
Mesial temporal
40
Peri-lesional
Continued
wean
Unknown
Yes
Yes
Yes
Yes
No
Yes
No
No
ATL
Class 1
RNS
Class 4
Temporal
ablation
RNS
DBS
Class 5
Class 4
Recent
surgery
None
N/A
Temporal
ablation
Recent
surgery
DBS
Recent
surgery
None
None
None
None
None
None
None
None
Abbreviations: F = female, M = male. ASM = anti-seizure medication. ATL = anterior temporal lobectomy, RNS = responsive neurostimulation, DBS = deep brain stimulation. ILAE =
International League Against Epilepsy.
8
3
6
T
e
s
t
i
n
g
t
h
e
i
m
p
l
a
n
t
e
f
f
e
c
t
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
(Figure 1). This implies that original electrodes closer to the site of implant revision are more
connected to the new electrodes as measured by Pearson correlation and co-spiking. This
finding also provides additional validation of the automated spike detections and functional
connectivity measurements.
There Is No Consistent Change in Spike Rate Within the Implantation
We compared spike rates between the early and late periods of both the first and second
implant (Figure 2). There was no difference in spike rates between the early and late stage
of the original electrodes in the first implant (Early M = 1.0 spikes/electrode/min, SD = 1.1;
Late M = 1.0 (0.9), t(9) = 0.1, p = 0.90), of the original electrodes in the second implant (Early
M = 1.0, SD = 1.0; Late M = 0.6 (0.4), t(9) = 1.0, p = 0.32), or of the added electrodes in the
second implant (Early M = 0.5, SD = 0.6; Late M = 0.3 (0.2), t(9) = 1.3, p = 0.23). There was
also no difference in the early to late relative spike rate change between the original electrodes
in the first versus the second implant (first relative change M = 0.6, SD = 1.3; second relative
change M = 0.5, SD = 1.7; t(9) = 0.04, p = 0.97) or between the original electrodes and the
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
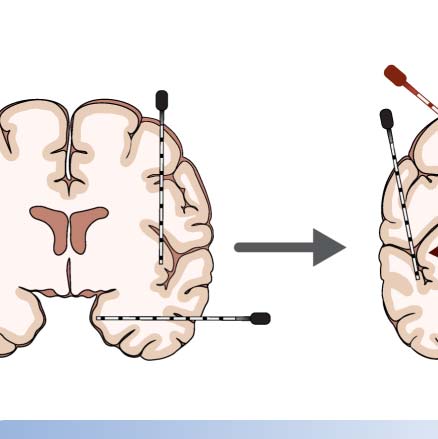
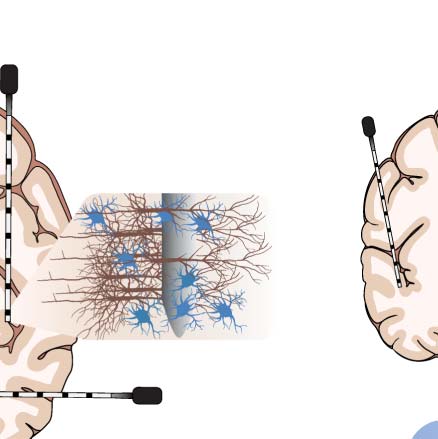
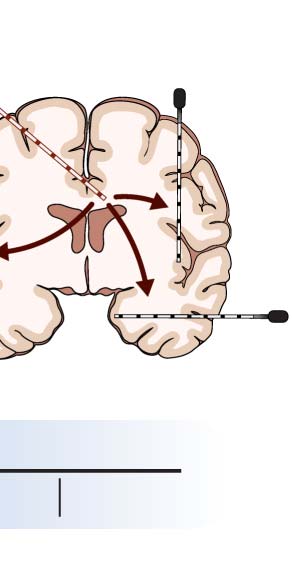
Figure 1. Study approach and concordance between different measures of proximity to the revision site. (A) Conceptual diagram demon-
strating reported effects of implanting intracranial electrodes, including local injury, hemorrhage, and non-habitual seizures. (B) Conceptual
diagram describing our study’s approach. We examined patients who underwent intracranial implantation and subsequently had new elec-
trodes placed. We examined the relative change in the electrographic features on the old electrodes in response to implanting new electrodes.
(C–H) Concordance between measures of proximity to the revision site. C–E show results for a single patient (Patient 1) as an example. F–H
show aggregate results across patients. (C, F) The correlation between distance from the nearest added electrode and the co-spike index. (D, G)
The correlation between distance from the nearest added electrode and functional connectivity to the added electrodes. (E, H) The correlation
between functional connectivity to the added electrodes and co-spike index. For subfigures C–E, each circle represents the values for a single
original electrode in the example patient. For subfigures F–H, each circle is the Pearson correlation coefficient for a single patient, and error
bars represent the 95% confidence intervals on the correlation coefficient (obtained by bootstrapping with 10,000 iterations). The p value is
that from a two-sided t test testing whether the Fisher r- to z-transformed correlation coefficients across patients were significantly different
from 0.
Network Neuroscience
837
Testing the implant effect
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
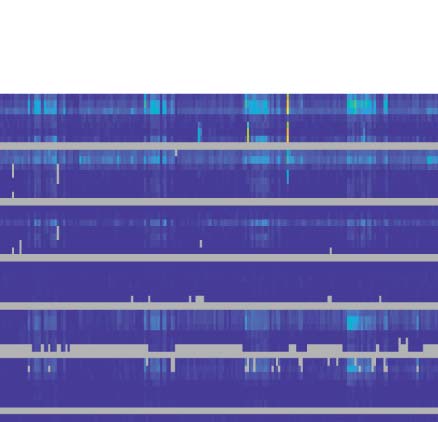
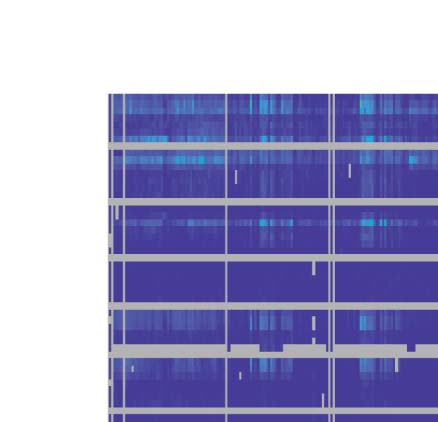
Figure 2. Spike rates across time within the implant. (A) Raster plot showing the spike rate across original electrodes at different times for an
example patient (Patient 5). Gray periods are periods of automatically detected disconnection or severe electrode artifact. The vertical maroon
dotted line shows the time of the implant revision. The precise time of the implant revision during the period of disconnection is unknown.
Horizontal bars above the graph show the time periods defined as Early Implant 1, Late Implant 1, Early Implant 2, and Late Implant 2. (B) The
change in spike rate from early in the implant to late in the implant for both implants. Each line represents data for a single patient. The line
connects the average spike rate in the early period to that in the late period. The leftmost set of lines represents the original electrodes in the
first implantation. The middle lines represent the original electrodes in the second implantation. The rightmost lines represent the added elec-
trodes in the second implantation. There was no consistent change in spike rates between the early and late period for any set of electrodes.
Also, there was no difference in the relative early to late spike rate change between the first and second implantation, or between the original
and added electrodes in the second implantation. (C) The correlation between the early to late period time difference and the relative spike rate
change. The leftmost plot shows data for Implant 1, the middle plot shows the original electrodes from Implant 2, and the rightmost plot shows
the added electrodes from Implant 2. There was no correlation between the early to late time difference and the relative spike rate change for
either implant.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
added electrodes in the second implant period (original electrodes relative change M = 0.5,
SD = 1.7; added electrodes relative change M = −0.0, SD = 0.8; t(9) = −1.0, p = 0.33). This
was also true for each tested duration ranging from 3 to 60 hr defining the early and late
periods (Table S2 in the Supporting Information). There was no correlation between the early
to late duration and the relative spike rate change for the first implant (ρ = 0.05, p = 0.89), the
Network Neuroscience
838
Testing the implant effect
Spike stability:
Spearman rank correlation between
the pre- and post-revision spike rate
distribution. The agreement between
the distribution of spike rates across
electrodes pre- to post-revision
(higher spike stability → less peri-
revision change).
Spike rate distribution:
Vector containing the average spike
rate of each electrode. The
distribution of spike rates across
electrodes.
Node strength stability:
Spearman rank correlation between
the pre- and post-revision
connectivity distribution. The
agreement between the distribution
of connectivity across electrodes pre-
to post-revision (higher node strength
stability → less peri-revision change).
Node strength:
Sum of the Pearson correlation
coefficients between the EEG signal
on a given electrode and the EEG
signals on all other electrodes. A
measure of overall connection
strength for a given electrode (higher
node strength → more connected).
Network Neuroscience
original electrodes in the second implant (ρ = −0.21, p = 0.56), or the added electrodes in the
second implant (ρ = 0.07, p = 0.86). These results imply that (a) there is no consistent change
in spike rates within either implantation, (b) the post-implantation change in spike rates is sim-
ilar between the two implants, and (c) the post-revision change in spike rates is similar
between newly added electrodes and those electrodes already in place.
Overall Spike Rate Does Not Change Surrounding Electrode Implantation
We next compared the overall spike rate between the pre- and post-revision period. No indi-
vidual patient had a larger peri-revision change in overall spike rates than expected at ran-
domly chosen time periods (Monte Carlo test with Bonferroni correction). Patient 3, who
was the only patient in whom a grid electrode configuration was added, had the largest
peri-revision spike rate change (1.1 → 3.5 spikes/electrode/min), although the Monte Carlo
analysis was not significant after Bonferroni correction (p = 0.02, α = 0.005). There was no
consistent difference across patients between the pre-revision (M = 1.0, SD = 0.9
spikes/electrode/min) and post-revision (M = 1.0, SD = 1.0 spikes/electrode/min) spike rate
(t(9) = 0.1, p = 0.95) (Figure 3B). There was also no consistent peri-revision change in spike
rate seen using any other peri-revision duration ranging from 6 to 120 hours (Table S3 in the
Supporting Information, Bonferroni correction).
The Pre- to Post-Implant Change in the Distribution of Electrographic Features Across Electrodes Is No
Larger Than Chance
We measured the peri-revision spike stability, defined as the Spearman rank correlation
between the pre- and post-revision spike rate distribution across electrodes (Figures 3C–3F).
The spike stabilities for all individual patients and aggregated across patients (M = 0.76, SD =
0.19) were no different from chance (Monte Carlo with Fisher’s method: p = 0.40). The node
strength stability (M = 0.75, SD = 0.21) was also no different from chance ( p = 0.42). The same
findings were observed examining other peri-revision interval durations (Table S3 in the
Supporting Information, Bonferroni correction). Taken together, these results imply that the dis-
tributions of spike rates and node strength across electrodes do not change more across the peri-
revision period than at other time points in the recording.
There Is No Correlation Between the Peri-Revision Change in Electrographic Features and the Proximity
to the Revision Site
We next measured the correlation between the relative change in spike rate and distance from
the site of implant revision. Figure S1 in the Supporting Information shows the individual
patient correlations. Although several individual patients had significant correlations (with
inconsistent directions), no correlation was greater than that observed at randomly chosen
pseudo-revision times (Monte Carlo test with Bonferroni correction). This suggests that the cor-
relations on individual patient levels are incidental, resulting from the high spatial autocorre-
lation in spike rates (electrodes close to each other demonstrate similar changes in spike rates)
and are not specific to the timing of the implant revision itself. The average correlation across
patients between relative spike rate change and distance from the revision site was ρ = −0.15,
which was not significant (t (9) = −1.6, p = 0.14). There was no significant correlation seen for
other choices of peri-revision durations (Figures 4A and 4C; Table S3 in the Supporting Infor-
mation). There was also no consistent correlation between relative spike rate change and func-
tional connectivity with the revision site (average ρ = 0.09, t (9) = 1.2, p = 0.26) or between
relative spike rate change and co-spike index with the revision site (average ρ = 0.08, t (9) =
0.8, p = 0.46).
839
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Figure 3. Change in electrographic features from pre- to post-implant revision. (A) The overall spike rate for an example patient (Patient 4).
The x-axis shows the time in hours, and the y-axis shows the spike rate across time. The maroon dotted vertical line shows the time of the
implant revision. Green and purple lines denote, respectively, the times defined as the pre-revision and post-revision periods assuming a 24-hr
peri-revision interval duration. (B) The average spike rate in the pre- and post-revision periods for each patient. Each line represents one patient
and connects the average spike rate in the pre-revision period to that in the post-revision period. There was no significant group change in
spike rates surrounding implant revision (paired t test, α = 0.05). (C) Spike stability in the 24-hr peri-revision interval. Each circle in the “true”
column shows the spike stability, defined as the correlation in spike rate distribution across electrodes between the pre- and post-revision time
periods. Each circle in the “Monte Carlo” column shows the same statistic, but averaged across randomly chosen pseudo-revision times. (D)
Node strength stability in the 24-hr peri-revision interval. Each circle in the “true” column shows the correlation in node strength distribution
across electrodes between the pre- and post-revision time periods. Each circle in the “Monte Carlo” column shows the same statistic, but
averaged across randomly chosen pseudo-revision times. (E and F) The spike and node strength stability, respectively, when comparing
pre- and post-revision periods for different peri-revision interval durations. Both the true and Monte Carlo statistics are shown. Error bars show
standard deviations across patients and, in the case of the Monte Carlo statistics, Monte Carlo iterations. ns = not significant.
We also measured the correlation between the relative change in node strength and dis-
tance from the revision site. The average correlation between relative node strength change
and distance from the revision site was ρ = −0.01, which was not significant (t(9) = −0.1, p =
0.92). This result was consistent when examining different peri-revision durations (Figures 4B
and 4D; Table S3 in the Supporting Information). There was also no correlation between rel-
ative node strength change and functional connectivity with the revision site (average ρ =
0.04, t(9) = 0.5, p = 0.62) or between relative node strength change and co-spike index with
the revision site (average ρ = −0.06, t(9) = −0.5, p = 0.62). Together, these results indicate that
electrodes more proximate to the revision site (as measured by distance, EEG Pearson connec-
tivity, or co-spiking) do not experience a larger change in electrographic features surrounding
the implant revision.
Network Neuroscience
840
Testing the implant effect
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
Figure 4. The effect of proximity to the revision site and anatomy on peri-revision spike and connectivity changes. (A) The correlation
between peri-revision relative spike rate change and distance from the revision site for both the true revision time (blue) and the average
and standard deviation of 1,000 randomly chosen pseudo-revision times (Monte Carlo, red; error bars indicate standard deviation across
pseudo-revision times), for a peri-revision interval duration of 24 hr. Random jitter has been added to the x-axis for visualization. (B) The
correlation between peri-revision relative node strength change and distance from the revision site for the true revision time and the average
of randomly chosen pseudo-revision times, again for a peri-revision interval duration of 24 hr. (C) The true (blue) and Monte Carlo (red) mean
and standard deviation (error bars) correlation between the relative spike rate change and distance from the revision site. The mean and
standard deviation are performed across patients and, in the case of the Monte Carlo statistics, across Monte Carlo iterations. Results for each
peri-revision duration are shown. (D) The true (blue) and Monte Carlo (red) mean and standard deviation (error bars) correlation between the
relative node strength change and distance from the revision site. Results for each peri-revision duration are shown. (E) The mean (circle) and
standard deviation (error bars) across patients of the relative change in spike rate peri-revision according to anatomical location. (F) The rel-
ative change in node strength according to anatomical location. ns = not significant.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Peri-Revision Change in Spike Rate and Node Strength Did Not Differ Across Anatomical Locations
Across all patients, 194 electrodes (19.8%) were outside cerebral tissue; we excluded these
from analysis. Three hundred forty-nine (35.6%) of electrode contacts were in white matter,
54 (5.5%) were in mesial temporal regions, 158 (16.1%) were in temporal neocortical regions,
and 226 (23.0%) were in other locations. The mean (SD) relative spike rate change in the 24-hr
peri-implant interval was 0.3 (1.0) for white matter, 0.5 (1.4) for mesial temporal, 0.3 (0.8) for
temporal neocortical, and 0.4 (1.3) for other regions. The difference between groups was not
Network Neuroscience
841
Testing the implant effect
significant (Skillings-Mack χ2(3) = 0.4, p = 0.95). The mean (SD) relative node strength change
in the 24-hr peri-implant interval was −0.3 (1.3) for white matter, −0.6 (2.5) for mesial tempo-
ral, −1.5 (3.7) for temporal neocortical, and 0.3 (1.5) for other regions. The difference between
groups was not significant (Skillings-Mack χ2(3) = 2.3, p = 0.52). There was also no difference
seen for any other peri-revision duration (Table S3 in the Supporting Information).
Peri-Revision Change in Spike Rate and Node Strength Did Not Depend on Type of Added Electrode
We tested the effect of added electrode type on relative spike rate and node strength change
using a single patient (Patient 2) who had a combination of depth and subdural electrodes added.
The median relative spike rate change for original contacts within 20 mm of the nearest
added depth contacts was −0.56, which was lower than that observed for contacts within
20 mm of the closest added subdural contacts (9.80) (Mann-Whitney U test: U(Ndepth proximate =
5, Nsubdural proximate = 17) = 16.0, p = 0.041). The median relative node strength change for
original contacts within 20 mm of the closest added depth contacts was −1.17, which was not
significantly different from that for contacts within 20 mm of the closest added subdural con-
tacts (−0.77) (Mann-Whitney U test: U(Ndepth proximate = 5, Nsubdural proximate = 19) = 41.5, p =
0.70). There was no significant difference in relative feature change between electrodes close
to added depth electrodes and those close to added subdural electrodes for any other peri-
revision duration or for using a distance threshold of 10 or 30 mm (Table S4 in the Supporting
Information). Taken together, these results suggest that the implant effect does not clearly differ
by electrode type. However, the fact that this was a single-patient analysis limits interpretation.
DISCUSSION
Establishing the existence of an “implant effect” on electrographic features is challenging
without a pre-implantation baseline. In our study, we found no evidence that implanting elec-
trodes affects either the spike rate or network connectivity of preexisting electrodes.
The Change in Spike Rates Within Each Implantation Is Inconsistent Across Patients
We observed no consistent change in spike rates from early to late in the implant. Furthermore,
the relative change in spike rate within the revised implant did not differ between the original
and the newly added electrodes. This latter result argues against an implant effect producing
immediate and transient changes in spike rates. We would expect such an effect to produce a
larger change in spike rates on the newly added electrodes compared with the original elec-
trodes (which had been in place for several days by the time of the implant revision). However,
this analysis is limited by the several confounders that influence spike rates, including peri-
implant sedation, medication changes, and seizures (Spencer et al., 2008).
The Change in Electrographic Features Pre- to Post-Electrode Revision Is No Larger Than Chance
We found no consistent pre- to post-implant revision change in overall spike rates. Also, the
pre- to post-revision change in the distribution of spikes rates and network connectivity across
electrodes was no higher than that observed at random periods throughout the intracranial
recording. This suggests that the effect of implanting new electrodes on electrographic features
from other brain regions is no larger than the baseline fluctuations in these features. Some of
these fluctuations were large (Figure 3), implying substantial variability in the distribution of
spikes across electrodes throughout the recording. This highlights the importance of analyzing
prolonged durations to capture the variability in spike location when using interictal data for
surgical planning (Conrad et al., 2020; Diamond et al., 2019; Janca et al., 2018).
Network Neuroscience
842
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
The peri-revision change in spike rate and node strength did not depend on the distance to,
functional connectivity to, or co-spiking with the implant revision site. This analysis tested the
hypothesis that implanting electrodes would disproportionately affect spiking and network
connectivity in nearby or connected regions. The negative result provides further evidence
against a direct effect of electrode implantation on spike rates and network connectivity.
Peri-Revision Electrographic Changes Do Not Differ Across Anatomical Locations
We found no difference in spike rate or node strength change across anatomical locations. This
analysis tested the hypothesis that a global implant-related cause—such as anesthesia—may
have a disproportionate effect on EEG features in certain anatomical regions. Our negative
finding leaves open the possibility that a global implant-related effect causes diffuse EEG
changes. However, our other finding of no overall peri-revision spike rate change argues
against this possibility.
Limitations
We cannot exclude an exquisitely focal implant effect, influencing only the brain regions
immediately underlying the implanted electrodes. Our finding that the electrodes added in
the implant revision do not experience a larger change in spike rate compared with the orig-
inal electrodes argues against this. Future studies incorporating microelectrode recordings
could potentially probe the hyper-local effect of implanting additional macroelectrodes.
Two additional major limitations relate to the timing of electrographic changes. First, the
24-hr pause in EEG recording surrounding implant revision precluded us from studying very
brief post-implant changes. A future study incorporating intraoperative recordings from
patients undergoing implant revision could probe this effect. Finding no implant effect in
the immediate post-implantation period would support the feasibility of using immediate post-
operative data to localize seizure generators. Second, we could not study electrographic
changes that begin after recording finishes. Other studies in long-term implantations described
chronic changes in spike rates in response to implanting neurostimulation devices (F. T. Sun
et al., 2018; Ung et al., 2017).
Most patients in our study had only stereo-EEG depth electrodes added. We might expect a
larger implant effect from the implantation of grid and strip subdural electrodes, particularly in
the setting of complications such as hemorrhage and infection. In our secondary analysis of a
single patient who underwent addition of both depth and subdural electrodes, we found no
consistent difference between electrographic feature change between the original electrodes
closest to added depth electrodes and those closest to added subdural electrodes. On the other
hand, we observed a nonsignificant (p = 0.02, α = 0.005) trend of peri-revision increased
spiking in the single patient who underwent implantation of a subdural grid. This latter result
suggests that implantation of subdural grid electrodes may increase spike rates, although this
interpretation is limited by our single patient analysis.
Clinical and Research Implications
There is concern that the early post-implant period may be nonideal for gathering electrocli-
nical data to use in surgical planning. Competing evidence supports that this period may either
be pro- or anti-convulsive. In favor of the pro-convulsive hypothesis, multiple case series
reported non-habitual seizures in the first few days after implanting intracranial electrodes
(Fountas et al., 2004; Kovac et al., 2014). Important caveats to these clinical reports are
the following: (a) They represent grid/strip implantations, which have higher rates of
Network Neuroscience
843
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
pro-convulsive complications compared with depth-only implantations. (b) Some non-
habitual seizures may simply be clinically subtle scalp-negative seizures. And (c) non-habitual
seizures may result from a combination of medication wean and peri-operative sedation,
rather than from electrode implantation itself. On the other hand, other groups have reported
cases in which electrode implantation alone apparently cured the patients’ epilepsy (Katariwala
et al., 2001; Roth et al., 2012; Schulze-Bonhage et al., 2010). A similar mechanism could
plausibly cause a temporary decrease in seizures and cortical irritability. Insofar as interictal
spikes may serve as a marker for irritable, seizure-prone cortex (Goncharova et al., 2016;
Karoly et al., 2016), then these competing hypotheses could predict either an increase or a
decrease in spikes after implantation.
We found no electrographic evidence supporting either a pro- or anti-irritative implant
effect on nearby or connected brain regions. With our study’s limitations noted above, our
findings suggest that early periods (24+ hr after electrode implantation) in intracranial record-
ing represent the patient’s typical interictal network. These findings argue against discounting
early post-implantation IEEG recording for clinical use in surgical planning or in research
aimed at understanding interictal networks.
MATERIALS AND METHODS
Patient Selection, Clinical Data Review, and Intracranial Recording
This retrospective study was approved by the Hospital of the University of Pennsylvania (HUP)
Institutional Review Board. Informed written consent was obtained from each participant. We
examined 16 sequential patients with DRE who underwent IEEG recording during presurgical
evaluation at HUP and who had electrode revision during their hospitalization. Implant revi-
sion was performed to sample brain regions not captured in the original recording and hypoth-
esized to be involved in the seizure network. A board-certified epileptologist reviewed clinical
charts for clinical information and two-year International League Against Epilepsy (ILAE) sur-
gical outcomes, when available (Wieser et al., 2001). The methods for intracranial EEG record-
ing, electrode localization, and seizure identification are described in the Supporting
Information.
EEG Preprocessing, Artifact Rejection, Spike Detection, and Functional Network Calculation
EEG recording was usually paused or leads were disconnected surrounding the implant revi-
sion (mean [M] total gap in data 25.9 hr, standard deviation [SD] 10.5 hr). Five-minute con-
tinuous segments of IEEG were selected at random from every 30 min of the full recording
duration, excluding this gap and time periods containing seizures. This downsampling was
performed to reduce computation time. The EEG signal on each 5-min segment and each elec-
trode was then subjected to automated artifact detection to identify and remove periods of
heavy noise or disconnection (see the Supporting Information).
We performed automated interictal spike detection using a previously validated detector,
described in the Supporting Information (Brown et al., 2007). We next calculated the co-spike
index for each original electrode, defined as the proportion of spikes that co-occurred within
50 ms on any revised electrode (50 ms chosen based on previous studies of spike propagation;
Baumgartner et al., 1995; Bourien et al., 2005; Tomlinson et al., 2016). The co-spike index
was averaged across all post-revision EEG segments. The co-spike index measured the degree
of connectivity to the revised electrodes as measured by spiking, where a higher co-spike
index implied higher spike-related connectivity. We also calculated functional networks for
each segment by measuring the Pearson correlation coefficient between the EEG signals on
Network Neuroscience
844
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
every pair of original electrodes (Supporting Information). As a measure of functional connec-
tivity to the revised electrodes, we then calculated, for each original electrode, the Pearson
correlation coefficient with every revised electrode, averaged over all revised electrodes
and across all post-revision EEG segments.
Within-Implant Electrographic Changes
We defined an early period and a late period for both the first and the second implant of each
patient, defined respectively as the first 12 hr and the last 12 hr of the implant (Figure 2A). The
choice of 12-hr period probed acute and potentially transient post-implantation changes,
given evidence for changes in clinical seizures that may begin soon after implantation and
persist up to 3 days (Kovac et al., 2014). As a secondary analysis, we examined shorter periods
of 3 hr and 6 hr, as well as longer periods ranging from 24 to 60 hr in 6-hr steps (Bonferroni
correction for multiple periods in secondary analyses).
We compared the overall spike rate between the early and late implantation periods using a
paired t test across patients. We performed this analysis separately for three conditions: (a) the
original electrodes in the first implant, (b) the original electrodes in the second implant, and (c)
the added electrodes in the second implant. We next measured the relative change in spike
rate between the early and late period for each of the three conditions. We tested for a differ-
ence in the early to late relative spike rate change between the first and second electrode
implantation, as well as between the newly added electrodes and the original electrodes in
the second electrode implantation using two separate paired t tests across patients. Finally,
we tested whether patients with longer implant durations had a larger relative change in spike
rates. To do this, we measured the time between the beginning of the early period and the
beginning of the late period of each implant, and we calculated the Spearman rank correlation
across patients between early to late time difference and relative spike rate change.
Analysis of Electrographic Changes Pre- to Post-Implant Revision
We restricted subsequent analyses to the original electrodes that remained in place throughout
the entirety of recording, allowing us to directly compare pre- and post-revision features on
these electrodes. Our primary analysis defined a 24-hr peri-revision interval (12-hr pre-revision
and 12-hr post-revision, ignoring periods of electrode disconnection). We repeated this anal-
ysis for peri-revision interval durations of 6 and 12 hr, as well as longer durations from 36 to
120 hr, in steps of 12 hr (with Bonferroni correction for this secondary analysis).
Change in Electrographic Features Surrounding Implant Revision
We determined whether the peri-revision change in overall spike rate was larger than expected
for random times throughout the recording. We compared the change in overall spike rates
from pre-revision to post-revision against that obtained from 10,000 Monte Carlo iterations
drawing from the original dataset but using randomly chosen pseudo-revision times. For the
Monte Carlo iterations in this and in subsequent analyses, we added a peri-pseudo-revision
pause equal to the duration of paused recording or electrode disconnection surrounding the
revision. This pause prevented a bias wherein Monte Carlo iterations would otherwise com-
pare time periods in closer temporal proximity than the true peri-revision calculation. The
Monte Carlo p value was the proportion of iterations for which the absolute value of the
pseudo-revision spike rate change was greater than or equal to the true peri-revision spike rate
change (α = 0.005, Bonferroni correction for testing 10 patients). We next tested whether there
Network Neuroscience
845
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
Connectivity distribution:
Vector containing the average node
strength of each electrode. The
distribution of connection strength
across electrodes.
was a consistent difference between spike rates in the pre- versus post-revision periods across
patients using a paired t test (α = 0.05).
We next examined how the distribution in spikes across electrodes changed in the peri-
revision period. Separately for the pre- and post-revision periods, we defined the spike rate
distribution vector to be the average spike rate in each electrode in that period. We defined
the spike stability as the Spearman rank correlation between the pre- and post-revision spike
rate distribution vectors. Higher spike stability implies a lower change in the spike rate distri-
bution across electrodes between the pre- and post-revision periods. We used a Monte Carlo
test (10,000 iterations) to determine whether the peri-revision spike stability was lower than
expected for randomly chosen pseudo-revision times for any individual patient (α = 0.005,
Bonferroni correction). We performed Fisher’s combined probability test to aggregate p values
across patients (α = 0.05) (Fisher, 1934). A significant result implies that the peri-revision
change in spike rate distribution is larger than expected for randomly chosen times.
We also tested whether the distribution in functional connectivity changed in the peri-
revision period. We measured the node strength of each original electrode, defined as the
sum of the Pearson correlation coefficients across other original electrodes (Fornito et al.,
2016). We measured the average node strength in each electrode in each time period, defining
a connectivity distribution vector for each period. We defined the node strength stability as the
Spearman rank correlation between the pre- and post-revision vectors. We performed a Monte
Carlo test (10,000 iterations) to compare the node strength stability with that observed at ran-
dom pseudo-revision times (α = 0.005). We performed Fisher’s combined probability test to
aggregate p values across patients (α = 0.05).
Correlation Between EEG Feature Changes and Distance From and Connectivity To Implanted Electrodes
We hypothesized that changes in spike rate and functional connectivity would be larger for
original electrodes closer to or more connected to the site of implant revision. We examined
three proximity measures for each original electrode: the Euclidean distance to its nearest
newly implanted electrode, the average Pearson connectivity to the new electrodes, and the
co-spike index with the new electrodes.
We calculated the peri-revision relative change in spike rate and node strength between the
pre- and post-revision periods. We then measured the Spearman rank correlation between the
vector representing the peri-revision relative change in the electrographic feature and the vector
representing the proximity to the revision site (each vector was NEO × 1 in size, where NEO is the
number of original electrodes), defining the proximity-change correlation. Electrodes with zero
spikes pre-revision sometimes had an infinite relative increase in spike rate. This occurred for
an average of 5.3 (3.8%) electrodes across patients. Spearman correlation ranks these electrodes
as tied for the highest relative spike rate change. We performed a Monte Carlo test (10,000 itera-
tions) to test whether the proximity-change correlation was larger than expected for randomly cho-
sen pseudo-revision times (α = 0.005). We next tested whether there was a consistent direction of
correlation between the EEG feature and proximity measure across patients. We performed Fisher’s
r- to z-transformation on each proximity-change correlation to transform it to an approximately
normally distributed value z (Fisher, 1915). We aggregated the z values across patients and per-
formed a two-sided t test to determine whether these were significantly different from 0 (α = 0.05).
Anatomical Differences in Changes in Peri-Revision Spike Rate and Connectivity
We next tested whether different anatomical regions demonstrate different changes in peri-
revision spike rate or connectivity. This method is described fully in the Supporting Information.
Network Neuroscience
846
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
Effect of Electrode Type on Implant Effect
We asked whether electrode type—depth versus subdural—influenced the effect of electrode
implantation on spike rates and functional connectivity. We performed a limited within-patient
analysis on Patient 2 (the only patient with both depth and subdural electrodes added). We
measured the distance in millimeters between each original electrode and the nearest added
depth and subdural electrode, respectively. We identified those electrodes whose distance was
less than 20 mm (a threshold chosen based on visualizing a histogram of distances; we also
tested threshold distances of 10 and 30 mm). We compared the peri-implant relative change in
spike rate and node strength between those electrodes most proximate to added depth elec-
trodes and those most proximate to added subdural electrodes using a Mann-Whitney U test.
Statistical Analysis
All analyses were performed in MATLAB 2021a (Mathworks). The Skillings-Mack test was per-
formed using the skillmack package in MATLAB (Pingel, 2010). EEG data are publicly avail-
able on ieeg.org. All code, along with an intermediate dataset containing spike detections and
network calculations, is available on GitHub (Conrad, 2021; https://github.com/erinconrad
/interictal_hubs/tree/main/implant_analyses).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
ACKNOWLEDGMENTS
The authors thank Jacqueline Boccanfuso for her help curating EEG data.
SUPPORTING INFORMATION
Supporting information for this article is available at https://doi.org/10.1162/netn_a_00248.
AUTHOR CONTRIBUTIONS
Erin Conrad: Conceptualization; Formal analysis; Writing – original draft. Russell Shinohara:
Formal analysis; Supervision; Writing – review & editing. James Gugger: Validation; Writing –
review & editing. Andrew Revell: Visualization; Writing – review & editing. Sandhitsu Das:
Methodology; Software; Writing – review & editing. Joel Stein: Methodology; Software;
Writing – review & editing. Eric Marsh: Conceptualization; Writing – review & editing. Kathryn
Davis: Conceptualization; Supervision; Writing – review & editing. Brian Litt: Conceptualiza-
tion; Supervision; Writing – review & editing.
FUNDING INFORMATION
Erin Conrad, National Institute of Neurological Disorders and Stroke (https://dx.doi.org/10
.13039/100000065), Award ID: R25 NS-065745. Erin Conrad, National Institute of Neurolog-
ical Disorders and Stroke (https://dx.doi.org/10.13039/100000065), Award ID: NIH
1K23NS121401-01A1. Russell Shinohara, National Institute of Mental Health (https://dx.doi
.org/10.13039/100000025), Award ID: R01MH112847. Russell Shinohara, National Institute
of Neurological Disorders and Stroke (https://dx.doi.org/10.13039/100000065), Award ID:
R01NS060910.
Institute of Neurological Disorders and Stroke
(https://dx.doi.org/10.13039/100000065), Award ID: T32NS091006. James Gugger, American
Epilepsy Society (https://dx.doi.org/10.13039/100001454). Andrew Revell, National Institute
of Neurological Disorders and Stroke (https://dx.doi.org/10.13039/100000065), Award ID:
5-T32-NS-091006-07. Eric Marsh, Intellectual and Developmental Disabilities Research Cen-
ter (https://dx.doi.org/10.13039/100007857), Award ID: P50 HD105354 Project 8785. Kathryn
Davis, National Institute of Neurological Disorders and Stroke (https://dx.doi.org/10.13039
James Gugger, National
Network Neuroscience
847
Testing the implant effect
/100000065), Award ID: R01NS116504. Kathryn Davis, National Institute of Mental Health
(https://dx.doi.org/10.13039/100000025), Award ID: R01MH117155. Kathryn Davis,
Pennsylvania Tobacco Fund. Kathryn Davis, Thornton Foundation. Brian Litt, National Insti-
tute of Neurological Disorders and Stroke (https://dx.doi.org/10.13039/100000065), Award
ID: DP1NS122038. Brian Litt, National Institute of Neurological Disorders and Stroke (https://
dx.doi.org/10.13039/100000065), Award ID: 2R56NS099348-05A1. Brian Litt, The Mirowski
Family Foundation. Brian Litt, Jonathan and Bonnie Rothberg.
COMPETING INTERESTS
R. T. Shinohara receives consulting income from Octave Bioscience, and compensation for
reviewing scientific articles from the American Medical Association and for reviewing grants
for the Emerson Collective, the National Institutes of Health, and the Department of Defense.
S. Das is a consultant for Nia Therapeutics. J. M. Stein receives support from two sponsored
research agreements with Hyperfine Research, Inc., and he is a consultant for Centaur Diag-
nostics, Inc. K. A. Davis reports the following conflicts of interest: Eisai (research funding, advi-
sory board), Eton Pharmaceuticals (advisory board), GW Pharmaceuticals (consultant), SK Life
Science (advisory board), and Pfizer (consultant).
REFERENCES
Baumgartner, C., Lindinger, G., Ebner, A., Aull, S., Serles, W.,
Olbrich, A., Lurger, S., Czech, T., Burgess, R., & Lüders, H.
(1995). Propagation of interictal epileptic activity in temporal
lobe epilepsy. Neurology, 45(1), 118–122. https://doi.org/10
.1212/ WNL.45.1.118, PubMed: 7824100
Bourien, J., Bartolomei, F., Bellanger, J. J., Gavaret, M., Chauvel, P.,
& Wendling, F. (2005). A method to identify reproducible subsets
of co-activated structures during interictal spikes. Application to
intracerebral EEG in temporal lobe epilepsy. Clinical Neurophys-
iology, 116(2), 443–455. https://doi.org/10.1016/j.clinph.2004
.08.010, PubMed: 15661121
Brown, M. W., 3rd, Porter, B. E., Dlugos, D. J., Keating, J., Gardner,
A. B., Storm, P. B., Jr., & Marsh, E. D. (2007). Comparison of
novel computer detectors and human performance for spike
detection in intracranial EEG. Clinical Neurophysiology, 118(8),
1744–1752. https://doi.org/10.1016/j.clinph.2007.04.017,
PubMed: 17544322
Conrad, E. C. (2021). Interictal hubs, GitHub, https://github.com
/erinconrad/interictal_hubs/tree/main/implant_analyses
Conrad, E. C., Tomlinson, S. B., Wong, J. N., Oechsel, K. F., Shinohara,
R. T., Litt, B., Davis, K. A., & Marsh, E. D. (2020). Spatial distribution
of interictal spikes fluctuates over time and localizes seizure onset.
Brain: A Journal of Neurology, 143(2), 554–569. https://doi.org/10
.1093/brain/awz386, PubMed: 31860064
Diamond, J. M., Chapeton, J. I., Theodore, W. H., Inati, S. K., &
Zaghloul, K. A. (2019). The seizure onset zone drives
state-dependent epileptiform activity in susceptible brain
regions. Clinical Neurophysiology, 130(9), 1628–1641. https://
doi.org/10.1016/j.clinph.2019.05.032, PubMed: 31325676
Fisher, R. A. (1915). Frequency distribution of the values of the cor-
relation coefficient in samples from an indefinitely large
population. Biometrika, 10(4), 507–521. https://doi.org/10.2307
/2331838
Fisher, R. A. (1934). Statistical methods for research workers. Oliver
& Boyd.
Fornito, A., Zalesky, A., & Bullmore, E. (2016). Fundamentals of
brain network analysis. Academic Press.
Fountas, K. N., King, D. W., Jenkins, P. D., & Smith, J. R. (2004).
Nonhabitual seizures in patients with implanted subdural
electrodes. Stereotactic and Functional Neurosurgery, 82(4),
165–168. https://doi.org/10.1159/000081881, PubMed:
15528955
French, J. A. (2007). Refractory epilepsy: Clinical overview. Epilep-
sia, 48(Suppl. 1), 3–7. https://doi.org/10.1111/j.1528-1167.2007
.00992.x, PubMed: 17316406
Goncharova, I. I., Alkawadri, R., Gaspard, N., Duckrow, R. B.,
Spencer, D. D., Hirsch, L. J., Spencer, S. S., & Zaveri, H. P.
(2016). The relationship between seizures, interictal spikes
and antiepileptic drugs. Clinical Neurophysiology, 127(9),
3180–3186. https://doi.org/10.1016/j.clinph.2016.05.014,
PubMed: 27292227
Janca, R., Krsek, P., Jezdik, P., Cmejla, R., Tomasek, M., Komarek,
V., Marusic, P., & Jiruska, P. (2018). The sub-regional functional
organization of neocortical irritative epileptic networks in pedi-
atric epilepsy. Frontiers in Neurology, 9, 184. https://doi.org/10
.3389/fneur.2018.00184, PubMed: 29628910
Karoly, P. J., Freestone, D. R., Boston, R., Grayden, D. B., Himes,
D., Leyde, K., Seneviratne, U., Berkovic, S., O’Brien, T., & Cook,
M. J. (2016). Interictal spikes and epileptic seizures: Their
relationship and underlying rhythmicity. Brain: A Journal of Neu-
rology, 139(Pt. 4), 1066–1078. https://doi.org/10.1093/ brain
/aww019, PubMed: 26912639
Network Neuroscience
848
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Testing the implant effect
Katariwala, N. M., Bakay, R. A., Pennell, P. B., Olson, L. D., Henry,
T. R., & Epstein, C. M. (2001). Remission of intractable partial
epilepsy following implantation of intracranial electrodes. Neu-
rology, 57(8), 1505–1507. https://doi.org/10.1212/ WNL.57.8
.1505, PubMed: 11673602
Kovac, S., Rodionov, R., Chinnasami, S., Wehner, T., Scott, C. A.,
McEvoy, A. W., Miserocchi, A., & Diehl, B. (2014). Clinical sig-
nificance of nonhabitual seizures during intracranial EEG moni-
toring. Epilepsia, 55(1), e1–e5. https://doi.org/10.1111/epi
.12462, PubMed: 24299110
Kwan, P., Schachter, S. C., & Brodie, M. J. (2011). Drug-resistant
epilepsy. New England Journal of Medicine, 365(10), 919–926.
https://doi.org/10.1056/NEJMra1004418, PubMed: 21899452
Lee, R. W., Worrell, G. A., Marsh, W. R., Cascino, G. D., Wetjen,
N. M., Meyer, F. B., Wirrell, E. C., & So, E. L. (2014). Diagnostic
outcome of surgical revision of intracranial electrode placements
for seizure localization. Journal of Clinical Neurophysiology, 31(3),
199–202. https://doi.org/10.1097/ WNP.0000000000000047,
PubMed: 24887601
Liu, X., McCreery, D. B., Carter, R. R., Bullara, L. A., Yuen, T. G. H.,
& Agnew, W. F. (1999). Stability of the interface between neural
tissue and chronically implanted intracortical microelectrodes.
IEEE Transactions on Rehabilitation Engineering, 7(3), 315–326.
https://doi.org/10.1109/86.788468, PubMed: 10498377
Morrell, M. J. (2011). Responsive cortical stimulation for the treat-
ment of medically intractable partial epilepsy. Neurology, 77(13),
1295–1304. https://doi.org/10.1212/ WNL.0b013e3182302056,
PubMed: 21917777
Pingel, T. (2010). Skillmack [MATLAB]. https://github.com
/thomaspingel/skillmack-matlab
Polikov, V. S., Tresco, P. A., & Reichert, W. M. (2005). Response of
brain tissue to chronically implanted neural electrodes. Journal of
Neuroscience Methods, 148(1), 1–18. https://doi.org/10.1016/j
.jneumeth.2005.08.015, PubMed: 16198003
Roth, J., Olasunkanmi, A., Ma, T. S., Carlson, C., Devinsky, O., Harter,
D. H., & Weiner, H. L. (2012). Epilepsy control following intra-
cranial monitoring without resection in young children. Epilep-
sia, 53(2), 334–341. https://doi.org/10.1111/j.1528-1167.2011
.03380.x, PubMed: 22242686
Schulze-Bonhage, A., Dennig, D., Wagner, K., Cordeiro, J. G., Carius,
A., Fauser, S., & Trippel, M. (2010). Seizure control resulting from
intrahippocampal depth electrode insertion. Journal of Neurology,
Neurosurgery, and Psychiatry, 81(3), 352–353. https://doi.org/10
.1136/jnnp.2009.180075, PubMed: 20185477
Spencer, S. S., Goncharova, I. I., Duckrow, R. B., Novotny, E. J., &
Zaveri, H. P. (2008). Interictal spikes on intracranial recording:
Behavior, physiology, and implications. Epilepsia, 49(11),
1881–1892. https://doi.org/10.1111/j.1528-1167.2008.01641.x,
PubMed: 18479398
Sun, D. A., Yu, H., Spooner, J., Tatsas, A. D., Davis, T., Abel, T. W.,
Kao, C., & Konrad, P. E. (2008). Postmortem analysis following
71 months of deep brain stimulation of the subthalamic nucleus
for Parkinson disease. Journal of Neurosurgery, 109(2), 325–329.
https://doi.org/10.3171/ JNS/2008/109/8/0325, PubMed:
18671648
Sun, F. T., Arcot Desai, S., Tcheng, T. K., & Morrell, M. J. (2018).
Changes in the electrocorticogram after implantation of intracra-
nial electrodes in humans: The implant effect. Clinical Neuro-
physiology, 129(3), 676–686. https://doi.org/10.1016/j.clinph
.2017.10.036, PubMed: 29233473
Tomlinson, S. B., Bermudez, C., Conley, C., Brown, M. W., Porter,
B. E., & Marsh, E. D. (2016). Spatiotemporal mapping of interictal
spike propagation: A novel methodology applied to pediatric
intracranial EEG recordings. Frontiers in Neurology, 7, 229.
https://doi.org/10.3389/fneur.2016.00229, PubMed: 28066315
Ung, H., Baldassano, S. N., Bink, H., Krieger, A. M., Williams, S.,
Vitale, F., Wu, C., Freestone, D., Nurse, E., Leyde, K., Davis,
K. A., Cook, M., & Litt, B. (2017). Intracranial EEG fluctuates over
months after implanting electrodes in human brain. Journal of
Neural Engineering, 14(5), 056011. https://doi.org/10.1088
/1741-2552/aa7f40, PubMed: 28862995
Van Kuyck, K., Welkenhuysen, M., Arckens, L., Sciot, R., & Nuttin,
B. (2007). Histological alterations induced by electrode implan-
tation and electrical stimulation in the human brain: A review.
Neuromodulation: Technology at the Neural Interface, 10(3),
244–261. https://doi.org/10.1111/j.1525-1403.2007.00114.x,
PubMed: 22150838
Wiebe, S., Eliasziw, M., Bellhouse, D. R., & Fallahay, C. (1999).
Burden of epilepsy: The Ontario Health Survey. Canadian Journal
of Neurological Sciences / Le Journal Canadien des Sciences
Neurologiques, 26(4), 263–270. https://doi.org/10.1017
/S0317167100000354, PubMed: 10563210
Wieser, H. G., Blume, W. T., Fish, D., Goldensohn, E., Hufnagel,
A., King, D., Sperling, M. R., & Lüders, H. (2001). Proposal
for a new classification of outcome with respect to epileptic sei-
zures following epilepsy surgery. Epilepsia, 42, 282–286. https://
doi.org/10.1046/j.1528-1157.2001.4220282.x, PubMed:
11240604
Network Neuroscience
849
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
/
6
3
8
3
4
2
0
4
6
4
5
4
n
e
n
_
a
_
0
0
2
4
8
p
d
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3