社论
Incomplete COVID-19 Data:
The Curation of Medical Health Data by
the Virus Outbreak Data Network-Africa
Mirjam Van Reisen1,2,3,4†, Francisca Onaolapo Oladipo4,5,6, Mouhamed Mpezamihigo4,5, Ruduan Plug2,4,
Mariam Basajja2,4, Aliya Aktau2,4, Putu Hadi Purnama Jati4,7, Reginald Nalugala4,8, Sakinat Folorunso4,9,
Samson Yohannes Amare4,10, Ibrahim Abdulahi4,11, Oluwole Olumuyiwa Afolabi4,5, Ezra Mwesigwa4,12,
Getu Tadele Taye4,10, Abdulahi Kawu4,11, Mariem Ghardallou4,13, Yan Liang2,4, Obinna Osigwe4,5,
Araya Abrha Medhanyie4,10, Munyaradzi Mawere14
1Leiden University Medical Centre, 1310, 荷兰人
2莱顿大学, 1310, 荷兰人
3Tilburg University School of Humanities and Digital Sciences, 1310, 荷兰人
4VODAN-Africa, 260101
5Kampala International University, P.O. Box 20000, 乌干达
6Federal University Lokoja, 尼日利亚
7Central Bureau of Statistics, 81119, 印度尼西亚
8Tangaza University College, P.O.Box 15055, Karen Nairobi Code 00509, 肯尼亚
9Olabisi Onabanjo University, P.M.B 2002, Ago-Iwoye, Ogun State, 尼日利亚 120005, 尼日利亚
10Mekelle University, P.O. Box 231, 埃塞俄比亚
11Ibrahim Badamasi Babangida University, 911101, 尼日利亚
12Makerere University, P.O. Box 7062 Kampala, 乌干达
13Université de Sousse, 4002 Sousse, Tunisia
14Great Zimbabwe University, P.O. Box 1235 Masvingo, Zimbabwe
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
t
/
我
关键词: FAIR Guidelines; FAIR Equivalency; Federated data; Digital health; GDPR; VODAN-Africa
引文: Van Reisen, M。, Oladipo, F。, Mpezamihigo, M。, Plug, R。, Basajja, M。, Aktau, A。, Purnama Jati, P.H., Nalugala, R。,
Folorunso, S。, Amare, Y.S., Abdulahi, 我。, Afolabi, O.O., Mwesigwa, E., Taye, G.T., Kawu, A。, Ghardallou, M。, 梁, Y。, Osigwe,
奥。, Medhanyie, A.A., Mawere, M。: Incomplete COVID-19 data: The curation of medical health data by the Virus Outbreak
Data Network-Africa. 数据智能 4(4), 673–697 (2022). 土井: 10.1162/dint_e_00166
Submitted: 行进 10, 2021; 修改: 六月 10, 2022; 公认: 七月 15, 2022
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
†
Corresponding author: Mirjam van Reisen, Leiden University Medical Centre (LUMC) (电子邮件: m.e.h.van_reisen@lumc.nl,
mirjamvanreisen@gmail.com; ORCID: 0000-0003-0627-8014).
© 2022 Chinese Academy of Sciences. 根据知识共享署名发布 4.0 国际的 (抄送 4.0) 执照.
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
抽象的
The incompleteness of patient health data is a threat to the management of COVID-19 in Africa and
globally. This has become particularly clear with the recent emergence of new variants of concern. The Virus
Outbreak Data Network (VODAN)-Africa has studied the curation of patient health data in selected African
countries and identified that health information flows often do not involve the use of health data at the point
of care, which renders data production largely meaningless to those producing it. This modus operandi leads
to disfranchisement over the control of health data, which is extracted to be processed elsewhere. 作为回应
对于这个问题, VODAN-Africa studied whether or not a design that makes local ownership and repositing
of data central to the data curation process, would have a greater chance of being adopted. The design team
based their work on the legal requirements of the European Union’s General Data Protection Regulation
(GDPR); the FAIR Guidelines on curating data as Findable, Accessible (under well-defined conditions),
Interoperable and Reusable (FAIR); and national regulations applying in the context where the data is
produced. The study concluded that the visiting of data curated as machine actionable and reposited in the
locale where the data is produced and renders services has great potential for access to a wider variety of
数据. A condition of such innovation is that the innovation team is intradisciplinary, involving stakeholders
and experts from all of the places where the innovation is designed, and employs a methodology of co-creation
and capacity-building.
ACRONYMS
Center for Expanded Data Annotation and Retrieval
CEDAR
COVID-19 coronavirus disease of 2019
eCRF
欧洲联盟
FAIR
FE-Score
GDPR
VODAN
WHO
electronic COVID report Form
欧洲联盟
Findable, Accessible, Interoperable, Reusable
FAIR Equivalency Score
General Data Protection Regulation
Virus Outbreak Data Network
世界卫生组织
1. 介绍
Following the announcement of the discovery of a new coronavirus disease of 2019 (COVID-19) ‘variant
of concern’, Omicron (B.1.1.529), the Co-Chair of the African Vaccine Delivery Alliance, Ayoade Alakija,
expressed outrage over the inadequate and incomplete action taken to include Africa in global efforts to
curb the COVID-19 pandemic. This shone a spotlight on the dramatic inequality of vaccination rates: 63%
of people in high-income countries were fully vaccinated by October 2021, compared to only 1.4% 人的
in low-income countries [1]. The B.1.1.529 variant of COVID-19 was first reported on 24 十一月 2021
by the National Institute for Communicable Diseases (NICD) [2] in South Africa, and was later classified
as the Omicron variant by the World Health Organization (WHO) [3]. The inequality of vaccination has
been condemned by WHO, with organisations such as Amnesty International calling for global vaccine equity.
674
数据智能
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
.
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
Lack of and incomplete data on COVID-19 constitutes a critical shortcoming, affecting global efforts to
curb the SARS-CoV-2 pandemic. It has resulted in a lack of clarity about the situation and obscured the
problems posed by COVID-19 on the African continent. Lack of understanding of the challenges in Africa,
missed opportunities to set up production facilities for vaccines in Africa, and limited allocation of vaccines
to Africa, have undermined efforts to get the pandemic under control on the continent—and globally. 这
failure to address vaccination needs in Africa is partly due to the of lack of reliable data on COVID-19
infection and hospitalisation rates, which has resulted in the urgency of vaccination in Africa remaining
低的. While vaccination is needed to protect populations from COVID-19, irrespective of the scale of
感染, it is also needed to curb the emergence of new variants of concern. Africa has become a blind
spot in the quantification of the global pandemic, which makes the formulation of measures and distribution
of resources for health facilities in Africa particularly challenging. Without adequate data on COVID-19
from Africa, global efforts to curb the pandemic are incomplete and new variants of concern may continue
to emerge and spread globally before proper local measures are able to be taken.
With the absence of solid data, insights into the extent to which the 1.3 billion people in Africa have
been affected are speculative [4–6]. It also remains unclear whether COVID-19 has affected the African
continent less than other continents, or if the extent of infections has simply remained undetected [7].
If access to reliable measurement is limited, COVID-19 rates of infection in Africa will remain unquantifiable.
As well as incomplete or missing data, data related to the incidence, treatment and severity of COVID-19
in Africa is often biased towards the more affluent regions, while impoverished regions see little testing, 作为
people do not have the resources to seek medical help. 在这些情况下, the number of cases and
fatalities may go unreported, which explains the high variance in the tests per case ratio across the continent.
For all of these reasons, it can be assumed that it is highly unlikely that Africa has been less affected by
COVID-19 than other places.
‘Incompleteness’ is explored as a concept by Francis Nyamnjoh, who explains the world’s predicament
as ‘incomplete’, while exploring the idea that COVID-19 invites the recognition of digital technology as a
conduit to complement human capacity [8]. Digital transitions require new paradigms “to bridge the gaps
between technological and human elements in digital service innovation” [9], and a recognition of epistemic
所有权, which can also be referred to as agentic capability [10], the ability to understand the world and
to act upon that understanding. The observation that data is incomplete, does not imply that something like
‘completeness’ can be attained. Incompleteness, as conceptualised by Nyamnjoh, refers to a state of
理解, bounded by ontology, that is characterised by “fluidity, compositeness of being and a
capacity to be omnipresent in whole or in fragments” [8].
Incompleteness is translated as any understanding that requires a certain ordering. Key ordering principles
are reflected as (逻辑的) units of analysis. Nation states remain a key ordering principle. How the world is
doing on COVID-19 is typically represented at the level of continents and countries. A comparison of
leading COVID-19 trackers (WHO coronavirus dashboard [11]; John Hopkins COVID-19 dashboard [12];
The Conversation data map of Africa [13]; and Humdata COVID-19 cases data [14]) reveals that not one
数据智能
675
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
/
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
of these trackers show differences within countries, however large these are. The data is based on averages
of partial and biased representation of some places in nations that widely vary in size, 人口,
demographics, and geography, undermining the intelligibility of differences. Such representations can be
misleading [15]. The response measures taken to fight the pandemic reflect the presentation of data as
naturally ordered within the unit of a nation state and, 因此, have consisted of the closing of borders,
national colour codes and mobility restrictions.
In the transcendence from digital data points to knowledge, these ordering principles represent images
of the human thought process, formalised as semantic data. Digital data is a set of observations that have
provenance and emerge from context, and can transcend into information, knowledge and understanding
based on selective representations, modelled as ontologies, that mirror socially understood concepts. 数据
can only ever be relevant when accompanied by semantics that give data meaning, and the accuracy and
validity of semantics is fundamental to the quality of data.
This raises the question: can we consider different ordering principles? Maeda and Nkengasong (2021) [4]
found that data is based on testing and surveillance with a highly variable capacity across and within
countries in Africa. The expectation is that data badly reflects the situation in each locality and that accurate
estimates based on means would require representative sampling in population studies, which are generally
lacking [4]. Studies that analyse data within countries show the variations obtained with a higher degree
of data granularity. John Hopkins publishes a map of data within the United States [12], which shows that
COVID-19 has affected domestic populations differently, with populations in vulnerable social economic
situations being disproportionally affected [16]. 此外, Sze et al. (2020) [17] found that vulnerability
to COVID-19 infection is not the same in different geographic locations and for different populations in
美国. The finding that populations in poverty are disproportionally affected begs the question
of how low-income communities within low-income countries are affected by COVID-19 and how we can
know this [18].
To complement the data on COVID-19 with a greater heterogeneity in terms of locations and communities
could be a way of assisting diverse communities to deal with the pandemic. A higher degree of data diversity
can also be regarded as in the global interest, as a way of getting a grip on any new SARS-CoV-2 variants
of concern that may emerge, particularly in areas that are now not represented in the data or from which
provenance is not detectable [19]. 但, in order to do so, we need a different unit of analysis, 例如,
as a starter, the health facility where health data is produced and care is provided.
In summary, the incompleteness or absence of reliable and representative data from Africa is relevant
for two main reasons: (我) it dampens the urgency to address healthcare gaps and needs in Africa related to
the pandemic, 和 (二) it exposes Africa and the world to SARS-CoV-2 variants of concerns. This may create
a vicious cycle that will maintain the conditions under which the pandemic was able to spread in the first
place and delay the transition to a post-COVID-19 era.
676
数据智能
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
.
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
2. VIRUS OUTBREAK DATA NETWORK-AFRICA
This Special Issue describes the collaborative work of the Virus Outbreak Data Network (VODAN) 非洲,
which was established soon after the COVID-19 pandemic was announced. The research reported covers
the period from March to December 2020, which is the first phase of the VODAN-Africa research programme.
The objective of this phase was to explore the cause of structurally missing data from Africa, and identify
and inventory alternative data-handling strategies that could overcome the structural problems. 这
hypothesis is that data is missing due to a global sampling bias, not due to stochastic processes.
The second research phase ran from January 2021 to March 2022. During this phase (which is ongoing
the time of writing), the network deployed a minimum viable product (MVP) of patient health records
produced in health facilities. The objective of the second phase is to bring the results into actionable
策略, software and deployment. This phase will be reported in a future publication.
VODAN was established under the GO FAIR Foundation, as a collaboration on the curation of data
relevant to the COVID-19 epidemic as Findable, Accessible (under well-defined conditions), Interoperable
and Reusable—or FAIR [20]. VODAN-Africa was developed as part of the GO FAIR Implementation Network
非洲, which primarily investigates culturally sensitive approaches to digital data handling in Africa.
VODAN-Africa is a growing network of researchers from over 10 非洲国家, as well as from other
continents. These researchers have expertise in different disciplines related to health and medicine, 数据
science and computer science, computer engineering and social sciences. The network is hosted by
Kampala International University in Uganda.
As the COVID-19 lockdowns forced most researchers to work from home, the network focused on the
use of ICT for collaboration. From the start of the network, the multidisciplinary group met online every
week on Zoom, which had the best reach in many of the low-bandwidth areas in which the members of
the network are located, allowing people in different geographies to collaborate. To increase quality in
low-bandwidth areas, the one-hour meetings were held in audio without video. Every week the team of
一些 30 researchers took stock of the progress made and discussed the way forward. The advent of new
digital communication platforms and the expansion of collaborative technologies proved to be an important
asset for international collaboration with researchers in remote locales.
The initial group of universities represented by VODAN-Africa included 11 universities and 2 centres of
expertise in 9 国家: Kampala International University (乌干达); Great Zimbabwe University and
Solidarmed (Zimbabwe); University de Sousse (Tunisia); Mekelle University and Addis Ababa University
(埃塞俄比亚); Olabisi Onabanjo University, Ibrahim Badamasi Babangida University and Data Science Nigeria
(尼日利亚); University of Liberia (利比里亚); Tangaza University (肯尼亚); Kilimanjaro Christian Medical College
(坦桑尼亚); and East Africa University (索马里). The team also collaborated with Leiden University and
Tilburg University in the Netherlands, the GO FAIR Foundation (a centre of research expertise), 斯坦福大学
大学, the Centre for Super Computing in San Diego, and the Chinese Academy of Sciences. 这
primary question that the research groups focused on was the possibility of increasing the capacity to
generate novel data within Africa, in order to strengthen the understanding of the global spread of infections
of COVID-19, while simultaneously strengthening local health systems in a sustainable manner.
数据智能
677
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
.
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
3. METHODOLOGY
The research employed an ethnographic approach, following an action research design. The investigators
sought to integrate stakeholders—such as the administrators of health facilities, data processors in facilities,
doctors and physicians, policymakers in the various ministries of health and political representatives—in
their regular consultations and exchanges. An ethnographic design is a way of exploring a problem by
engaging relevant stakeholders in a particular problem and is especially relevant when dealing with what
is known as a ‘wicked design problem’—a problem that requires structuring and definition [21]. Such a
problem may have different solutions, depending on the pathway chosen to explore the problem in the first
地方. An important determinant, 所以, is who is consulted in the process of exploring the problem.
The choice made in this research was to consult a wide array of practitioners. The consultations included
conversations and meetings, training sessions, participation in testing and participation in the meetings of
the research group. Stakeholders related closely to the collaborative effort of defining the problem, structuring
it and exploring solutions. Action research allows investigators to carefully document a design process-in-
the-making.
如前所述, the research presented in this Special Issue documents the work of the first phase of
the research performed by VODAN-Africa. The objective was to explore the ‘fuzzy front’ end of this ‘wicked
problem’ [22]. The exploration included the following objectives: (我) to understand the problem of the
incompleteness of global health data on COVID-19 and its causes, especially in relation to Africa; (二) 到
understand the related context of this problem; (三、) to explore the potential of designing solutions for more
complete data by increasing data interoperability using the FAIR Guidelines; 和 (四号) to explore avenues
for further research. The third question, on the potential of a solution using the FAIR Guidelines, splits into
two very different sub-questions, 即: (我) the potential of using the FAIR Guidelines given the regulatory
context and political policy priorities in Africa, 和 (二) the technical feasibility of the application of the
FAIR Guidelines.
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
t
.
我
4. FAIR GUIDELINES IN DATA PROTECTION THROUGH PUBLIC POLICY
4.1 Public Agenda
In this research, the framework of Kingdon is used to study the potential for the adoption of the FAIR
Guidelines to improve the handling of sensitive health data in Africa. Kingdon (1984) describes the
public agenda as emerging from what he calls a ‘primeval soup’ of ideas, generated by a “community of
specialists” [23], which can be researchers and academics, officials, or interest group analysts, from which
alternative ideas and proposals for the public agenda may emerge. He refers to ‘policy communities’ as
“specialists in a given policy area” [23]. Kingdon distinguishes three streams that need to be aligned for
any alternative to reach the policy agenda: 问题, policy and political streams. In the problem stream,
a problem is identified, framed and understood in a certain way; the policy stream identifies the alternative
solutions available to handle the problem, and the political stream is associated with the priority given to
the matter at hand. 此外, Kingdon identifies what he refers to as the ‘policy entrepreneur’—a person
or a group who has a special interest in a particular policy domain or issue and inputs time, energy and
other resources in exchange for a potential impact on the direction of the public agenda [23].
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
678
数据智能
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
4.2 The Primeval Soup of Digital Data
The concept of the FAIR Guidelines is concerned with the metaphorical primeval soup in relation to
digital data objects. The concern of FAIR data is that the lack of findability, machine-readability and semantic
meaning of digital data renders data meaningless—mere ‘floating’ digital objects that can only regain
meaning with concentrated efforts to shed light on them by connecting them with other digital objects
through which semantic meaning can be derived. The FAIR Guidelines were a response to the exponential
growth of digital data and the observation that the World Wide Web (万维网) misses a machine-actionable
equivalent necessary to create access, as well as give meaning, to digital data objects. The FAIR Guidelines
are a way of bringing life to the ‘primeval soup’ of unconnected digital data objects, which are like free
atoms that have not yet found their place in living, well-connected objects that are part of a meaningful
ecosystem. According to the theory of FAIR data, the problem can best be solved by the creation of linked
machine-actionable metadata, and the fruits of this strategy will be maximised if it can connect digital data
reposited in multiple repositories, available in various locations. 因此, the FAIR Guidelines are based on
the expectation that meaningful knowledge can be produced by linking digital data available across different
locations, which are bridged through the Internet by elastic and federated virtual computational techniques.
4.3 Data Provenance, Residence and Localisation
The concept of structured data originating from an inherently chaotic and contextual process links well
with the idea that digital data is always produced in a localised surrounding. The definition of this surrounding
is the product of social categorisation. The ownership and control of data relates to the idea that digital
data is produced in a specific place, relates to specific data subjects and that a degree of ownership and
control over this data follows from its provenance. Following Mawere and Van Stam [24], ownership and
control of data in Africa is defined at national and sub-national levels through the regulatory frameworks
in each context. 然而, ownership and control of data in African countries is limited by the extractive
practices of monopolistic platforms, which move data away from the place where it is produced [24],
creating value elsewhere and resulting in the loss of the value of this data to the place where the data was
produced [19, 25].
The ownership and control over data produced within the European Union (欧洲联盟), or in relation to it, 是
a critical notion that informs the provisions of Europe’s General Data Protection Regulation (GDPR) [26].
The GDPR informs a new ethic of ownership and control of data based on the concept of the ‘citizenship
of data’, which is rooted in an understanding of where data is coming from (provenance) and where and
for what it is being used (意义). The collection of data must be proportional to its intended use. 这
legal frameworks consider that data can be both ‘in rest’ or ‘in motion’ [27]. The GDPR and other privacy
法律, 例如, 例如, the laws of California, consider rights and obligations in relation to the disclosure
and use of personal data. Data residency refers to the geographical location where data can be stored,
based on the regulatory framework that applies. Data localisation laws refer to the regulations that specify
how data can be collected, 处理, stored or transferred within a country [28]. The recognition in recent
legislation of the relevance of ownership and control of data has consequences for data handling in Africa,
数据智能
679
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
t
.
/
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
specifically in relation to the ownership and control of the data, where the data should or could reside,
and how we can optimise practices that recognise the provenance of the data. According to the African
Union Digital Transformation Strategy for Africa (2020–2030), this recognition is likely to generate respect
for the ownership and control of data “even though Africa is at the moment less restrictive, soon it will be
necessary to ensure localization of all personal data of Africa’s citizens” [29]. The Alliance for Accelerating
Excellence in Africa has also underscored the importance of the protection of data provenance [25].
4.4 Personal Health Data
In the EU, the ownership and control over data is greater when it concerns personal data belonging to
a data subject who is a citizen of the EU and who enjoys the protection of EU laws. A higher level of
protection is awarded to health data, which is classified as sensitive personal data (文章 53, preamble of
the GDPR) [26]. The GDPR sets clear restrictions on the processing of digital data for health-related
目的, which is to be processed “only where necessary to achieve those purposes for the benefit of
natural persons and society as a whole” [26]. The purpose of such processing is identified as in:
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
…the context of the management of health or social care services and systems, including processing
by the management and central national health authorities of such data for the purpose of quality
控制, management information and the general national and local supervision of the health or social
care system, and ensuring continuity of health or social care and cross-border healthcare or health
安全, monitoring and alert purposes, or for archiving purposes in the public interest. [26]
The legislation builds on the notion that health systems are a central component of national social
protection systems, with the responsibility of providing “safe, high quality, efficient and quantitatively
adequate healthcare to citizens on their territory” [26]. The legislation explicitly identifies health data as
under the jurisdiction of national legislation and a national responsibility. This has direct implications for
the physical location of data. The relevance of safeguarding data and African interests, while supporting
the custodians of the data, is increasing, and African legislators are starting to recognise this through the
promulgation of legislation regarding the protection of personal information, including health-related
sensitive personal data [25].
5. OVERVIEW OF THIS SPECIAL ISSUE
The objective of the research reported in this Special Issue was to explore the reasons why data is
structurally missing from Africa and, based on the findings, explore the theory that the FAIR Guidelines
might be a way forward in creating new and alternative designs with the capacity to solve some of the
problems around incomplete data in Africa.
5.1 Terminology and Regulatory Frameworks
In Article 3 of this Special Issue, Plug et al. [30] present an overview of the terminology relevant to the
FAIR Guidelines, which is used as the conceptual framework for this research. This article presents a
680
数据智能
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
/
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
systematic set of terminology defined to offer greater conceptual clarity on the issues discussed in this
Special Issue. This is followed by a presentation by Stocker et al. [31] in Article 4 on the background to the
fast rise of the FAIR Guidelines on the EU policy agenda. These authors observe that the FAIR Guidelines
responded to a concern recognised by EU policymakers, 即, the loss of valuable data due to lack of
curation strategies. As this concern was rising, the need for personal data protection was simultaneously
gaining urgency, and the FAIR Guidelines present a potential solution, driving the issue onto the policy
议程. 然而, Stocker et al. [31] warn that the proof is in the pudding and that, unless the FAIR
Guidelines are transformed into a set of tools, they may be removed from the agenda, as an impractical
主张.
In Article 5, Lin et al. [32] investigate the adoption of the FAIR Guidelines in non-Western geographies.
The authors find that FAIR is recognised in the languages investigated, although to a lesser degree than in
the English literature. The findings suggest that there might be potential for the application of the FAIR
Guidelines in non-Western geographies.
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
数字 1. Legal framework for VODAN-Africa.
5.2 FAIR Equivalency
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
/
t
我
This is followed by six articles (Articles 6–11) that discuss the regulatory frameworks in six countries—
乌干达 [33], 印度尼西亚 [34], 埃塞俄比亚 [35], Zimbabwe [36], 尼日利亚 [37], and Kenya [38]—in relation to the
application of FAIR Guidelines to the digitalisation of health data. Following this, Purnama Jati et al. [39]
compare the FAIR Guidelines with open data, which is the original basis for the Satu Data policy in
印度尼西亚 (文章 11).
The researchers for this group of articles identified the EU GDPR and FAIR Guidelines as foundational
frameworks for baseline data protection, in addition to the national regulatory frameworks in each
participating country in Africa. A first task was to explore the extent to which the FAIR Guidelines were in
line with national regulatory frameworks. The FAIR Guidelines can be understood as a spectrum—the
degree of ‘FAIRness’ can range from very high to low, and the appropriate degree of FAIRness can differ
from situation to situation. The facets of the FAIR Guidelines are [40]:
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
数据智能
681
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
To be ‘Findable’:
F1: (meta)data are assigned a globally unique and persistent identifier
F2: data are described with rich metadata (defined by R1 below)
F3: metadata clearly and explicitly include the identifier of the data it describes
F4: (meta)data are registered or indexed in a searchable resource
To be ‘Accessible’:
A1: (meta)data are retrievable by their identifier using a standardised communications protocol
A1.1: the protocol is open, 自由的, and universally implementable
A1.2: the protocol allows for an authentication and authorisation procedure, where necessary
A2: metadata are accessible, even when the data are no longer available
To be ‘Interoperable’:
I1: (meta)data use a formal, accessible, 共享, and broadly applicable language for knowledge
表示.
I2: (meta)data use vocabularies that follow FAIR Principles
I3: (meta)data include qualified references to other (meta)数据
To be ‘Reusable’:
R1: (meta)data are richly described with a plurality of accurate and relevant attributes
R1.1: (meta)data are released with a clear and accessible data usage licence
R1.2: (meta)data are associated with detailed provenance
R1.3: (meta)data meet domain-relevant community standards
In Article 6, Basajja et al. [33] offers a methodology to measure the degree of alignment with the FAIR
Guidelines, called FAIR Equivalency, which is replicated in articles 7 到 11 [34–38]. FAIR Equivalency was
determined by investigating the documents constituting the regulatory framework of the country to see how
closely they are aligned with the FAIR Guidelines, as defined in the 15 facets of FAIR. The mention of the
15 FAIR facets (or equivalent terminology) in each of the policy documents was analysed by assigning codes
(to the text) and labels to the appropriate FAIR facet (IE。, F1, F2, F3, F4; A1, A1.1, A1.2, A2; I1, I2, I3; R1,
R1.1, R1.2, R1.3). The mention of an equivalent notion of the FAIR facet in a policy document was assigned
the measure ‘1’, and the absence of equivalency was assigned ‘0’. A FAIR Equivalency Score (FE-Score) 曾是
calculated as the sum of scores on all 15 facets for all policy documents. This methodology was carried
out by researchers in Uganda [33], 埃塞俄比亚 [35], Zimbabwe [36], 尼日利亚 [37] and Kenya [38], 也
印度尼西亚 [34], and is also included in an overview of comparative results presented in Table 1.
The analysis shows a high or very high degree of FAIR Equivalency in the countries studied. The percentage
ranged from 70% (in Nigeria) 到 100% (in three countries: 埃塞俄比亚, 肯尼亚, Zimbabwe). Indonesia had a
分数为 75% and Uganda of 83%. A score of 100% means that the researchers found FAIR-like principles
in all of the documents checked. A score of 100% does not mean that all of the FAIR facets are recognised
in all of the policy documents, but it means that all of documents mention at least one FAIR Equivalent.
682
数据智能
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
/
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
This means that in the policy documents, the FAIR Guidelines are recognised as relevant, at least to a certain
程度. Given the positive score of FAIR Equivalency, it was concluded that the FAIR Guidelines did not
contradict the existing national policy frameworks and that it was worthwhile to explore FAIR as a potential
framework for increasing COVID-related health data from Africa.
桌子 1. FAIR Equivalency comparison.
Variable
乌干达
印度尼西亚
埃塞俄比亚
Zimbabwe
尼日利亚
肯尼亚
Average of
percentage
(排)
12
10 (83%)
8
6 (75%)
11
11 (100%)
8
8 (100%)
10
7 (70%)
15
15 (100%)
–
88%
Total documents
Fair Equivalent
文件
F1
F2
F3
F4
A1
A1.1
A1.2
A2
I1
I2
I3
R1
R1.1
R1.2
R1.3
‘Findable’ principle in
文档
5 (41%)
3 (25%)
0
4 (30%)
9 (75%)
6 (50%)
7 (58%)
0
8 (67%)
1 (8%)
4 (30%)
4 (30%)
4 (30%)
4 (30%)
6 (50%)
Average:
24%
1 (12%)
1 (12%)
0
2 (25%)
3 (37%)
2 (25%)
4 (50%)
0
5 (62%)
0
0
1 (12%)
1 (12%)
0
3 (37%)
Average:
12.25%
4 (36%)
1 (9%)
1 (9%)
1 (9%)
9 (81%)
2 (18%)
3 (27%)
0
9 (81%)
0
2 (18%)
8 (72%)
2 (18%)
5 (45%)
10 (90%)
Average:
15.75%
1 (12%)
4 (50%)
1 (12%)
5 (62%)
6 (75%)
3 (37%)
6 (75%)
0
4 (50%)
3 (37%)
3 (37%)
2 (25%)
7 (87%)
3 (37%)
3 (37%)
Average:
34%
7 (70%)
4 (40%)
6 (60%)
0
7 (70%)
6 (60%)
7 (70%)
0
5 (50%)
1 (10%)
1 (10%)
7 (70%)
3 (30%)
5 (50%)
6 (60%)
Average:
42.5%
9 (60%)
5 (33%)
0
8 (53%)
5 (33%)
9 (60%)
8 (53%)
8 (53%)
2 (13%)
10 (67%)
5 (33%)
5 (33%)
6 (40%)
4 (40%)
3 (20%)
Average:
36.5%
‘Accessible’ principle
in document
Average:
45.75%
Average:
28%
Average:
31.5%
Average:
46.75%
Average:
50%
Average:
49.75%
‘Interoperable’
principle in document
Average:
35%
Average:
20%
Average:
33%
Average:
41.3%
Average:
23.3%
Average:
37.67%
‘Reusable’ principle
in document
Average:
35%
Average:
15.25%
Average:
56.25%
Average:
46.5%
Average:
52.5%
Average:
33.25%
来源: Created by Purnama Jati, 2021
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
/
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
38%
28.17%
13.5%
29.83%
61.83%
41.67%
55.5%
8.83%
48.67%
26.5%
24.5%
32.5%
47.67%
32.33%
40.17%
Average for
6 国家:
31.96%
Average for
6 国家:
45.04%
Average for
6 国家:
30.10%
Average for
6 国家:
39.17%
The total number of policy documents included ranged from 8 in Indonesia and Zimbabwe to 15 在
尼日利亚. Of the four components of the FAIR Guidelines, the requirement that data be ‘Accessible’ had the
highest mention (in equivalent terms), while the requirement that it be ‘Interoperable’ had the lowest
mention. Facet A1 of accessibility ([meta-]data are retrievable by their identifier using a standardised
数据智能
683
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
communications protocol) had the highest mention. A very low score was obtained for the facets A2
([meta-]data are accessible, even when the data are no longer available) and F3 ([meta]data clearly and
explicitly include the identifier of the data it describes).
肯尼亚, 乌干达, Zimbabwe and Indonesia scored the highest for data being ‘Accessible’. Ethiopia and
Nigeria scored highest for it being ‘Reusable’. ‘Findable’ had the lowest equivalency score in Ethiopia,
乌干达, Zimbabwe and Indonesia. In Indonesia, ‘Accessible’ received the greatest attention, 然而, 的
the facets, it was facet I1 ([meta-]data use a formal, accessible, 共享, and broadly applicable language
for knowledge representation) that was most frequently referred to. Zimbabwe also highlighted accessibility
the most often, but of all the facets R1.1 ([meta]data are released with a clear and accessible data usage
licence) was mentioned the most frequently. Kenya also had the highest score for the requirement that data
be ‘Accessible’, but the facet with the highest mention was the equivalent of I2 ([meta]data use vocabularies
that follow FAIR Principles). The highest score for each of the guidelines among the six countries was Nigeria
for data being ‘Findable’, Kenya for ‘Accessible’, Zimbabwe for ‘Interoperable’ and Ethiopia for ‘Reusable’.
It was concluded that the FAIR Guidelines are aligned with the national policy documents of the respective
governments and regulatory bodies, which constitute the regulatory frameworks of the six countries
studied [33–38].
5.3 Exploring the Information Flows of Digital Health Data: The Problem of Data Extraction
In the subsequent section of the Special Issue, Basajja and Nambobi [41] offer an analysis of information
streams in selected health facilities in Uganda. This article demonstrates that data are produced in health
facilities without the data being used for care practices within the facility. The data that is produced is sent
away to the concerned ministry of health for policy purposes and further afield to platforms outside the
African continent. Data does not return to improve practices at the original point of care. This article
concludes that, unless data is analysed and visualised within the health facilities to support the quality of
关心, the production of data is meaningless. The practice of tying in digital data for reasons that do not
benefit the facility where it is produced is diagnosed as a critical problem in health data architecture today.
Basajja et al. [42] measure the interoperability of digital health solutions in Uganda by examining existing
digital health solutions in Uganda, 即, the Digital Health Atlas Uganda (DHA-U) and Uganda Digital
Health Dashboard (UDHD), using the FAIR Evaluation Services tool. This study concludes that FAIR maturity
is low in digital health solutions in Uganda. The movement of data through vertical upward streams of
competing solutions to platforms generally outside the country and the continent is not conducive to
horizontal data integration at the policy level, or at the point of care.
The articles by Basajja and Nambobi [41] and Basajja et al. [42] both point to the problem of health
data extraction. They note that data that is produced do not always serve purposes at the point of care. 这
extraction of data can be regarded as the removal of ‘value’ from Africa to solely benefit places outside the
continent. It is concluded that innovation aimed at expanding medical health data from Africa should
restore the local ownership and use of data.
684
数据智能
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
.
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
5.4 Proof of Concept of a FAIR-Based Health Data Architecture for COVID-19
The next section of this Special Issue explores the design of an alternative data architecture for COVID-
19 based on FAIR Guidelines. Basajja et al. [43] presents the proof of concept of the first test carried out
in September 2020 to place FAIR Data Points in selected African locations and curate and reposit data
locally. The data produced in machine actionable format were based on the WHO electronic COVID Report
Form (eCRF) and reposted in FAIR Data Points discoverable over the Internet. The proof of concept constituted
a test to send queries over the Internet in the form of an algorithm and compute findings by visiting the
data reposited in local containers within the places where the data was produced. The proof of concept
was carried out by Basajja in September 2020, with a data visiting experiment of FAIR Data Points placed
in two continents, one at Leiden University Medical Centre in Leiden and another one at Kampala
International University in Uganda.
The proof of concept of data visiting, which was carried out with the software produced by DSWizard
and installed in selected sites, was technically successful and showed the possibility of retaining data
ownership with data repositing of machine actionable data in locale, while adding the possibility of
querying the data across different sites, countries and continents with approved algorithms. 本实验
also revealed a range of issues that would need to be addressed in any further iteration of a solution based
on the FAIR Guidelines, as was intended. These included, among other issues the following:
•
•
•
•
•
The need for data production that was flexible and could be adapted to the input carried out at point
of care in health facilities.
Interest on the part of health facilities to understand and analyse the data they produce for improved
关心, and the focus on data most relevant to point of care operation (such as outpatient data records).
The importance of including local engineers to incorporate sensitivity to the local engineering realities,
challenges and possibilities.
The realisation that the FAIR-based data infrastructure requires new skills in terms of data science and
data curation and, 因此, the need to invest in capacity building.
The observation that co-creation with interdisciplinary experts and stakeholders connected across
非洲, and in collaboration with partners in Asia, Europe and the United States, proved to be a fast-
track to innovation.
Purnama Jati et al. [44] describes the considerations based on the proof of concept for further development
of the data infrastructure regarding the critical question of access and control to the data. Ghardallou
等人. [45] discuss a study to create FAIR data objects for data obtained through scientific data collection
and to make this data machine actionable and interoperable with the patient data obtained in VODAN-
Africa health facilities. This article focuses on data on COVID infections obtained from refugees and
migrants, who usually do not have access to medical facilities and testing. These are vulnerable populations,
in which infection may remain undetected and which have no structural access to treatment or vaccines.
This article describes how the FAIR curation of data can make these interoperable with patient data. 这
will increase the representativity of vulnerable social groups in the data.
数据智能
685
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
t
.
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
In the next article, Folorunso et al. [46] discuss a workflow in which analytical algorithmic tools can be
used on FAIR data. The study shows an in-country geographic analysis of COVID-19 infections in Nigeria,
a country with a population of over 200 百万, and attempts to clarify these variations. The study shows
that an analysis of the data can reveal large differences in infection rates within countries, enabling better
targeted policy measures.
5.5 Capacity Building
In the following two articles, Oladipo et al. [47] and Akindele et al.) [48] discuss efforts to enhance the
capacity of data curation, following FAIR data. Oladipo et al. [47] look at a new curriculum specifically
set up to grasp FAIR data curation as a new area of instruction in computer science. Akindele et al. [48]
examine the potential for reaching students in Africa through distance learning, using digital tools,
precipitated by the COVID-19 lockdowns.
6. 讨论: SPECIFICATIONS AND REQUIREMENTS FOR FURTHER IMPLEMENTATION
This Special Issue documents the first phase of the implementation of VODAN-Africa. The following
important conclusions were reached during this phase. The study of the regulatory framework for (digital)
health in five countries in Africa (埃塞俄比亚, 肯尼亚, 尼日利亚, 乌干达, Zimbabwe), as well as Indonesia,
showed an interest in the values associated with the FAIR Guidelines. The greatest interest shown was in
relation to the accessibility and interoperability of data. It was further found that data extraction from Africa
was considered a key problem to be addressed, specifically the non-use of data at the point of care where
the data extracted was generated (health facilities). The studies revealed an urgent need to redirect efforts
for data use to improve the quality of care. 此外, it was found that the parallel efforts of digital health
solutions were focused on data analytics within narrowly defined objectives, which lacked attention to
horizontal data integration within and across facilities.
Based on these preliminary findings, it was hypothesised that the FAIR Guidelines could be used as a
conceptual framework for a new approach to health data curation. The approach follows the workflow of
FAIR data proposed by Jacobsen et al. [49], who proposed the ‘FAIRification’ of both data and semantic
数据, divided into three phases: pre-FAIRification, FAIRification, and post-FAIRification (见图 2).
The efforts reported in this Special Issue are concentrated on phase 1 (pre-FAIRification) and phase 2
(FAIRification), with a proof of concept implemented as a data visiting effort in the post-FAIRification phase.
During the FAIRification phase, the team made use of the DSWizard. The selection of this tool was based
on the requirement that data should be curated in the locale in which it was produced, and hosted with
an exposure to the Internet so as to be findable and reachable for algorithmic queries. The data production
was based on the WHO eCRF, a standard document to record patient data related to COVID-19. While the
proof of concept was successful, the experiment showed that a review and adaptation was needed of the
specifications and requirements of any software to be use or produced. The adaptations to specifications
and requirements were identified as following:
686
数据智能
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
.
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
t
/
.
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
数字 2. FAIRifi cation workfl ow model [49].
• A more direct link with actual workflows within the health facilities is needed.
• The workflows have to be adaptable to variations in the workflows of different health facilities.
•
The VODAN-Africa procedure needs to be fully compatible with existing workflows in health facilities
to avoid the duplication of data input.
A flexible production of machine-actionable templates of patient data and scientific health data needs
to be available to adapt to actual work practices and to replace the inflexible standard of using just
one WHO eCRF template, which most health facilities did not use.
The localisation of data repositing and ownership by the facility over the data handling process is a
fundamental requirement for the success of the design.
Data visualisation within the health facilities was identified as a critical need for the data to be able
to inform health practices at the point of care (where the data is generated).
Software tools need to be adapted to African realities and engineers in the locale should be integrated
to strengthen co-creation innovation practices.
The capacity building of FAIR data curation and FAIRification processes, including the use and
adaptation of available software, is a critical need to ensure future sustainability and expansion.
•
•
•
•
•
数据智能
687
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
/
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
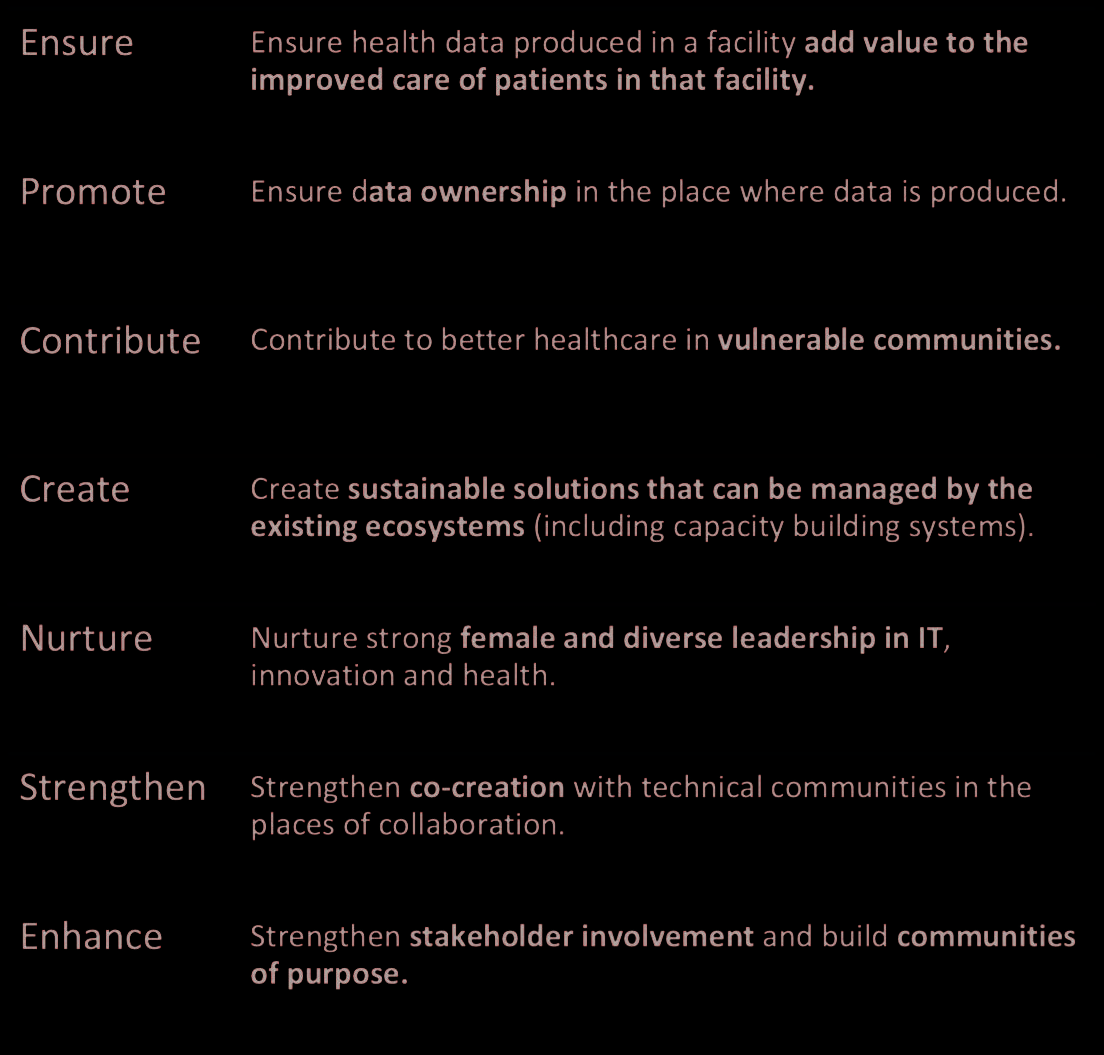
数字 3. Core values of VODAN-Africa.
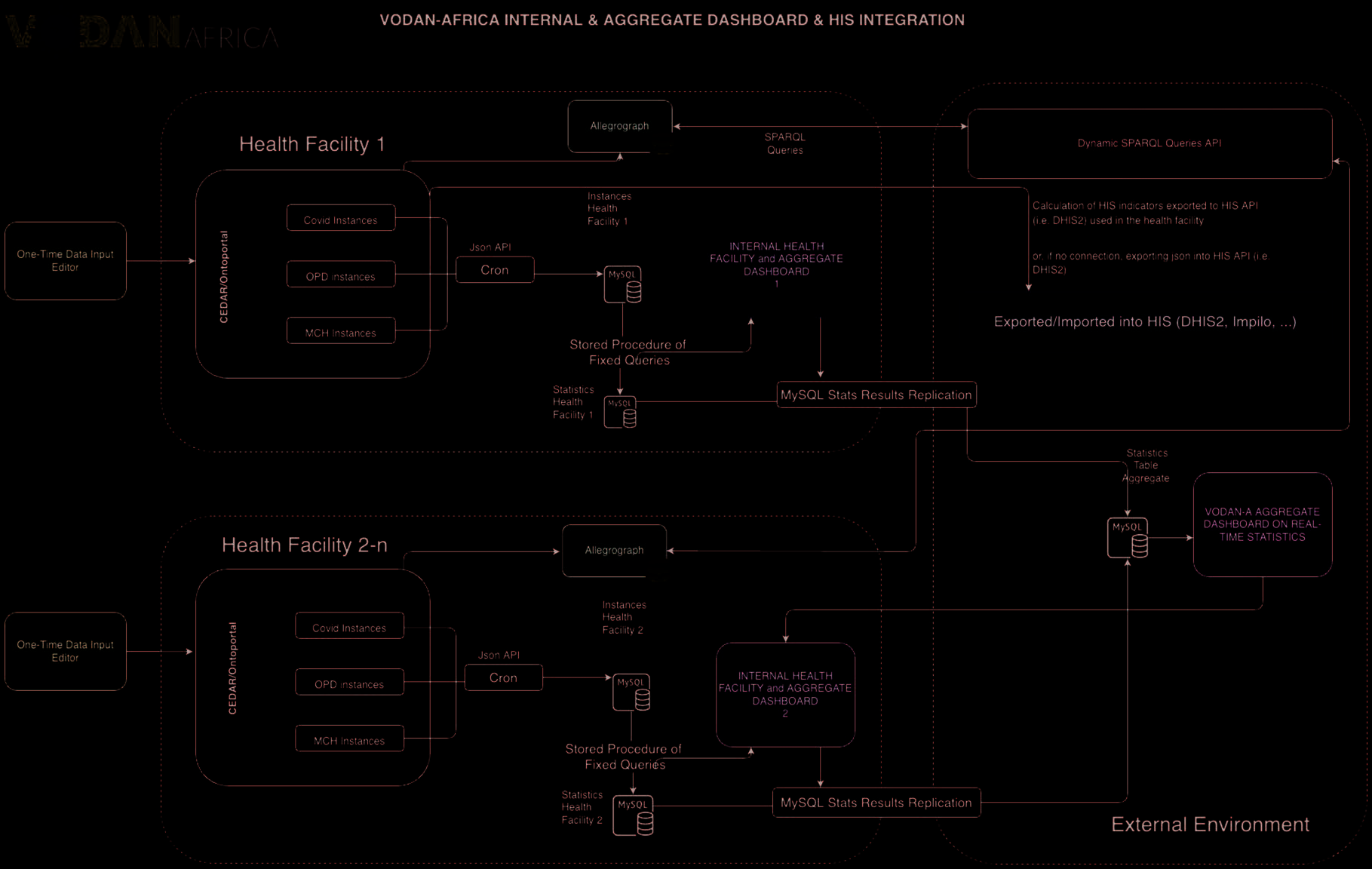
7. LOOKING AHEAD TO PHASE 2: FURTHER DEVELOPMENT OF A VODAN-AFRICA
ARCHITECTURE
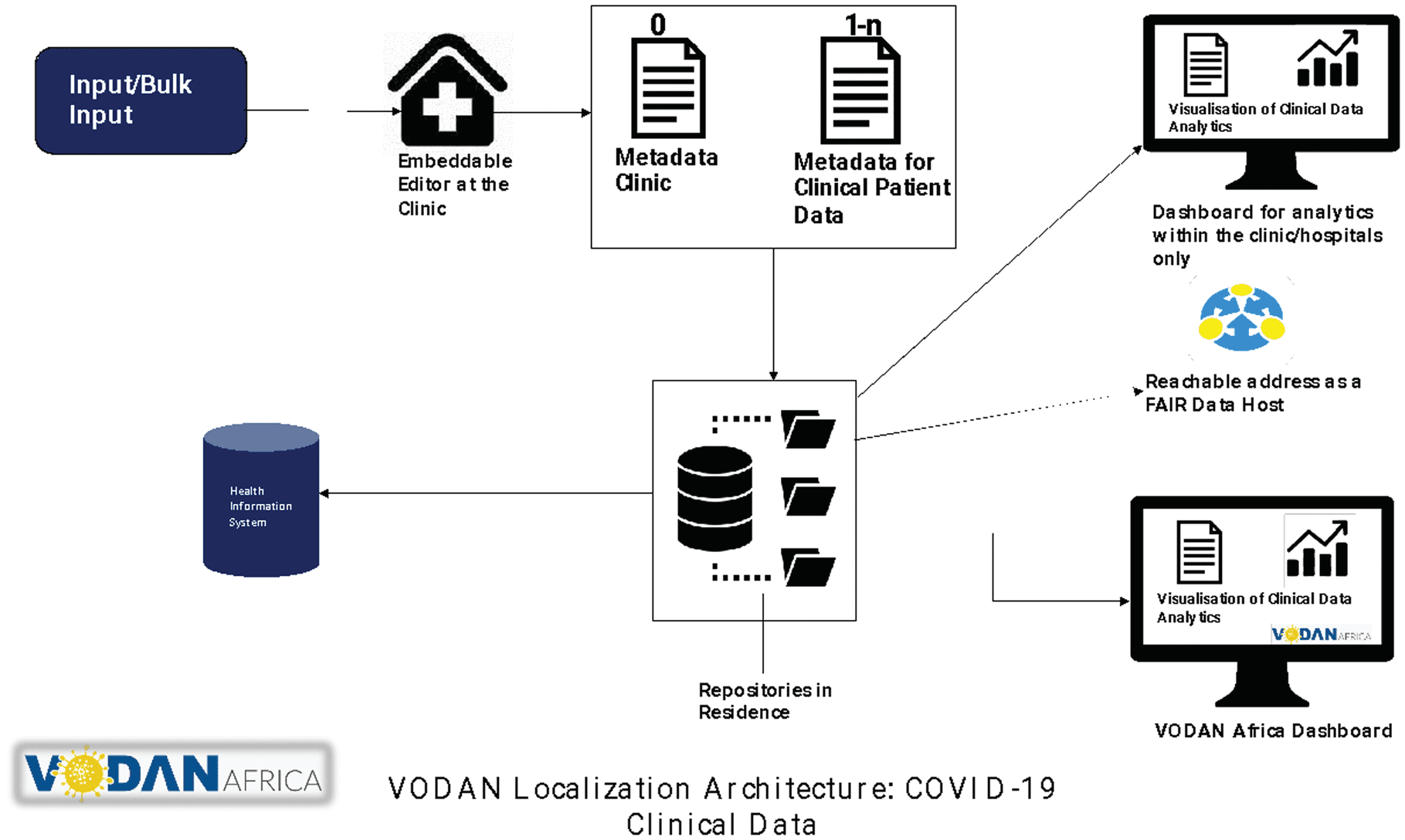
The assessment of these requirements in Phase 1 led the VODAN-Africa team to develop a new architecture
for the second phase of the VODAN-Africa implementation [19, 49]. This architecture includes a one-stop
data entry, facilitated by an editor through templates that generate machine-actionable language (RDF or
JSON), with data reposited in containers within the health facility, with an automated output to the health
information system in use by the health facility, and an output to the facility dashboard where data is
visualised for use by the medical team in the facility. The dashboard also includes the visualisation of
generic data obtained through data visiting, computed over all VODAN-Africa facilities, to provide additional
context and value to these data. The architecture enables interoperability with other data, including data
obtained through scientific efforts and curated to be interoperable with the VODAN-Africa facilities.
The research team identified that this architecture could be realised if it could develop a localised version
of the software of the Center for Expanded Data Annotation and Retrieval (CEDAR). Based at Stanford
大学, CEDAR was established in 2014 to create a computational ecosystem for the development,
评估, 使用, and refinement of biomedical metadata. In the second phase, the VODAN research team
established a collaboration for co-creation with the CEDAR team to design a localised version that could
be installed within health facilities in Africa.
688
数据智能
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
数字 4. VODAN-Africa localisation architecture for patient health records [19].
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
/
t
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
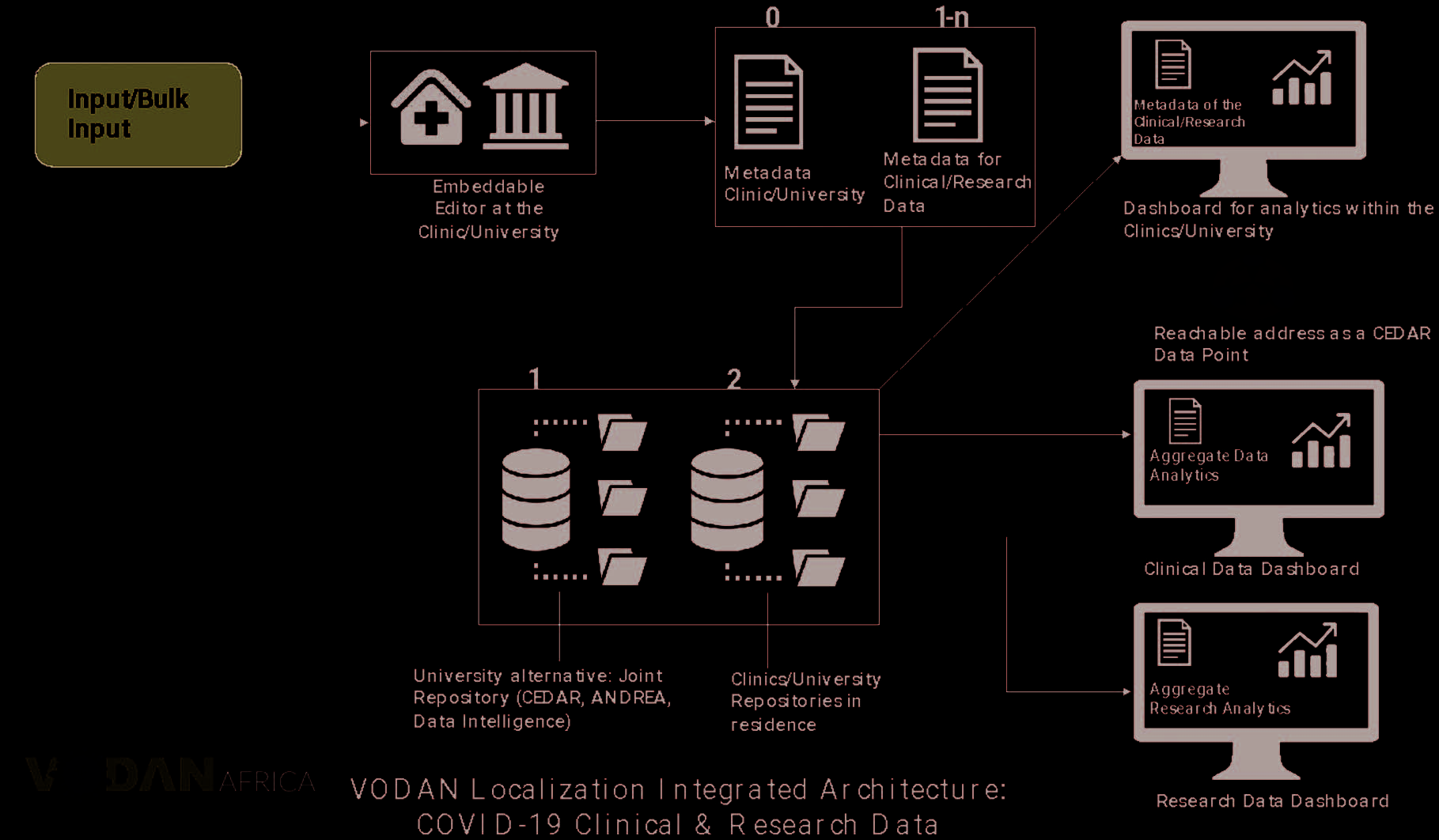
数字 5. VODAN-Africa localisation architecture for patient health records combined with scientifi c data [19].
数据智能
689
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
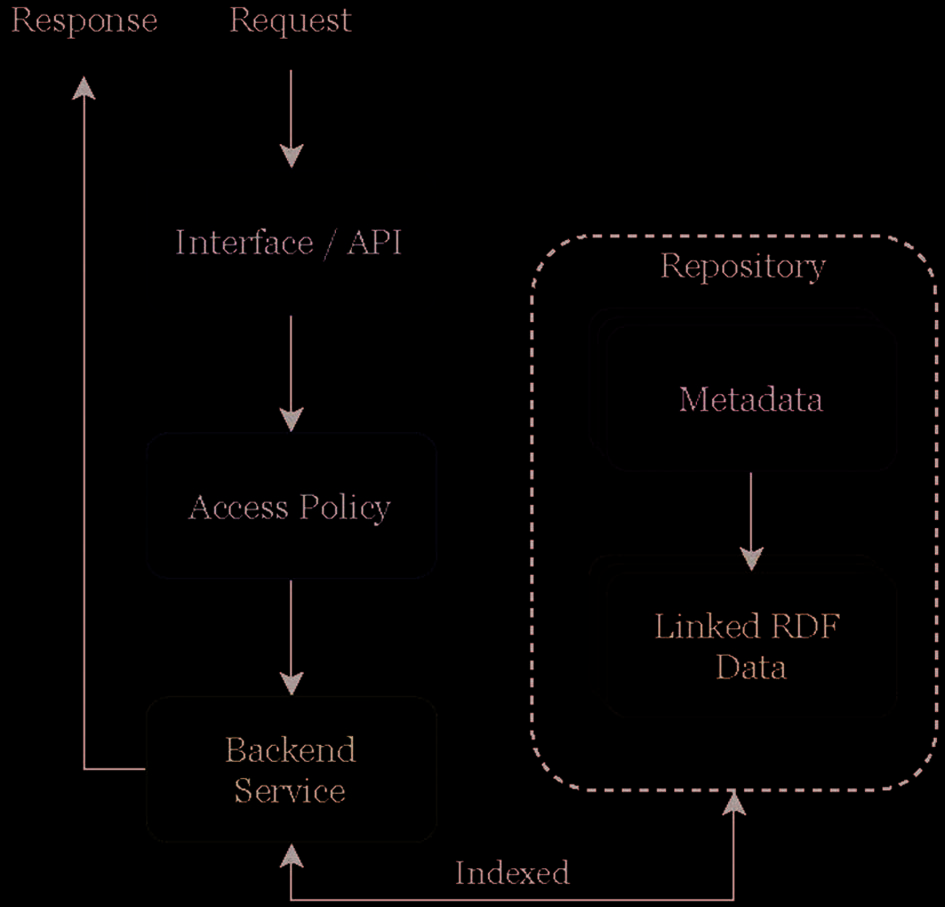
The basic infrastructure of the CEDAR-based FAIR Data Point was the creation of a visualisation on the
Dashboard based on requests sent through the interface to the back-end service of metadata reposited
within the facility, creating a front end visualisation. The FAIR Data Point does not need to be visible
publicly on the Internet, but can be installed as a point reachable through CEDAR, through which data in
location can be reached (with a prerequisite of access being granted).
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
t
.
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
数字 6. CEDAR as a FAIR Data Point [50].
The overarching architecture is based on the various components of the CEDAR software, but redesigned
to follow localisation requirements. 数字 6 shows the architecture in which CEDAR is engineered as a
FAIR Data Point, and federated with the software for localised machine actionable data production,
reachable over the Internet in a closed CEDAR community. This is the basic architecture for realisation of
localised deployment in phase 2. This is further expandable with a dynamic search function, 这是
architecturally conceptualised in Figure 7.
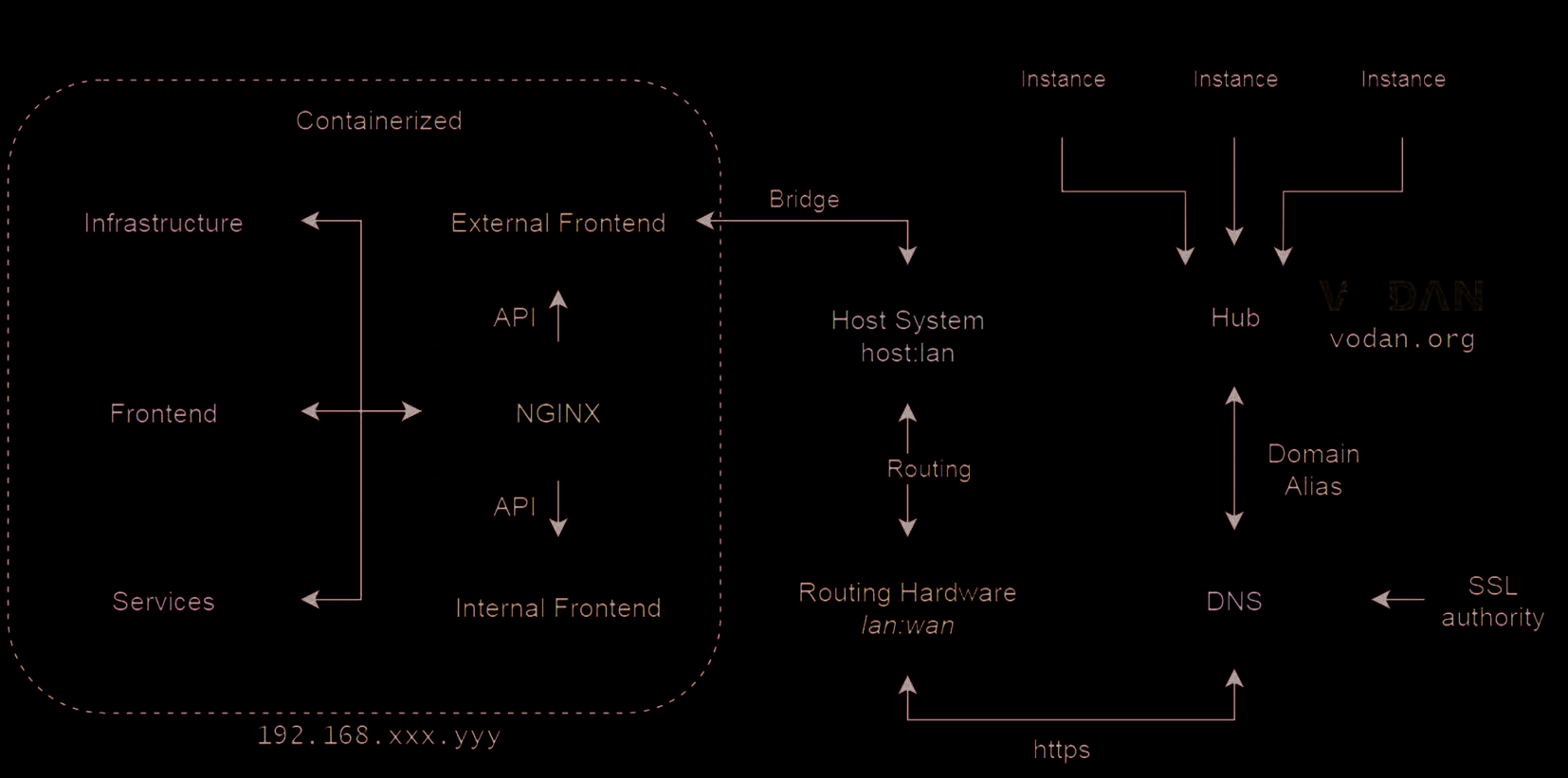
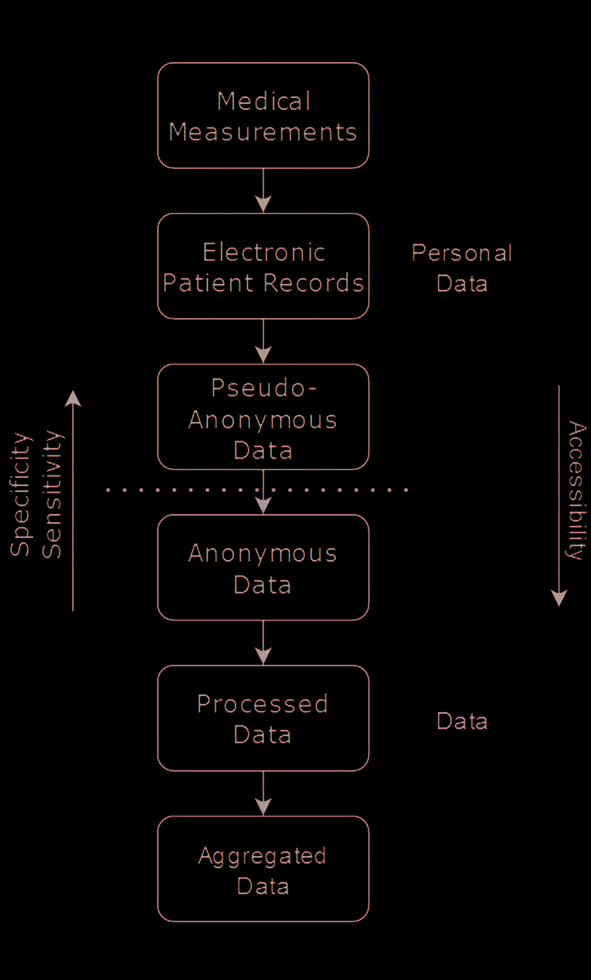
The system generates data at different levels of sensitivity for different purposes. The personal data are
受保护的, encrypted and reposited within the health facility. The processed data and aggregate data can
be visited for computational purposes. This leads to the following architecture to support the visualisation
of data at the point of care (in the health facility) computed from data produced and reposited in the health
facility (internal dashboard) as well as data aggregated through data visiting from health facilities in VODAN-
Africa Network (External Dashboard).
690
数据智能
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
数字 7. Conceptual architecture for data analysis and visualisation of locally produced and reposited machine-
actionable data [51].
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
t
/
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
数字 8. Conceptual architecture for data analysis and visualisation of locally produced and reposited machine-
actionable data.
数据智能
691
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
The design of this data infrastructure, as envisaged, will aim to simultaneously serve the purpose of: (我)
informing decisions at the point of care based on the data produced in the facility, 和 (二) 增加
data available for analysis, including at the global level, without compromising the ownership of the data.
While all personal data remain within the facility, the aggregate data is obtained by federated computations
through data visiting and can be shared in aggregate form as this data is depersonalised and de-identified.
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
数字 9. Accessibility spectrum of processed personal data [50].
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
t
.
/
我
The second phase is being rolled out with the participation of Leiden University and over 80 健康
facilities in 8 countries in Africa.
For future design the architecture will make better use of the machine-actionable semantic enrichment
数据的, by storing of the data in a triple store and to install through docker to maximise flexibility of
operation and allow dynamic queries, all within the agreed access and permission control associated with
regulatory frameworks in each place.
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
8. 结论
The analysis of the evolution of the COVID-19 pandemic in Africa suffers from incomplete data. 这
negatively impacts on the capacity to adequately respond to COVID-19 at the point of care. Data partitioned
as averages per country, based on limited samples, hide the variations across countries and communities.
Few population studies within Africa have been carried out with a representative research design or sampling
methodology that covers the entire continent.
692
数据智能
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
In this Special Issue, the research network VODAN-Africa investigated the reasons why the availability,
variety and veracity of COVID-19 data from Africa are inadequate. The lack of ownership of the data
produced is reflected in the low degree of relevance of such data to the users. This raises the question:
Would it be possible to enhance data collection in Africa by using the FAIR Guidelines for data production
in health facilities? The studies in this Special Issue found that the FAIR Guidelines are aligned with policy
directions in all of the countries that were studied, which is confirmed by the FAIR-Equivalency of their
regulatory frameworks.
In current research paradigms, digital health data is extracted from health facilities without rendering any
sustainable use of the data by the facilities for improvement of quality of care at the point of care. 在
添加, digital health applications suffer from a vertical architecture that does not prioritise the horizontal
integration of data inside health facilities. To make data relevant, information flows in health facilities need
to be redirected to make use of the facility central to the purposing of such data. 为了测试这个, the team at
VODAN-Africa conducted a data visiting experiment of data produced as machine actionable, curated and
reposited in location and visited with computational queries over the Internet. With this, the proof of
concept of data visiting was successfully established.
The studies in this Special Issue looked at whether or not a data architecture based on Findable, Accessible,
Interoperable and Reusable (FAIR) data would provide opportunities for horizontal research data integration,
linking together data from multiple studies into a sustainable data ecosystem. A FAIR Equivalency analysis
of regulatory frameworks showed a positive inclination to embrace the FAIR Guidelines in the studied
非洲国家, revealing the potential for new data governance paradigms that enable more equitable
international research cooperation within the health domain. 因此, it can be concluded that the FAIR
concept could help envision a design that would protect data ownership and enable data use within the
health facilities, while simultaneously allowing data analysis across facilities through data visiting. A
successful proof of concept of data visiting across two continents, Africa and Europe, was carried out. 这
assessment of the first research phase suggests specifications and requirements for further development.
These include the co-creation of the inclusive innovation process with designers based in Africa, 更多的
flexibility to adapt ontology-based metadata specifications according to the research design to various
workflows in different health facilities in Africa and the capacity building to curate data as machine
actionable semantic objects.
In a further assessment, it was found that adaptations were necessary to construct an architecture that
would be useable in health facilities with adaptability to the operational variations in the clinics. A second
phase has started based on the conclusions drawn from the first phase. This second phase is based on a
collaboration between VODAN-Africa, Leiden University and Stanford University to develop a localised
version of the software developed by CEDAR.
Compliance with regulatory frameworks and GDPR-based personal data protection provide a strong
foundation to defend data privacy. The proposed VODAN architecture employs the FAIR Guidelines as the
conceptual framework to inform the design of a localised data curation and repositing of (病人) 健康
数据智能
693
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
/
t
.
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
数据, useable for data analysis within the facilities. This enables collaboration while retaining data in a
strong framework of ownership, control and retention of data where data is produced. The architecture is
enhanced with data visiting capability to create a more comprehensive set of data from varied places in
非洲, available for multiple site data analytics.
ACKNOWLEDGEMENTS
We would like to thank Misha Stocker for managing and coordinating this Special Issue (体积 4) 和
Susan Sellars for copyediting and proofreading. We would also like to acknowledge VODAN-Africa, 这
Philips Foundation, the Dutch Development Bank FMO, CORDAID, and the GO FAIR Foundation for
supporting this research.
AUTHORS’ CONTRIBUTIONS
Mirjam van Reisen conceptualised this article, wrote the first and second drafts, and approved the final
草稿. Francisca Onaolapo Oladipo contributed to the research reported in this article. Mouhamed
Mpezamihigo provided support for the coordination of the research reported in this article. Ruduan Plug
conceptualised key ideas for this article and provided the architecture for elements of the research reported.
Mariam Basajja carried out research concerning the problem explored in this article and conceptualised
the methodology of FAIR Equivalency reported in this article. Aliya Aktau coordinated the capacity building
of researchers in the research group that carried out the work for this article. Putu Hadi Purnama Jati
coordinated the work with the health facilities and stakeholders in each of the participating countries,
conducted the comparison of FAIR Equivalency in six countries, and wrote the text and the table of results.
Reginald Nalugala provided ideas on the adoption strategy within Kenya. Sakinat Folorunso provided
expertise on the use of the FAIR data model. Samson Yohannes Amare conducted research on the
requirements for the innovation reported on in the article. Ibrahim Abdulahi provided insights into the
adoption potential in Nigeria. Oluwole Olumuyiwa Afolabi provided expertise in the realisation of
the software adaptation to localised use in African countries. Ezra Mwesigwa provided expertise on the
visualisation of data and the architecture to link locally reposited data to dashboards. Getu Tadele Taye
researched the potential to work with the DSW and CEDAR platform in health facilities. Abdulahi Kawu
(a data steward) carried out research. Meriem Ghardallou was in charge of investigating the inclusion of
scientific data on COVID-19 prevalence in the architecture. Yan Liang worked on an early architecture
for the solution discussed in this article. Obinna Osigwe assisted in regular reporting on research outcomes.
Araya Abrha Medhanyie coordinated research between digital health and computer science experts.
Munyarazdi Mawere made comments on the article.
CONFLICT OF INTEREST
All of the authors declare that they have no competing interests.
694
数据智能
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
t
/
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
ETHICS STATEMENT
Tilburg University, Research Ethics and Data Management Committee of Tilburg School of Humanities
and Digital Sciences REDC#2020/013, 六月 1, 2020-可能 31, 2024 on Social Dynamics of Digital Innovation
in remote non-western communities
Uganda National Council for Science and Technology, Reference IS18ES, 七月 23, 2019-七月 23, 2023
参考
[1] Amnesty International: COVID-19: Omicron variant must spur world leaders to share vaccines. [在线的].
Amnesty International (2021). Available at: https://www.amnesty.org/en/latest/news/2021/12/covid-19-
omicron-variant-must-spur-world-leaders-to-share-vaccines/. Accessed 14 十二月 2021
[2] NICD: New COVID-19 variant detected in South Africa [在线的]. National Institute for Communicable
Diseases (25 十一月 2021). Available at: https://www.nicd.ac.za/new-covid-19-variant-detected-in-
south-africa/. Accessed 12 十二月 2021
[3] WHO: Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern [在线的]. World Health
组织(26 十一月 2021). 可用于: https://www.who.int/news/item/26-11-2021-classification-
of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern. Accessed 12 十二月 2021
[4] Maeda, Justin M., Nkengasong, John N.: The puzzle of the COVID-19 pandemic in Africa. 科学 371
(6524), 27–28 (2021). DOI: 10.1126/science.abf8832
[5] Wadvalla, Bibi-Aisha: How Africa has tackled COVID-19. BMJ 370, m2830 (2020). http://dx.doi.org/10.1136/
bmj.m2830
[6] Mbow, M。, Lell, B., Jochems, S.P., 等人。: COVID-19 in Africa: Dampening the storm? 科学 369(6504),
624–626 (2020). DOI: 10.1126/science.abd3902
[7] AIV: The Netherlands and the global approach to COVID-19. Letter, Advisory Council on International Affairs
(AIV), The Hague (2020)
[8] Nyamnjoh, Francis B.: A post-COVID-19 fantasy on incompleteness and conviviality. 在: C. Besteman, H.
Cabot, 乙. Kalir (编辑), Post-COVID fantasies, American Ethnologist (27 七月 2020). Available at: https://
americanethnologist.org/features/pandemic-diaries/post-covid-fantasies/a-post-covid-19-fantasy-on-
incompleteness-and-conviviality. Accessed 9 十二月 2021
[9] Häikiö, J。, Koskela-Huotari, K.: Bridging the gap between technical and human elements in digital service
创新. 在: BLED 2014 会议记录 14 (2014). 可用于: https://aisel.aisnet.org/bled2014/14. Accessed
9 十二月 2021
[10] Buskens, 我。, Van Reisen, M。: Theorising agency in ICT4D: Epistemic sovereignty and transformation-in-
联系. 在: 中号. Mawere (编辑。), Underdevelopment, Development and the Future of Africa, Langaa RPCIG,
Bamenda, PP. 394–432 (2016).
[11] WHO: WHO coronavirus (COVID-19) dashboard [在线的]. 世界卫生组织 (日期不详。). 可用于:
https://covid19.who.int/. Accessed 9 十二月 2021
[12] John Hopkins University: COVID-19 dashboard [在线的]. Coronavirus Resource Center (2021). 可用于:
https://coronavirus.jhu.edu/map.html. Accessed 9 十二月 2021
[13] The Conversation: Data map: Tracking COVID-19 waves in Africa [在线的]. The Conversation Media Group
(2 十一月 2021). Available at: https://theconversation.com/data-map-tracking-covid-19-waves-in-
africa-170884. Accessed 9 十二月 2021
[14] Humdata: Novel coronavirus (COVID-19) cases data [在线的]. Humanitarian Data Exchange (HDX) (日期不详。).
Available at: https://data.humdata.org/dataset/novel-coronavirus-2019-ncov-cases Accessed 9 十二月
2021
数据智能
695
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
.
t
/
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
[15] 泰勒, L。, Broeders, D .: In the name of development: 力量, profit and the datafication of the global South.
Geoforum 64, 229–237 (2015). http://dx.doi.org/10.1016/j.geoforum.2015.07.002
[16] Tai, D.B.G., Shah, A。, Doubeni, C.A., Sia, I.G., Wieland, M.L.: The disproportionate impact of COVID-19 on
racial and ethnic minorities in the United States. Clinical Infectious Diseases 72(4), 703–706 (2021)
[17] Sze, S。, Pan, D ., Nevill, C.R., 等人。: Ethnicity and clinical outcomes in COVID-19: A systematic review and
meta-analysis. EClinical Medicine 29, 100630 (2020). DOI: 10.1016/j.eclinm.2020.100630
[18] Spivak, G.C.: “Can the subaltern Speak?” (Revised edition). 在: R.C. 莫里斯 (编辑。), Can the Subaltern Speak?:
Reflections on the History of an Idea, 哥伦比亚大学出版社, PP. 21–78 (2010). 可用于: http://万维网.
jstor.org/stable/10.7312/morr14384.5. Accessed 24 十二月 2021
[19] Van Reisen, M。, Oladipo, F。, Stokmans, M。, Mpezamihigo, M。, Folorunso, S。, Schultes, E., 等人。: Design of a
FAIR digital data health infrastructure in Africa for COVID-19 reporting and research. Advanced Genetics 2(2)
(2021). 土井: 10.1002/ggn2.10050
[20] Wilkinson, M.D., Dumontier, M。, Aalbersberg, I.J., Appleton, G。, Axton, M。, Baak, A。, 等人。: The FAIR guiding
principles for scientific data management and stewardship. Scientific Data 3(1), 1–9 (2016). http://万维网.
nature.com/articles/sdata201618
[21] Björklund, T.A.: Initial mental representations of design problems: Differences between experts and novices.
Design Studies 34(2), 135–160 (2013). https://doi.org/10.1016/j.destud.2012.08.005.
[22] Sanders, L。: On modeling: An evolving map of design practice and design research. Interactions 15(6), 13–17
(2008). https://interactions.acm.org/archive/view/november-december-2008/on-modelingan-evolving-map-
of-design-practice-and-design-research1
[23] Kingdon, J.W.: Agendas, 备择方案, and public policies. HarperCollins Publishers, 纽约 (1984)
[24] ACM Web Science Conference, University of Southampton, Association for Computing Machinery, &
Association for Computing Machinery: WebSci ’20: 12th ACM Conference on Web Science Companion, 七月
6–10, 2020, 南安普敦, 英国, Association for Computing Machinery (ACM), 纽约, 纽约
(2020). https://doi.org/10.1145/3394332.3402823
[25] Alliance for Accelerating Excellence in Science in Africa (AESA): Recommendations for data and biospecimen
governance in Africa. ASP Policy Paper 3, African Academy of Sciences (2021). 可用于: https://万维网.
aasciences.africa/sites/default/files/Publications/Recommendations%20for%20Data%20and%20
Biospecimen%20Governance%20in%20Africa.pdf. Accessed 13 可能 2021.
[26] European Parliament and Council of the European Union: Regulation (欧洲联盟) 2016/679 of the European
Parliament and of the Council of 27 四月 2016, on the protection of natural persons with regard to the
processing of personal data and on the free movement of such data, and repealing Directive 95/46/EC
(General Data Protection Regulation). Official Journal of the European Union L119/1, PP. 1–88 (2016).
可用于: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016R0679&rid=2. Accessed
7 九月 2021
[27] Bauer, J。, Petroni, M.J.: Chapter 7. Data Ethics Guidebook [在线的]. Causeit Guide to Digital Fluency, Digital
Fluency (2018). Available at: https://www.digitalfluency.guide/data-ethics/data-sovereignty-and-data-politics.
Accessed 13 十二月 2021
[28] Techopedia: Data Sovereignty [在线的]. Technopedia (7 九月 2021). Available at: https://万维网.
techopedia.com/definition/33304/data-sovereignty. Accessed 13 十二月 2021
[29] African Union: The digital transformation strategy for Africa (2020–2030). African Union, 亚的斯亚贝巴(埃塞俄比亚首都 (日期不详。).
可用于: https://au.int/sites/default/files/documents/38507-doc-dts-english.pdf. Accessed 22 十二月
2021
[30] Plug, R。, Liang Y., Aktau, A。, Basajja, M。, Oladipo, F.O., Van Reisen, M。: Terminology for a FAIR Framework
for the Virus Outbreak Data Network-Africa. 数据智能 4(4), 698–723 (2022)
[31] Stocker, M。, Stokmans, M。, Van Reisen, M。: Agenda setting on FAIR Guidelines in the European Union and
the role of expert committees. 数据智能 4(4), 724–746 (2022)
696
数据智能
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
t
/
.
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3
Incomplete COVID-19 Data: The Curation of Medical Health Data by the Virus Outbreak Data
Network-Africa
[32] 林, Y。, Purnama Jati, P.H., Aktau, A。, Ghardallou, M。, A。, Nodehi, S。, Van Reisen, M。: Implementation of FAIR
Guidelines in selected non-Western geographies. 数据智能 4(4), 747–770 (2022)
[33] Basajja, M。, Van Reisen, M。, Oladipo, F.O.: FAIR Equivalency with regulatory framework for digital health in
乌干达. 数据智能 4(4), 771–797 (2022)
[34] Purnama Jati, P.H.: FAIR Equivalency in Indonesia’s digital health framework. 数据智能 4(4), 798–812
(2022)
[35] Taye, G.T., Amare, S.Y., Tesfit, G.G, Medhanyie, A.A., Ayele, W., Habtamu, T。, Van Reisen, M。: FAIR
Equivalency with regulatory framework for digital health in Ethiopia. 数据智能 4(4), 813–826 (2022)
[36] Chindoza, K.: Regulatory framework for eHealth data policies in Zimbabwe: Measuring FAIR Equivalency.
数据智能 4(4), 827–838 (2022)
[37] Kawu, A.A., 约瑟夫, E., Abdullahi, 我。, Maipanuku J., Folorunso, S。, Basajja, M。, Oladipo, F.O., Ibrahim, H.L.:
FAIR Guidelines and data regulatory framework for digital health in Nigeria. 数据智能 4(4), 839–851
(2022)
[38] Thea, E.I., Nalugala, R。, Nandwa, W., Obwanda, F。, Wachira, A. Cartaxo, A.M.: FAIR Equivalency, 监管
framework and adoption potential of FAIR Guidelines in health in Kenya. 数据智能 4(4), 852–866
(2022)
[39] Purnama Jati, P.H., 林, Y。, Nodehi, S。, Cahyono, D.B., Van Reisen, M。: FAIR versus open data: A comparison
of objectives and principles. 数据智能 4(4), 867–881 (2022)
[40] GO FAIR: FAIR Principles [在线的]. 可用于: https://www.go-fair.org/fair-principles/. Accessed 30 四月
2020
[41] Basajja, M。, Nambobi, M。: Information streams in health facilities: The case of Uganda. 数据智能
4(4), 882–898 (2022)
[42] Basajja, M。, Nambobi, M。, Wolstencroft, K.: Possibility of enhancing digital health interoperability in Uganda
through FAIR data. 数据智能 4(4), 899–916 (2022)
[43] Basajja, M。, Suchanek, M。, Taye, G.T., Amare, S.Y., Nambobi, M。, Folorunso, S。, Plug, R。, Oladipo, F.O., 货车
Reisen, M。: Proof of concept and horizons on deployment of FAIR Data Points in the COVID-19 pandemic.
数据智能 4(4), 917–937 (2022)
[44] Purnama Jati, P.H., Van Reisen, M。, Flikkenschild, E., Oladipo, F.O., Meerman, B., Plug, R。, Nodehi, S。: 数据
使用权, 控制, and privacy protection in the VODAN-Africa architecture. 数据智能 4(4), 938–954
(2022)
[45] Ghardallou, M。, Wirtz, M。, Folorunso, S。, Touati, Z。, Ogundepo, E., Smits, K., Mtiraoui, A。, Van Reisen, M。:
Expanding non-patient COVID-19 data: Towards the FAIRification of migrants’ data in Tunisia, Libya and
Niger. 数据智能 4(4), 955–970 (2022)
[46] Folorunso, S。, Ogundepo, E.A., Basajja, M。, Awotunde, J.B., Kawu, A.A., Oladipo, F.O., Abdullahi, 我。: FAIR
machine learning model pipeline implementation of COVID-19 data. 数据智能 4(4), 971–990 (2022)
[47] Oladipo, F.O., Folorunso, S。, Ogundepo, E.A., Osigwe, E., Akindele, A.T.: Curriculum development for FAIR
data stewardship. 数据智能 4(4), 991–1012 (2022)
[48] Akindele, A.T., Tayo, A.O., Taye, G.T., Amare, S.Y., Van Reisen, M。, Berhe, K.F., Gusite, B., Edozie, E.: 这
impact of COVID-19 and FAIR data innovation on distance education in Africa. Data Intelligence 4(4),
1013–1032 (2022)
[49] Jacobsen, A。, Kaliyaperumal, R。, da Silva Santos, L.O.B., Mons, B., Schultes, E., Roos, M。, 汤普森, M。: A
generic workflow for the data FAIRification process. 数据智能 2(1–2), 56–65 (2020)
[50] Plug, R。, 梁, Y。, Basajja, M。, Aktau, A。, … Van Reisen, 等人。: FAIR and GDPR compliant population health
data generation, processing and analytics. Semantic Web Applications and Tools for Healthcare and Life
科学 (2022, 即将推出)
[51] Plug, R。: Presentation. Unpublished (2022)
数据智能
697
我
D
哦
w
n
哦
A
d
e
d
F
r
哦
米
H
t
t
p
:
/
/
d
我
r
e
C
t
.
米
我
t
.
e
d
你
d
n
/
我
t
/
我
A
r
t
我
C
e
–
p
d
F
/
/
/
/
4
4
6
7
3
2
0
6
3
8
2
6
d
n
_
e
_
0
0
1
6
6
p
d
t
.
/
我
F
乙
y
G
你
e
s
t
t
哦
n
0
7
S
e
p
e
米
乙
e
r
2
0
2
3