Mahad Ibrahim, Aman Bhandari
Jaspal S. Sandhu, 和P. Balakrishnan
Making Sight Affordable (第一部分)
Aurolab Pioneers Production of
Low-Cost Technology for Cataract Surgery
Blindness from causes treatable by modern medicine afflicts millions of people
every year. Cataracts, the single largest cause of preventable blindness, can be treat-
ed by a simple and quick surgical procedure that restores sight; sadly, extreme
poverty and its consequences limit access to the medical technologies and infra-
structure needed for the surgery. As a result, the crush of blindness continues
unabated worldwide.
理论上, the solution to this public challenge seems simple: increase access to
care and reduce the cost of the medical technologies needed to restore sight
enough to permit cataract surgery to be performed on a mass scale (see inset text
box “The Burden of Blindness”). 在实践中, in the one place where the goal of
restoring sight affordably to the many has been achieved, success has required
three decades of effort by a dedicated team led by a visionary leader: 博士.
Govindappa Venkataswamy, an ophthalmic surgeon in Madurai, 印度. The living
legacy of Dr. Venkataswamy’s leadership is the Aravind Eye Care System, one of the
largest eye care systems in the world, with five hospitals in the Indian State of Tamil
Nadu, together performing over 200,000 cataract surgeries a year. 博士.
Venkataswamy refused to accept that people must remain blind solely because they
lack money. His thirty-year crusade has addressed the financial, organizational,
and technological barriers to affordable eye care treatment.
博士. Balakrishnan is the Managing Director of Aurolab, a non-profit manufacturing
unit of the Aravind Eye Care System, Madurai, 印度. He received his bachelor’s
degree in mechanical engineering in India and doctorate from University of
威斯康星州, 麦迪逊.
Mahad Ibrahim is a PhD student in the School of Information at the University
加利福尼亚州, 伯克利. He received his bachelor’s degree from Cornell University and
a master’s degree from the University of California, 伯克利.
Aman Bhandari is a postdoctoral fellow in Pharmaceutical Health Services
研究, University of Maryland School of Pharmacy.
Jaspal S. Sandhu is a PhD student in the College of Engineering at the University
加利福尼亚州, 伯克利. He received his master’s and bachelor’s degrees from the
麻省理工学院.
© 2006 Tagore LLC
创新 / summer 2006
25
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Ibrahim, Bhandari, Sandhu, and Balakrishnan
The Burden of Blindness
Of the estimated 161 million people worldwide who suffer from some form of
visual impairment, 90 percent live in developing countries.* In 2000, blindness
is estimated to have cost the world economy $US20-25 billion in lost produc- 活力; blindness and low vision cost India alone an estimated US$4.4 billion
annually.** The need for constant care of the blind placed by families and com-
munities exacerbates the impact of blindness, creating a significant burden in
resource-poor settings.
Beginning in the early 1970s, the World Health Organization deemed
blindness such a critical issue that they created and the International Agency
for the Prevention of Blindness. Spurred on by this global effort, the govern-
ment of India along with nongovernmental organizations focused on building
the capacity to diagnose and treat cataracts in India’s rural areas—where 70
percent of the population lives. This monumental task required training more
ophthalmologists, increasing the number of hospital beds dedicated to eye
关心, and expanding ophthalmic services into the hinterland using eye screen-
ing camps and primary health clinics.
Cataracts represent the single largest cause of preventable blindness world-
宽的. In India, cataracts are responsible for approximately 80 percent of blind-
ness.*** According to the last World Health Organization (WHO) 国家的
Programme for Control of Blindness (NPCB) survey, 12 million people in
India are blind (defined as less than 6/60 visual acuity), 和 3.8 百万人
yearly suffer from newly formed cataracts. India currently has the capacity to
perform about 1.6-1.9 million cataract operations per year, 但 5-6 百万
operations per year would be needed to tackle the accumulation of cases.****
* The 10th Revision of the of the WHO International Statistical Classification of Diseases,
Injuries and Causes of Death defined low vision as visual acuity of less than 6/18, but equal to
or better than 3/60, or corresponding visual field loss to less than 20 degrees, in the better eye
with best possible correction. Blindness is defined as visual acuity of less than 3/60, or corre-
sponding visual field loss to less than 10 degrees, in the better eye with best possible correction.
Visual impairment includes low vision as well as blindness.
** Shamanna BR, Dandona L, Rao GN, Economic burden of blindness in India, Indian Journal
of Ophthalmology, 1998;46(3):169-172.
*** Vajpayee RB, Joshi S, Saxena R, Gupta SK, Epidemiology of cataract in India: combating
plans and strategies. Ophthalmic Res. 1999;31(2):86-92.
**** Vajpayee et al., 1999.
The development of the Aravind Eye Care System (AECS) to tackle such a seri-
ous problem required a sequence of innovations, both organizational and techni-
卡尔, starting in 1976. This case focuses on Aurolab, the manufacturing arm of
Aravind, which has developed critical eye care technologies for the Aravind hospi-
tals. A subsequent case in Innovations will describe the development of the Aravind
hospital system itself.
Aurolab was founded as a non-profit Indian medical device organization in
26
创新 / summer 2006
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Making Sight Affordable (第一部分)
Cataracts
The lens of the human eye is responsible for focusing light on the retina—the
inner surface of the eye—to create images. A cataract is a clouding of this
normally transparent lens that impairs vision. Cataracts are most often asso-
ciated with aging, but can develop due to trauma, 出生时, or due to metabol-
ic causes, as well as potentially being a result of environmental factors.
Advanced cataracts can cause complete blindness, but almost all cataracts are
treatable. Surgery is the only intervention that can treat cataracts. Cataract
surgery involves removal of the clouded lens; typically, this lens is replaced
with a permanent, artificial implant known as an intraocular lens (IOL). 这
IOL focuses light on the retina, replacing the functionality of the natural lens.
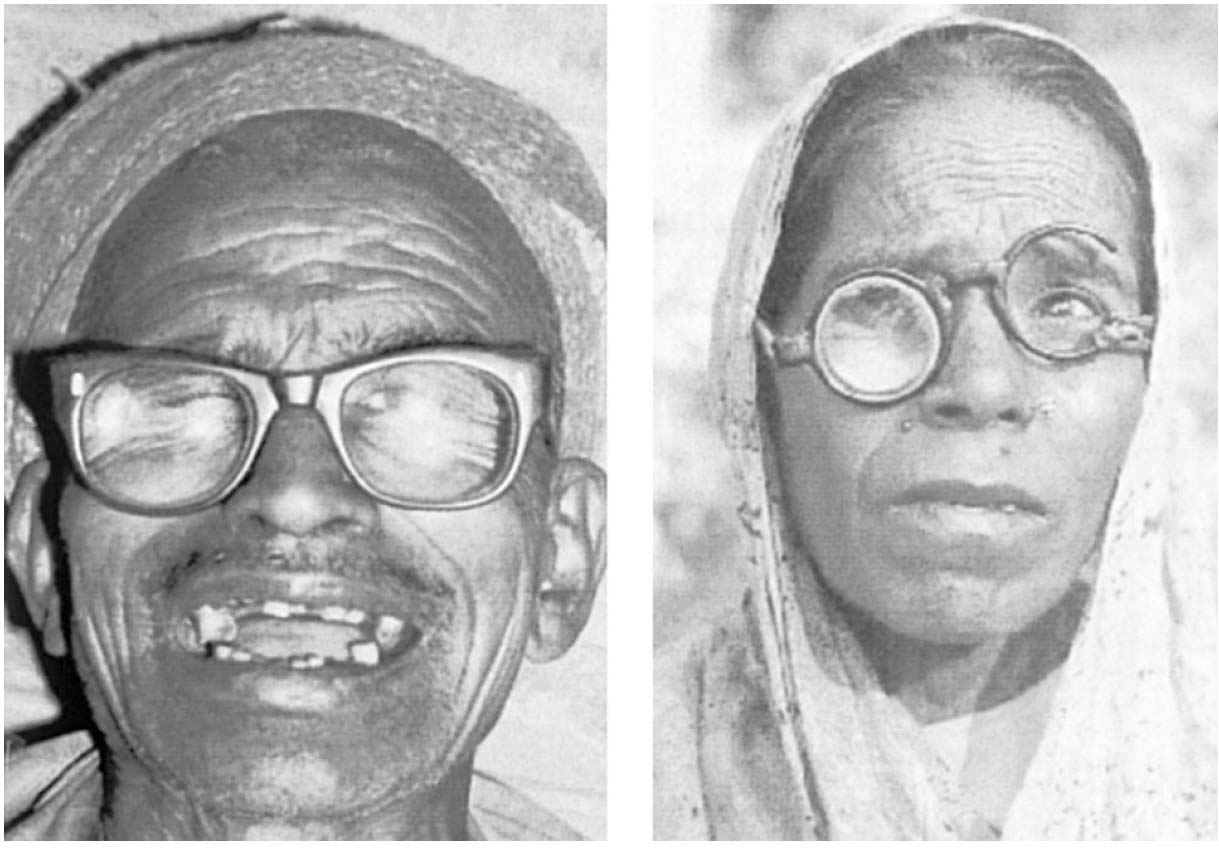
Before the IOL, cataract surgery was performed using a procedure known
as ICCE, or intra-capsular cataract extraction, that involved removal of sever-
al parts of the eye. This surgery typically subjected patients to bed rest of a
week or more. Since much of this surgery was performed before the wide
availability of IOL, patients were often fitted with external, aphakic eyeglasses,
also known as “coke bottle” glasses (见图 1).
Extra-capsular cataract extraction (ECCE) came later, and involved
removal of the cataract through an incision in the lens capsule. 尤其,
ECCE left intact parts of the eye that were removed during ICCE. The only
option for visual correction during ECCE was an artificial lens implant, 这
IOL.
Compared to ICCE, ECCE required less post-operative care—patients
could often go home the same day—and resulted in far superior visual out-
来了. Despite this, long after ECCE became the standard of care across the
industrialized world, ICCE remained widespread in the developing world.
1992 with the mission to manufacture intraocular lenses at an affordable cost for
the Indian market. For cataract surgery to be a viable option in any setting includ-
ing developing countries, the synthetic intraocular lens (IOL) is an essential com-
波南特 (see inset text box “Cataracts”). Since its founding, Aurolab has played a
unique and pioneering role in tackling the challenges of access to affordable oph-
thalmic technologies in developing countries.1 Aurolab is driven and sustained by
a strong social and spiritual mission to make high quality and affordable medical
technologies and supplies; to date, this has mostly involved the technological
inputs for cataract surgery.
Aurolab is one of a very small number of non-profit medical device or phar-
maceutical companies worldwide, and its unique capabilities in transferring vital
eye care technology to India have been paramount to its success. Aurolab’s technol-
ogy development model has three phases. 第一的, Aurolab identifies essential oph-
thalmic technologies and supplies that are inaccessible because of high cost or lim-
ited availability in the Indian market. 下一个, it assesses the potential of indigenous
创新 / summer 2006
27
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Ibrahim, Bhandari, Sandhu, and Balakrishnan
数字 1. Visual rehabilitation of aphakia with spectacles. 左边: Intact aphakic specta-
cles—poor optical correction at best. 正确的: Partially destroyed aphakic spectacles,
leaving only unilateral correction.
来源: Apple, 等人。, 2000. Cataract Surgery with Intracapsular Cataract Extraction and
Spectacles, Survey of Ophthalmology, 45:S45-S52 (figure 4.6, p. S48). © 2000 爱思唯尔
Inc. Reprinted with permission.
manufacturing and technology transfer. 最后, Aurolab develops a manufacturing
system that leverages the unique capabilities and strengths of Aurolab and India.
今天, Aurolab has grown into an organization with six product divisions
(intraocular lenses, pharmaceuticals, sutures, 仪器, spectacles, and hearing
aids) and more than 200 雇员. It supplies the lenses that Aravind uses in
多于 90 percent of its annual 200,000 plus cataract surgeries. 最近, 工作
has begun on a new manufacturing facility and business office designed to meet
strict global manufacturing standards—both the ISO 9000 standards as well as
FDA (我们. Food and Drug Administration) facility requirements—and to accom-
modate growth. Aurolab’s intraocular lenses and other products are exported to
多于 120 countries via a global network of NGO partners (大致 6 百分
of the global market). Aurolab has managed to be the first organization to provide
a solution to producing critical eye care technologies that allows the restoration of
sight among the many for whom the required surgery was previously unaffordable.
REDUCING THE COST OF A CRITICAL COMPONENT IN
CATARACT SURGERY: THE INTRAOCULAR LENS
Cataract surgery is the most common surgical procedure among the elderly in the
28
创新 / summer 2006
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Making Sight Affordable (第一部分)
美国, and one of the most common surgical procedures worldwide. 尽管
the procedure requires little post-operative care, it is often prohibitively expensive
in developing countries because of the cost of the synthetic intraocular lens and
other surgical consumables (the medical goods used during a procedure). Prior to
1992, the bundle of technologies and consumables necessary to perform cataract
surgery cost well over US$100, ensuring that cataract surgery using intraocular lenses was beyond the reach of most in the developing world. Since the vast majority of medical technologies are developed and produced in the West and targeted toward Western markets, developing countries are often at the mercy of external donations. The West’s market for ophthalmic surgical prod- ucts has been well established for more than two decades, and the international market for intraocular lenses is close to 10 million units with over US$1 billion in
sales annually, dominated by only a handful of manufacturers (例如. Alcon, AMO).2
Yet charity has provided a miniscule and inconsistent supply of lenses for patients
who cannot afford them. The story of Aurolab’s success in addressing this issue
begins long before its inception in 1992, with the pioneering work of Dr.
Venkataswamy.
在 1976, 博士. Venkataswamy founded Aravind to create an alternative model for
delivering health care that would supplement existing government services. Its first
project was the initial Aravind Eye Hospital located in Madurai, Tamil Nadu. 这
first clinic, which consisted of eleven beds in a small rented house, had many of the
elements that are representative of Aravind today. In expanding its operations ini-
tially Aravind innovated to remove the barriers to health care access in a develop-
ing country: clinical training, 支付, 运输, community education, 和
quality of care. As it has further developed it has filled the holes in system-level
deficiencies such as human resources, access to key technologies, and equipment
维护. Despite Aravind’s many successes, the organization soon faced a sig-
nificant barrier to offering widespread access to effective cataract treatment—the
lack of access to affordable intraocular lenses.
There are three surgical options for the treatment of cataract: (1) intracapsu-
lar cataract extraction (ICCE) with aphakic glasses; (2) ICCE with anterior cham-
ber intraocular lens implantation; (3) and extracapsular cataract extraction
(ECCE) with posterior chamber lens implantation (the standard of care in the
美国). The third option provides the best result, but in most developing
regions the ICCE surgery using aphakic glasses is the standard of care.
ICCE surgery is a simple procedure that does not require complex tools or
equipment, but since the clouded lens and lens capsule are removed, the eye needs
several weeks to fully heal. The main drawback of this approach is the use of apha-
kic glasses to treat a condition called aphakia, or the absence of the eye’s lens.
Aphakia is a byproduct of all forms of cataract surgery because of the need to
remove the clouded lens, but uncorrected aphakia results in a visual acuity tanta-
mount to blindness. Aphakic glasses (见图 1) present two principal problems.
First the thick lenses can cause problems with distortion and depth perception, 所以
that visual acuity is not dramatically improved. 第二, there are logistical prob-
创新 / summer 2006
29
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Ibrahim, Bhandari, Sandhu, and Balakrishnan
Medical Technologies and Developing Regions: Key Market Failures
There is little debate about the impact medical technologies have had on the
health and well-being of humans; equally indisputable is the unevenness of the
impact of medical technologies worldwide. 全球范围, approximately 90percent
of medical research funds are spent on just 10percent of the global disease bur-
这; 换句话说, most medical research focuses on diseases of the devel-
oped world. This is a natural result of the predominant private sector model
of medical technology development, which requires a strong profit motive to
persist and sustain high levels of research and development. What incentives
can be devised to increase spending and attention on developing world mar-
kets? As University of Michigan Business School professor C.K. Prahalad has
so eloquently argued, developing world markets have enormous purchasing
power collectively, and businesses with the right approach can profit from these
markets while improving conditions on the ground. The current situation has
led to three key failures in access to medical technologies:
(西德:121) High cost of existing medical technologies compared to the purchas-
ing power of individuals, 组织, and governments in developing
社团.
(西德:121) Lack of state-of-the-art technologies developed specifically for diseases
found only in resource poor settings such as India.
(西德:121) Inappropriate design of existing medical technologies for the health
care and environmental context found in many developing societies.
The creation of Aurolab was a direct response to these market failures, 和
innovation at Aurolab has centered on mitigating many of these challenges.
具体来说, Aurolab, has contributed three classes of innovations for the oph-
thalmic market in developing regions:
(西德:121) Cost reduction of key surgical consumables required for every cataract
手术, specifically the intraocular lens, ophthalmic sutures, and vis-
coelastic.
(西德:121) Mitigating supply problems through the production of neglected or
unavailable pharmaceuticals and other supplies for diseases prevalent in
the Indian context (anti-fungals).
(西德:121) Redesign of key medical technologies to make them more appropriate
for Indian context (shelf life, reusability, and packaging).
lems with providing the glasses after surgery, and problems with breakage and loss.
As one scholar noted, “At worst, breakage or loss of the glasses may condemn the
patient in a rural setting to a visual acuity as bad or worse that the acuity present
In essence, cataract surgery without the use of an
with the primary cataract.”3
intraocular lens is only half an operation, because there is not adequate visual
rehabilitation. 例如, one study in the Transvaal, 南非, found that 39
30
创新 / summer 2006
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Making Sight Affordable (第一部分)
Aurolab’s Technology Transfer Process
1) Identify prospective technologies through feedback with AECS.
2) Verify that the prospective technology has the potential to satisfy Aurolab’s
mission of producing critical eye care technologies that are affordable and
可持续的.
3) Receive approval from the board to pursue further research and develop-
ment on the potential technology.
4) Discovery phase—learn about the existing marketplace for the technology.
5) Identify potential partners for technology transfer, with the help of existing
relationships such as Project Impact and Seva Foundation.
6) Make a deal with a partner to transfer expertise and equipment necessary
to produce technology.
百分 (13 在......之外 33 cataract patients) were functionally blind because they no
longer had their aphakic glasses; a similar result was found in KwaZulu, 在哪里 113
cataract extractions resulted in an effective reduction of 16 blind patients; 其余的部分
remained functionally blind because of problems with the aphakic glasses.4
Because of the drawbacks of aphakic glasses, health care providers would only
operate on mature cataracts.
经过 1984, the ICCE operation was considered unacceptable in the West because
post-operative outcomes were considered substandard. 相比之下, ECCE surgery
allows for exceptional post-operative visual outcomes, so that it is practical to
intervene in younger patients whose cataracts are not mature. Yet there were sig-
nificant barriers to the accessibility of this procedure in developing regions such as
印度. State-of-the-art ECCE technology required:
(西德:121) Clinical training in the micro-surgical techniques necessary to perform
ECCE. Aravind had to provide and develop clinical training for this procedure
because such training was not available elsewhere;
(西德:121) Expensive equipment needed to perform the surgery and deal with any com-
并发症 (such as microscopes and a YAG laser); 和
(西德:121) Expensive consumables for each surgery (such as the lenses, methylcellulose,
and nylon sutures).5
20世纪90年代初, ECCE surgery cost three to four times more than the ICCE
procedure, even without the cost of consumables. Aravind’s challenge was to make
the surgery affordable enough to provide it to all its patients. Aravind tried to con-
vince the multinational producers of intraocular lenses to sell this critical eye care
technology to the developing world at an affordable price, but as has been shown
numerous times, health care markets in developing countries are not foremost in
the mind of multinational medical technology corporations (see inset text box
“Medical Technologies and Developing Regions”). This is reflected in the prices,
research focus, and design choices of these companies.
创新 / summer 2006
31
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Ibrahim, Bhandari, Sandhu, and Balakrishnan
桌子 1. Global costs of providing cataract surgery
Country/Region
印度, Bangladesh
Nepal
非洲
拉美
英国
德国
新西兰
澳大利亚
美国
日本 –
Cost of Surgery
(美元$) $15-$20 Acquisition price of IOL* less than $5
$80-$100
$150-$200
$1740 $1560
$1980 $1600-$2500 – – – – – $130
$105 $315
* These represent estimates based on interviews or other sources of information of the
cost to a hospital or surgeon. The cost of the IOL to the patient is often considerably
更高.
因此, the idea of Aurolab was born—an Indian, non-profit organization to
provide Aravind with affordable, high-quality lenses and supplies for cataract sur-
gery. 实际上, despite Aravind’s successful track record, few international agencies
were willing to support its mission to bring ECCE surgery to India. The prevailing
attitude was that ECCE was inappropriate for the developing context: in regions
with a dearth of health care capacity, why introduce a procedure that requires the
additional investment of significant physical and human capital? 然而,
Aravind had solved many of the health care delivery problems for eye care.6 AECS
was able to push ahead, 因为, as Mr. R.D. Thulasiraj, Executive Director of
LAICO (Lions-Aravind Institute for Community Ophthalmology), 指出,
“Having monetary success has given AECS the freedom to chart their own direc-
的, otherwise we would have had to rely on donor agencies.”
INNOVATION 1: MANUFACTURING THE LENS
The creation of Aurolab was a three-year project that started as collaboration
between Aravind, the Seva Foundation, and Sight Savers International. 类似于
the formation of many medical device companies, Aurolab had to demonstrate
need, form partnerships, engage in technology development, and raise venture
首都. 博士. 磷. Balakrishnan, an Aravind collaborator, who was working as an engi-
neering research scientist in the United States in 1989, worked with David Green
of the Seva Foundation to solve the greatest challenge to local IOL production—
access to the production technology. From its beginning, Aurolab has been
defined by technology transfer (see inset text box “Aurolab’s Technology Transfer
Process”). Aurolab had sufficient production space and resources to hire quality
32
创新 / summer 2006
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Making Sight Affordable (第一部分)
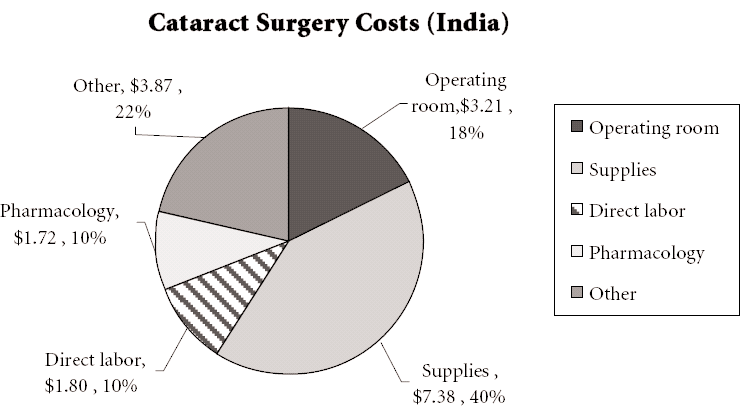
数字 2. Comparison of Costs (我们. 和印度)
来源: Naeim A. 2002. Healthcare Cost-Effectiveness Analysis for Older Patients:
Using Cataract Surgery and Breast Cancer Treatment Data. RAND publication
RGSD-168 [顶部]. Aurolab. 2004 [底部].
engineering and production staff and purchase manufacturing equipment, 但它
did not have access to the lens-making technology. The technology used to pro-
duce the intraocular lenses and other consumables were guarded closely by major
medical equipment manufacturers. The process of obtaining the technical know-
how to manufacture the lenses was arduous, but Aravind and Aurolab were ulti-
mately successful.
With the support of Seva Foundation, a systematic search was conducted to
创新 / summer 2006
33
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Ibrahim, Bhandari, Sandhu, and Balakrishnan
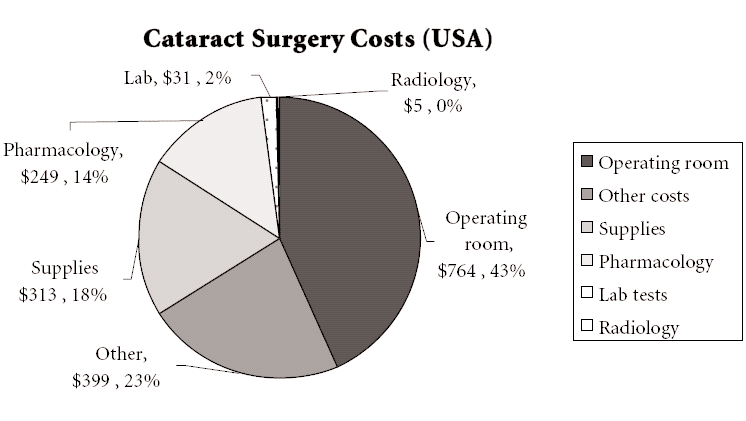
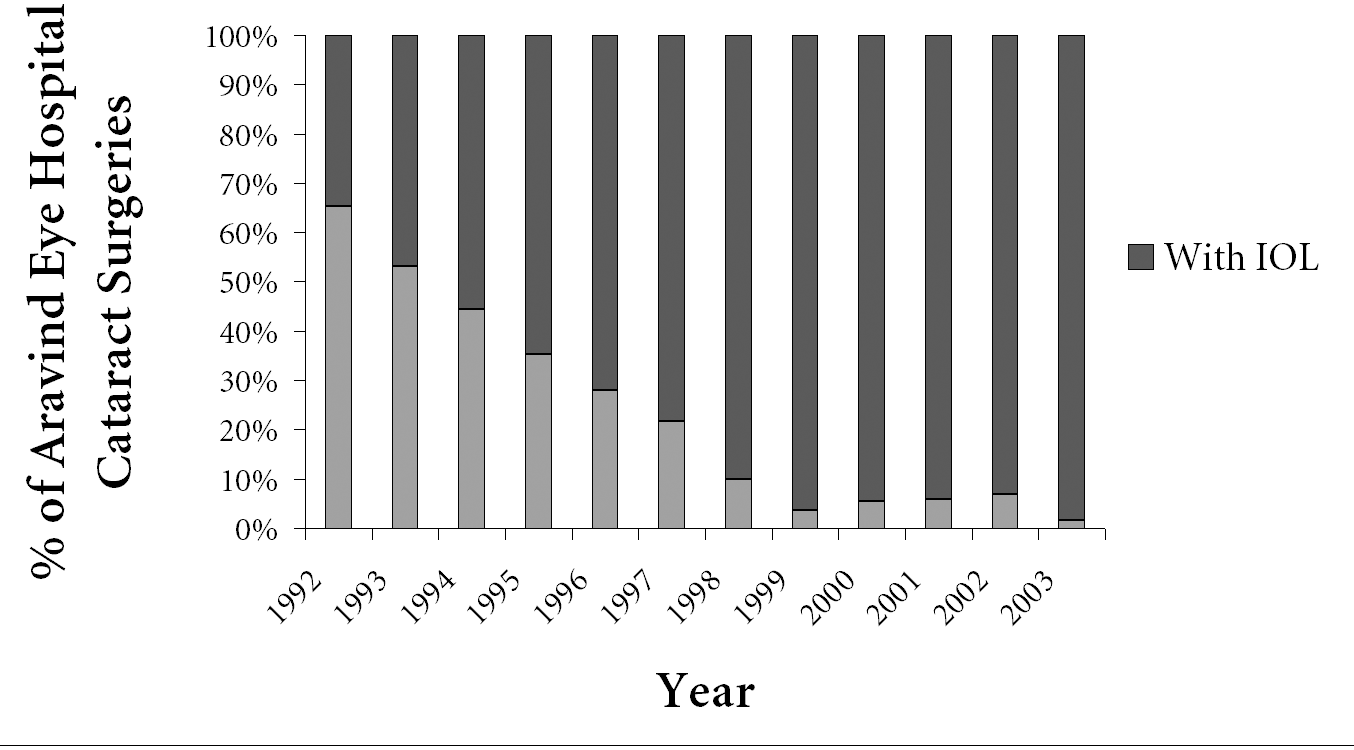
数字 3. Increase in the fraction of cataract surgeries at Aravind Eye Hospitals
involving use of intraocular lenses (IOLs) since the inception of Aurolab in 1992.
来源: Aurolab 2004
identify small companies or individuals willing to provide the know-how needed
to produce the lenses since initial efforts to obtain this expertise from established
companies were unsuccessful. 幸运的是, a small IOL manufacturer in Florida
looking to expand its business agreed to work with Aurolab to provide the expert-
ise and equipment for IOL production, 换句话说, to act as a technology
transfer agent for the lens-making technology. Given the unique physical and orga-
nizational context of Aurolab, the requirements for the equipment and processes
were tailored to minimize capital investment and instead to maximize use of the
labor cost advantage in India. The production equipment was constructed for
Aurolab by the Florida IOL manufacturer to meet these unique requirements, 和
trial run of the production system was set up in Florida to certify the system’s capa-
能力, but also to offer Aurolab engineers the chance to familiarize themselves with
the equipment and production process under the experienced eyes of the IOL
manufacturer. 然而, this exercise in technology transfer did not end in
Florida; for two weeks staff members of the IOL manufacturer made the journey
to India along with the equipment to ensure smooth installation and provide fur-
ther training to the broader Aurolab organization. Aurolab recruited experienced
nurses (also known as Sisters) from the hospital to serve as production staff and
trained them in a local contact lens manufacturing facility before the arrival of the
IOL production equipment. Through this careful planning and training, Aurolab
staff managed to quickly absorb the intricacies of IOL production. Through the
application of continuous improvement methods and procedures the rejection
rate improved gradually over a period of time. The technology provider assisted
Aurolab in monitoring and improving the production system through onsite vis-
34
创新 / summer 2006
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Making Sight Affordable (第一部分)
its and regular interaction over the course of the initial endeavor to manufacture
the lenses.
Aurolab officially began operation in 1992. At this stage, Aurolab produced
关于 100-150 three-piece lenses daily.7 In 1992 it produced nearly 35,000 PMMA
(polymethyl methacrylate) 镜片; today Aurolab manufactures over 600,000
intraocular lenses, sold in over 120 国家, and has reduced the manufacturing
cost to under US$4. In the same period, for-profit multinational ophthalmic com- panies reduced lens prices to US$100-$150 in developed markets.8 According to David Green, the price differential between the lenses produced in Madurai and those manufactured in developed countries is largely a result of the difference in organizational orientation: 基本上, we use the same equipment and manufacturing process and we fulfill the same regulatory requirements for quality as other companies do, whether they are in America or Europe or elsewhere … but Aurolab sells the lenses for less, not only because their costs are lower but because they choose to price them lower—because our goal is maximizing serv- ice rather than maximizing profit.9 These first production runs were sold to Aravind for INR (Indian rupees) 300 (US$11.60)10 per unit, as compared to the best discounted price of INR 2000
(US$77.50) for lenses from multinational companies. 随着时间的推移, Aurolab further reduced the lens cost to a price of INR 200 (US$7.75). This cost reduction has dra-
matically increased the number of ECCE procedures at AECS, 从 35 的百分比
all cataract-related procedures in 1992 到 98 百分比在 2004. 桌子 1 shows the
cost of cataract surgery in various geographic regions, as well as the cost of intraoc-
ular lenses; Aurolab’s impact on the costs in India are very clear. 数字 2 显示了一个
detailed comparison of cataract surgery costs between the United States and India.
数字 3 shows Aravind’s growth in ECCE procedures since the inception of
Aurolab.
The introduction of IOLs at the low end of the market by Aurolab created mil-
lions of new customers and increased substantially the overall IOL market size in
印度. Multinational companies had minimal interest in serving this market seg-
ment due to lower margins and other marketing difficulties. The considerable
growth in IOL surgery volume in many developing countries can be attributed to
the availability of quality IOLs at affordable prices.
INNOVATION 2: KEEPING UP WITH THE TIMES—FOLDABLE LENSES
The IOL market is constantly evolving as new types of intraocular lenses are devel-
oped and diffuse into the marketplace; innovation is thus a necessary part of
Aurolab’s ability to continue to provide technologies that allow doctors to deliver
the best standard of care. The single piece IOL that was state-of-the-art five years
ago is now simply a commodity. The current state-of-the-art is the foldable lens.
Of the three types of IOLs that Aurolab produces today, two are of hard polymer
创新 / summer 2006
35
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Ibrahim, Bhandari, Sandhu, and Balakrishnan
and the other is a soft, foldable lens. The primary advantage of the foldable lens is
that it enables a surgeon to use a smaller incision during surgery—the folded IOL
is inserted through this incision and unfolds into its proper form and position
after the insertion. The smaller incision has many direct clinical benefits, 包括-
ing no need for sutures, faster recovery, less astigmatism, and fewer post-operative
complications. 然而, the use of foldable lenses requires special equipment and
additional microsurgical training. The foldable IOL is typically used with pha-
coemulsification, a procedure that utilizes ultrasound to liquefy the clouded lens
before suction is used to remove it through a small incision.
For Western manufacturers, hard lenses represent a dead market; in develop-
ing countries, 然而, there is still a large market for hard lenses because the
expertise, equipment, and funds to support the surgery are often lacking. Foldable
lenses are produced almost exclusively by large U.S. lens producers, such as Alcon
and AMO. Sales of foldable lenses in the United States represent over 90 百分
of IOL sales, compared to just 8 percent in India. Aurolab began selling these lens-
es in 2003. The trend in India is for middle-class patients to prefer foldable lens-
英语, and for non-paying or low-income patients to select hard lenses because of
their affordability. The result is a shrinking market for quality hard lenses.
Advancements in polymeric materials led to the development of new foldable
IOLs. 那是, it is the material itself that represents the core technology of the lens.
Aurolab developed this technology through close cooperation with David Green’s
NGO Project Impact.11 In order to prove the lens safety, Aurolab conducted an 18-
month study with 100 患者; after this period Aravind adopted these lenses.
From initial technology development to lens sales took two years.
Aurolab’s price for these foldable lenses is INR 1000 (US$22), compared to the price of US$80-$100 for foldable lenses from multinational companies in India. 尤其, Aurolab managed to produce foldable lenses with minimum capital investment. Aurolab selected suitable foldable lens material and processes that could be produced with existing machinery. The lens’ flexibility is imparted at the end of the process by hydrating and packing the lens in saline solution. INNOVATIONS BEYOND THE LENS In addition to the intraocular lens, each cataract surgery requires the use of other consumables that can also present cost barriers. One expensive item is a product known as viscoelastic. Sold under the brand name Aurovisc™, viscoelastic is a high molecular weight solution of hydroxypropyl methylcellulose (HPMC) that is essential to cataract surgery. After the initial incision is made, viscoelastic is inject- ed into the eye to maintain its shape and protect interior surfaces from damage. With technical support from Moorsfield Hospital (英国), Aurolab started pro- duction of viscoelastic in 1997. At that time there were only three other manufac- turers of viscoelastic worldwide, and the solution was available at a high unit cost—8-10 percent of the total cost of consumables used in cataract surgery. 此外, the packaging was not appropriate for the Indian context. Pre-filled vials 36 创新 / summer 2006 从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023 Making Sight Affordable (第一部分) were needed, to ease both the logistical inconvenience to surgeons in the field and the cost burden for those performing fewer procedures. Aurolab’s cost structure for viscoelastic and other products is not significantly different from that of its international competitors. Particularly for raw material acquisition, Aurolab’s costs are actually higher than its international competitors— because of the shipping costs and lower-volume purchases from Western suppliers. 全面的, 80 percent of Aurolab’s raw materials come from Germany and the United States. Most of the remaining 20 percent are purchased locally.` Although pharmaceutical companies including Aurolab buy the main vis- coelastic ingredient (HPMC) from the United States, Aurolab was able to reduce the price by 50 百分, largely because of the shift to local production and selec- tive pricing. Today Aurolab sells a 2 ml pre-filled syringe for INR 45 (US$1), 和
是其中之一 10 viscoelastic manufacturers in India selling it for this price. Much as it
did for intraocular lenses, Aurolab assisted in the creation of a market and paved
the way for a collection of low-cost manufacturers.
There are two grades of viscoelastic—Aurolab produces the less expensive one.
Aurolab’s attempts to produce the higher-grade viscoelastic (sodium hyaluronate)
highlight the failure of Western manufacturers (see inset text box “Medical
Technologies and Developing Regions”) to adequately address developing world
市场. Most of the developed markets use the high-grade viscoelastic due its
benefits in the surgery. This beneficial product is not affordably available in many
markets because the knowledge needed to manufacture this high-grade viscoelas-
tic is closely guarded and controlled. Aurolab is looking at the possibility of local-
ly formulating and producing this high-grade viscoelastic using imported raw
材料, but the option of purchasing the finished product at an affordable cost
from existing manufacturers was also explored, albeit without success. 在 1995,
Aurolab was offered a price of INR 700 per ml by a U.S. company. This sourcing
price was more than 20 times the retail price of the less expensive viscoelastic
Aurolab is currently producing. Very recently, Aurolab visited another U.S. com-
pany that produces the high-grade viscoelastic, but the quoted price was US$10 per vial, equivalent to the current total cost for all surgical consumables used in cataract surgery. Aurolab asked the firm to reduce the price to US$3-4, 但是
firm required a guarantee to purchase several hundred thousand vials. Aurolab
could not possibly guarantee such a high volume purchase without incurring sig-
nificant risk. Given the large number of blind eyes worldwide and the ongoing
incidence of cataract blindness, there is potentially a huge market for high-grade
viscoelastic —but only at the right price.
CONTEXT MATTERS: ANTIFUNGALS & BUNDLED SURGERY KITS
Aurolab has focused on technologies where cost was the primary barrier, but has
also addressed other needs that multinational producers of essential medical tech-
nologies have failed to meet. Two particular concerns are problems in the supply
of technologies for diseases or conditions no longer common in the West, 和
创新 / summer 2006
37
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Ibrahim, Bhandari, Sandhu, and Balakrishnan
mismatch between the design of certain technologies and the realities of health
care infrastructure and practice in developing country settings.
例如, corneal scarring due to untreated fungal and bacterial infections
is a major cause of blindness across the world, second only to cataracts in the
developing world.12 Antifungal drugs, a major part of the required response, 是
often in short supply in the developing world. 在 2000, when Aurolab first consid-
ered development of a new antifungal drug, there was only one widely available in
the Indian marketplace. It sold for INR 100 (US$2.20) and was considered toxic. Aurolab developed a drug with much lower toxicity and sold it for INR 50 (US$1.10). To better suit the conditions of many hospitals and clinics across the
developing world, Aurolab later offered a formulation with an improved shelf life.
These local pharmaceutical innovations provided a cost-effective way to prevent
blindness due to fungal infections across the developing world.
To address a poor health care supply chain infrastructure in India and across
the developing world, Aurolab created a bundled surgery kit with all the supplies
needed to perform five cataract surgeries. By purchasing some supplies from other
manufacturers and drawing on its own diverse line of products (some manufac-
turers only produce lenses while Aurolab also produces microsurgical sutures and
ophthalmic pharmaceuticals), Aurolab provided a simple innovation that has had
a significant impact. If one lacks a single supply, those on-hand are useless. 这
bundle allows surgeons to buy their cataract-related products from a single suppli-
是, eliminating much of the uncertainty of the supply chain. This approach has
been successful partly because of the prevalence of the disease. In the developing
world cataract surgeries are performed in batches, rarely in isolation; 相比之下,
this is a relatively low-volume surgery in industrialized regions.
Reuse of single-use devices and drugs is common in emerging nations to cut
成本. Aurolab has designed products whose reuse does not reduce performance,
safety, or efficacy. 例如, Aurolab pursued rigorous testing to ensure that
reuse of suture needles for additional cases would not cause any performance
degradation of the product under normal use. Another example is the packaging
of some single-use drugs; a small quantity of the drug may be extracted more than
once through a rubber enclosure using sterile syringe needles without compromis-
ing sterility.
THE PARADOX OF PRIMARY CARE INNOVATION IN DEVELOPING
COUNTRIES: MANY TECHNOLOGIES, FEW OPPORTUNITIES
While Aurolab’s first task was to reduce the cost of the IOL, the management of
Aurolab and Aravind quickly realized that there were many essential ophthalmic
technologies that are prohibitively expensive or at least costly enough to severely
impact the bottom line of socially focused organizations in developing countries.
然而, not all these technologies represent an opportunity for Aurolab. As a
social enterprise, Aurolab must meet the dual mission of being self-sustaining and
reducing the cost of essential ophthalmic technologies. The prime opportunities
38
创新 / summer 2006
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Making Sight Affordable (第一部分)
for Aurolab are low-cost/high-volume products, where small margins can be offset
with a high volume of sales. Cataract surgery in India fits this profile perfectly,
because of India’s high prevalence and incidence of cataracts. Aurolab has focused
primarily on the consumables used in cataract surgeries, developing a full line of
IOL products, sutures, and viscoelastic solution.
Aravind and Aurolab’s success in developing a market for eye care technologies
in India has dramatically altered the landscape of available technology and inno-
vation in this arena. In addition to Aurolab, today India has roughly 150 ophthal-
mological companies, 其中 10-12 make intraocular lenses and four have CE
certification for their lenses.13 (The CE mark is a quality certification required for
marketing products in European Union countries. Aurolab was one of the first
companies in India to pursue the CE mark for IOLs and other ophthalmic medical
products.14)
Today rising demand for new products is undermining demand for some of
Aurolab’s core products. 例如, Aurolab’s development of foldable IOLs and
sutureless cataract surgeries using phacoemulsification has begun to erode sales of
hard lenses and sutures. The troubles of the suture division present a paradox of
mission versus business logic. It is clear that the market for ophthalmic sutures
will dwindle and may eventually become obsolete with greater adoption of the
sutureless surgeries. The existing manufacturing equipment and process could be
adapted to manufacture other types of sutures; 尤其, Aurolab has investi-
gated the market for sutures in cardiac surgery. This is a growing market because
of the rising incidence of heart disease in India and worldwide. Yet going beyond
its core competency to enter other markets such as cardiac sutures would be a sig-
nificant departure from Aurolab’s focus on the ophthalmic market, which would
create challenges because the Aurolab brand, as well as its sales and marketing, 是
tied heavily to its Aravind connection.
Are there other opportunities within the ophthalmic market that would allow
Aurolab to make up for the declining revenue of the suture division? The answer
is complicated. There are clearly ophthalmic technologies that are expensive and
基本的, but does Aurolab have the expertise and capacity to develop and produce
these technologies? 此外, would developing these technologies satisfy the
business logic of Aurolab? 例如, diabetes is growing problem worldwide,
and India has seen a significant growth in the prevalence of this disease. 如果不
properly managed and controlled, diabetes can lead to a number of complications
including vision loss and blindness due to a damaged retina or diabetic retinopa-
thy. Diabetic retinopathy cannot be cured but progression of vision loss can be
halted using special green laser technology. This laser is currently very expensive,
costing about INR 2 百万 (approximately US$45,000). If Aurolab could pro- duce this laser at a cost far below the current price it would have a tremendous impact on the treatment of diabetic retinopathy, but lasers differ from consum- ables both in the complexity of the technology design and production, and the market. The market for durable equipment such as the laser is typically low vol- ume and high cost because hospitals and other organizations will only make a pur- 创新 / summer 2006 39 从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023 Ibrahim, Bhandari, Sandhu, and Balakrishnan chase every five to ten years. 更远, ongoing maintenance and spare parts become critical pieces of the value chain for these products, reducing the impact of a lower initial purchase price; 此外, these areas are not within Aurolab’s current core competencies. Rather than sitting still, Aurolab is continuing to inves- tigate various technologies and innovations in the eye care arena. Thankfully, Aurolab is not alone in its mission to fill the gap in the production of affordable medical technologies. The global failure to address the lack of available and affordable medical tech- 逻辑的 (such as pharmaceuticals and medical devices) has spawned many efforts by the non-profit sector, of which Aurolab is one. 例如, the Bill and Melinda Gates Foundation has provided funding for the Institute for OneWorld Health, the first non-profit pharmaceutical company in the United States, which has developed a drug for visceral leishmaniasis,15 and has provided US$43 million
in funding to Amyris Biotechnologies for developing a synthetic malaria drug.16 A
host of other public-private partnerships are dedicated to neglected diseases.17
What differentiates Aurolab is that, while it has received critical help from Western
partnerships, it is driven from the ground up by the local community.
In filling critical gaps in the health care infrastructure for eye care in India,
Aurolab has proved a model for the indigenous development of medical technolo-
gies in developing countries. Not only has Aurolab managed to produce affordable
medical technologies, it has also, in partnership with Aravind Eye Care System, cre-
ated a solid supply chain and delivery system—often a critical deficit in resource-
poor settings. 在 14 years in operation, Aurolab has established and maintained a
position of leadership in the production of affordable ophthalmic technologies
because of its commitment to excellence and to delivering state-of-the-art care to
the underserved. There are several foreseeable challenges in the near future for
Aurolab; continued success will require renewed innovation, infused by the spiri-
We invite reader comments. 电子邮件
tual commitment and entrepreneurial vision of Dr. Venkataswamy.
Authors’ Dedication
We dedicate this article to Dr. Govindappa Venkataswamy, the founder of Aravind,
who passed away on July 7, 2006, at the age of 87. Though Dr. Venkataswamy, 或者
博士. V as he is more fondly known, is no longer with us, his mission was so power-
满, his personality so strong, and his faith so pure that he lives on in the organiza-
tion he founded and shaped until his last days—Aravind. 博士. V, who worked tire-
lessly to give sight to millions, began his medical career as an obstetrician. 在里面
prime of his life, he developed rheumatoid arthritis that eventually disfigured his
extremities so severely that he could no longer deliver babies. Dr.V has always pos-
sessed a singular focus and determination to his cause. He turned to ophthalmol-
40
创新 / summer 2006
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023
Making Sight Affordable (第一部分)
奥吉, creating specialized tools that allowed him to operate with unparalleled pre-
切除术. He was legendary in the Indian Medical Service for his stamina, routinely
performing 100 cataract surgeries a day, but this was only the beginning of his
legacy. Upon retirement from the government medical service, 博士. V enlisted the
help of his family to start the Aravind Eye Care System. Mixed with the philoso-
phy of Gandhi and Sri Aurobindo, 博士. V encountered more than a few raised eye-
brows with his insistence that if McDonald’s and Coca-Cola can bring consumer
goods to the masses, the same can be done with delivering eye care and eradicat-
ing blindness. The soul of Aravind is the deep commitment to service that perme-
ates all levels of the organization from the housekeeping staff to the surgeons, 和
is an outgrowth of the spiritual commitment of Dr. V; but what astonishes many
is that Aravind is also a superbly managed business with a focus on efficiency, fru-
gality, and innovation.
1. In the realm of ophthalmic technologies, the Fred Hollows Foundation has also been very active
in setting up IOL production facilities in Nepal and Eritrea. 此外, Jaipur Foot is a non-prof-
it manufacturer and developer of affordable prosthetics with a particular emphasis on the design of
prosthetics for the physical environment of developing regions. One important distinction between
these examples of non-profit medical technology organizations is the business model. Aurolab is a
self-sustaining and self-financing organization; these other organizations rely on the donor model.
2. Medennium news release. 2003. Medennium Announces Sale of PRL to CIBA Vision.
http://www.medennium.com/PRL_sale.htm.
3. Apple, D. 2000. Organizations Supporting Developing-World Cataract Surgery and Present
Surgical Initiatives, Survey of Ophthalmology, 45 (Suppl. 1), 191-196.
4. Yorston, D. 1998. Are intraocular lenses the solution to cataract blindness in Africa?, 英国人
Journal of Ophthalmology, 82, 469-471.
5. Perkins, A. 2001. Letter to the Editor, Community Eye Health 14(38), 51.
6. The standard of care for cataract treatment in developing regions is still Intracapsular Cataract
萃取 (ICCE) surgery with aphakic glasses. While the vast majority of cataract procedures in
India use implant intraocular lenses, in much of the developing world ICCE with aphakic glasses
remains the only choice. The cost of the lenses and other consumables is not the only barrier. 为了
例子, it is estimated that there is an ophthalmologist for every million Africans.
7. A three-piece IOL separates the two haptic ends from the main portion of the IOL.
8. Combat Blindness Foundation 2004, Project Impact 2004.
9. Herbst, K. 2004. Doing Business with Humanitarian Goals. India Together, http://www.indiato-
gether.org/2003/feb/hlt-lwcstman.htm.
10. The conversions are based on historical (1992) exchange rates from the U.S. Federal Reserve.
11. Project Impact is a non-profit organization founded by David Green to bridge the medical tech-
nology gap between the West and developing regions. They have been heavily involved with Aurolab
on the foldable lens and affordable Hearing Aid projects.
12. Bharathi MJ, Ramakrishnan R, Vasu S, Meenakshi. 2002. Palaniappan R. Aetiological diagnosis
of microbial keratitis in South India – A study of 1618 案例. Indian Journal of Medical Microbiology,
20, 19-24.
13. Personal Communication , R.D. Sriram, IOL Division Manager, Aurolab.
14. 同上.
15. Visceral leishmaniasis, also known as black fever, is a parasitic disease endemic to tropical and
temperate regions. After malaria, it is the second most deadly parasitic disease in the world.
16. Amyris Biotechnologies Press Release Dec 2004.
17. Buse K, Walt G. 2000. Global public-private partnerships: Part I—A new development in health?
Bulletin of the World Health Organization, 78(4), 549-561.
创新 / summer 2006
41
从http下载的://direct.mit.edu/itgg/article-pdf/1/3/25/704080/itgg.2006.1.3.25.pdf by guest on 07 九月 2023