Victoria Hale
Seeking a Cure for Inequity in
Access to Medicines
Innovations Case Narrative:
The Institute for OneWorld Health
The top five infectious disease killers in the world are HIV/AIDS, tuberculosis,
malaria, respiratory infections, and diarrhea. None of these, not even HIV/AIDS,
has received sufficient focus by the pharmaceutical industry to meet global health
necesidades. Though these diseases have severe global social and economic conse-
quences, very few effective treatments are available. Más, there are insufficient
incentives for industry to invest in developing new safe, affordable and effective
tratos.
Encima 60% of the world’s population lives in the places where these infectious
diseases are most prevalent: the tropics. These regions in the middle band around
the globe—places such as sub-Saharan Africa, the Indian sub-continent, South
Asia Oriental, and parts of Latin America—have high population densities, high pover-
ty rates and climates that are favorable to insects that transmit disease. Each year,
millions of lives are lost to infectious diseases.
Por qué, in the 21st century, is it that some places in the world people can get med-
ical treatment for nearly any condition, or even for a mere complaint, while in
other places millions of children die from diarrhea?
The reason is simple. The therapeutic drugs that exist today are produced by
Victoria Hale is founder and chief executive officer of the Institute for OneWorld
Salud (iOWH). Dr. Hale has been elected to membership in the Institute of Medicine
of the National Academies, is the recipient John D. and Catherine T. MacArthur
Foundation Fellow (2006), and has been selected as an Ashoka Fellow. She received
the Executive of the Year by Esquire Magazine (2005), The Economist Innovation
Award for Social and Economic Innovation (2005), and the Skoll Award for Social
Entrepreneurship from the Skoll Foundation (2005). Dr. Hale established her
expertise in all stages of biopharmaceutical drug development at the US Food and
Drug Administration (FDA) and at Genentech, Cª, the world’s first biotechnology
in Pharmaceutical Chemistry from the
company. Dr. Hale earned her Ph.D.
University of California, San Francisco. The Schwab Foundation for Social
Entrepreneurship has recognized Victoria Hale as an Outstanding Social
Entrepreneur.
© 2007 Victoria Hale
innovaciones / caer 2007
59
Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023
Victoria Hale
for-profit pharmaceutical companies. These companies operate according to a very
strict business model that requires a certain return on investment to shareholders
for any project undertaken. Adhering to this business model leads these companies
to pursue drugs for wealthy countries, focusing on heart disease, diabetes, cancer
and so-called ‘lifestyle’ drugs. These targets of opportunity are consistently more
appealing than taking on the
challenge of
treating tropical
in places
infectious diseases
where other challenges, such as
the lack of markets and distribu-
tion networks, also exist.
[F]ully one-third of the
world’s population lacks
access to essential medicines,
and in the poorest regions of
Africa and Asia, this figure
rises to one-half.
Como consecuencia, fully one-
third of the world’s population
lacks access to essential medi-
cines, and in the poorest regions
of Africa and Asia, this figure
rises to one-half. Between 1975
y 1999, out of 1,393 new drugs
13 eran
solo
desarrollado,
designed to treat tropical diseases. That is less than 1 por ciento, even though tropi-
cal diseases account for more than 90 percent of the worldwide disease burden.
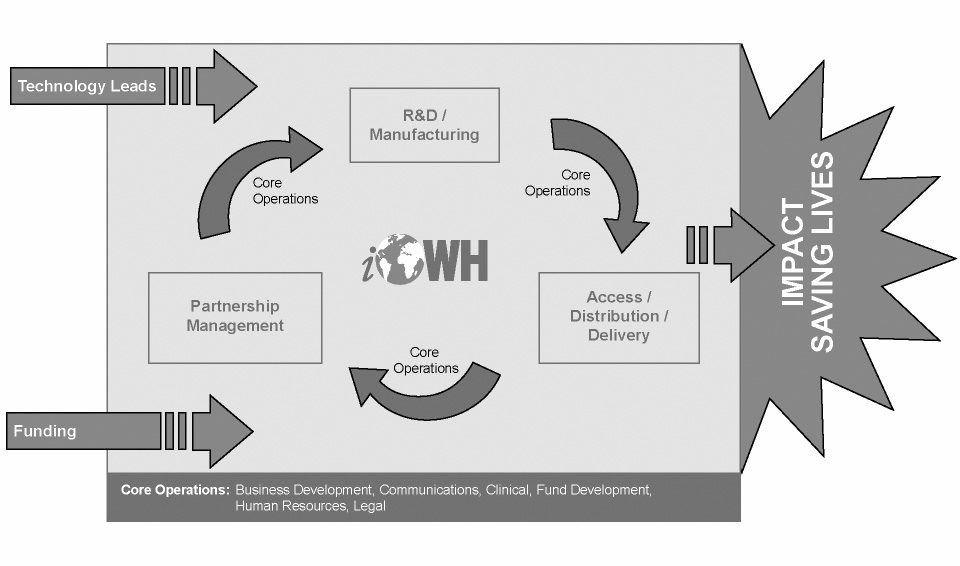
More broadly, solo 10 percent of the US$70 billion spent on health research world- wide each year is for research into the health problems that affect 90 percent of the world’s population. The idea behind the Institute for OneWorld Health is to look at this so-called “90/10 gap” as evidence not only of past failure, but also of future opportunity. Without question, pharmaceutical companies need to make profits to make drugs. The research that goes into discovery, diseño, and testing for safety and efficacy is expensive. If we can find ways to redirect back to global health even a fraction of the intellectual property and human resources of the global pharmaceutical com- munity, we can make a real difference. That is our aim. Hoy, iOWH has a staff of 80, in offices in the US and in India, with the sci- entific and policy expertise needed to identify new drug opportunities, develop a target product profile, produce a product development plan, and shepherd drugs through various regulatory approval processes. iOWH also has an array of research and development partnerships that work to develop a range of products for a vari- ety of diseases. And we have formed the partnerships needed to manufacture and deliver the medicines. THE BEGINNING: “YOU HAVE ALL THE MONEY” Back in 2000, I was riding in a taxi and chatting with the driver, an African immi- grant. He asked me what I did for a living. I am very proud of the work I do so I was happy to tell him that I am a pharmaceutical scientist. I was taken aback when 60 innovaciones / caer 2007 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Seeking a Cure for Inequity in Access to Medicines he responded by breaking out into a fit of laughter. When he finally regained his composure, he remarked with a shake of his head: “You guys have all the money.” All the money, Sí. But to what end? His comment crystallized the growing dis- comfort I had felt at the imbalance of resource allocation that was so evident in my chosen field of work. I recalled another moment of troubling introspection I had experienced not long before, while I was working at the Food and Drug Administration. I came to realize that up to one in five children in sub-Saharan Africa does not live to see their fifth birthday. And each year in the developing world, 10 million people die from neglected diseases—diseases for which no effec- tive treatments exist, nor are any in development. After my taxicab epiphany, I had an increasingly difficult time keeping these numbers out of my head. The pride I felt in being a pharmaceutical scientist became overwhelmed by feelings of shame and embarrassment at being part of an industry that was not taking full responsibility for the diseases of the world. I thought to myself, if there is anything that I can do personally to change things, how can I not do it? In further considering the problem, I began to wonder if it might be possible to take the profit imperative out of the drug development equation. Could I create a process for developing drugs, including testing them and getting them approved and manufactured, that would make them as safe and effective as any blockbuster drug, but affordable enough for the poorest of the poor? Is it possible to organize pharmaceutical development around the objective of human impact rather than profitability? I resigned from my position at Genentech and I took two years to simply con- sider the parameters of the challenge. Traveling around the world was an eye-open- ing experience, helping me better define the questions in mind and confirming my deep commitment to my pursuit. After a great deal of time and expense, I began to see a way forward. In July 2000 I founded the Institute for OneWorld Health (iOWH), an entire- ly new kind of pharmaceutical company. THE EXPERIMENT: A NON-PROFIT PHARMACEUTICAL COMPANY The pharmaceutical scientists who work at iOWH share a belief that their work can change the world and save lives. Of the many possible paths one could imag- ine toward this goal, the one we have taken is the development of a non-profit pharmaceutical company focused on neglected diseases. It is not possible for a non-profit pharmaceutical company to follow the stan- dard big pharma business model. The big pharma model typically starts with basic science and discovery in the laboratory and exploring educated choices. When promising results are identified, they are taken through the lengthy and expensive process of drug formulation and sequential testing in petri dishes, animals, and humans. Solo 1 drug in 10,000 that is discovered actually makes it to clinical tri- como. Solo 1 drug in 10 that makes it to human testing makes it to the market. innovaciones / caer 2007 61 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Victoria Hale Compounding the risk, of the few drugs that actually reach the market, 70% fail to recoup their R&D investments. In many cases, drugs are cast aside by standard, for-profit pharmaceutical firms for reasons having nothing to do with their potential to benefit people. Por ejemplo, some drugs are simply not profitable in any known application. Others may not compete successfully with other known candidates for a given disease. Still others are discarded because they have unacceptable side effects for the population the drug will treat, but may be acceptable for other populations. (Por ejemplo, a new antibiotic that causes sleepiness may be unacceptable for people who need to drive or go to work while taking the drug. But for a malaria patient or for a bedrid- den patient facing certain death from an infectious disease, sleepiness may be a perfectly acceptable side effect.) iOWH has sought a different path. For starters, we do not operate any of our own laboratories. En cambio, we have pursued a strategy of networked innovation, with an emphasis on streamlining the traditional process of bringing drugs to market. We streamline in many ways, of which partnership is the most important. We partner with investigators in the public and private sector to discover new compounds with potential for treating neglected diseases. We partner with for- profit pharmaceutical companies to find opportunities to match their cast-offs— abandoned, discontinued or no longer profitable drugs—with neglected diseases. And we partner with manufacturers, non-government organizations (ONG), and local infrastructure service providers to manufacture drugs and deliver them to patients. Our core operations involve using our R&D experience to coordinate and collaborate with these partners and, most importantly, identifying the technologi- cal leads and securing the funding to create—and seize—opportunities to save lives. [See Figure 1: Funding Model] We also aim to streamline the clinical trials process wherever possible. This of course does not imply that we cut corners in terms of safety. Bastante, if we don’t need to do as many trials—perhaps because our drugs do not compete with exist- ing drugs—then we don’t. Finding a late-stage drug to take over the finish line enables us to get the most from our investments. También, when we bring a drug to a developing country’s regulatory agencies, we work together with the agency to find the most straightforward path to satisfying the regulatory requirements that will prove safety and efficacy. Por último, we still have to do many studies, just as any other pharmaceutical company must do, and these studies can cost tens of millions of dollars. These costs have been one of the biggest challenges to our model. What replaces profit when you remove it from the equation? We account for success in human terms and we value each life equally rather than weighted in terms of abil- ity or willingness to pay. We were working for the same global public health out- comes as philanthropic organizations like the Bill and Melinda Gates Foundation. We were pioneering a new business model that groups like the Skoll Foundation and Schwab Foundation were looking to foster. Philanthropic funds would be our 62 innovaciones / caer 2007 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Seeking a Cure for Inequity in Access to Medicines Core Operations: Business Development, Clinical, Comunicaciones, Fund Development, Human Resources, Legal Figure 1. The Funding Model. main source of revenue, and capital would be put to work to achieve a social return on investment. But a shared sense of mission alone was not enough to persuade our current partners at the Gates Foundation and elsewhere to support us in the earliest stages of our development. What was required at the outset was a setting that would enhance our prospects for success, enabling us to overcome the scientific, financial, regulatory, and even political hurdles inherent in the development of drugs for neglected diseases. For OneWorld Health, that setting was Bihar, India. The disease was visceral leishmaniasis (VL), also known as “black fever” or Kala-Azar. MATCHING PROMISING DRUGS WITH NEGLECTED DISEASES Paromomycin is an antibiotic developed by Pharmacia (now Pfizer), which was discontinued in the 1970s because oral antibiotics came to market and its patent had expired. This drug rose to the top of our list of drugs to treat neglected dis- eases because it had such great potential. It had been a very effective and safe antibiotic, so much of the expensive testing had already been completed. Además, an African researcher had discovered that paromomycin had a powerful effect on a disease called Visceral Leishmanaisis, a fatal disease for which safe, effec- tive and affordable treatment options were urgently needed. Como consecuencia, Pharmacia granted the rights to paromomycin to the World Health Organization (WHO). The WHO had put efforts into using paromomycin to treat VL, but ulti- mately abandoned the program. VL is the second most deadly parasitic disease in the world. It is a devastating innovations / caer 2007 63 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Victoria Hale affliction. Caused by a parasite spread by a common insect in the tropics called the sand fly, the disease attacks the bone marrow and destroys the body’s ability to pro- duce red and white blood cells. This leaves the patient extremely vulnerable to infection. Similar to AIDS patients, those with Kala-Azar almost always die of an infection they simply cannot fight. I visited with patients suffering from Kala-Azar in Bihar, India where it is most prevalent, though the disease is also common in Nepal, Bangladesh, the Horn of Africa and Brazil. This region of India hosts the poorest of people who have been experienced famine years of their lives. Those afflicted with the disease are emaci- ated except for their large bellies, where the parasite hides, enlarging the liver and spleen. Witnessing the consequences of this illness was an indelibly marking expe- rience. In Bihar, a hundred million people are at risk for Kala-Azar. Approximately 1.5 million people are infected with the disease. There are approximately 500,000 new cases and 300,000 deaths each year. Existing therapies are so expensive that fami- lies have been put three generations into debt to treat and save a relative. en contra- contraste, the promise of paromomycin was a cure from Kala-Azar for about US$10 –
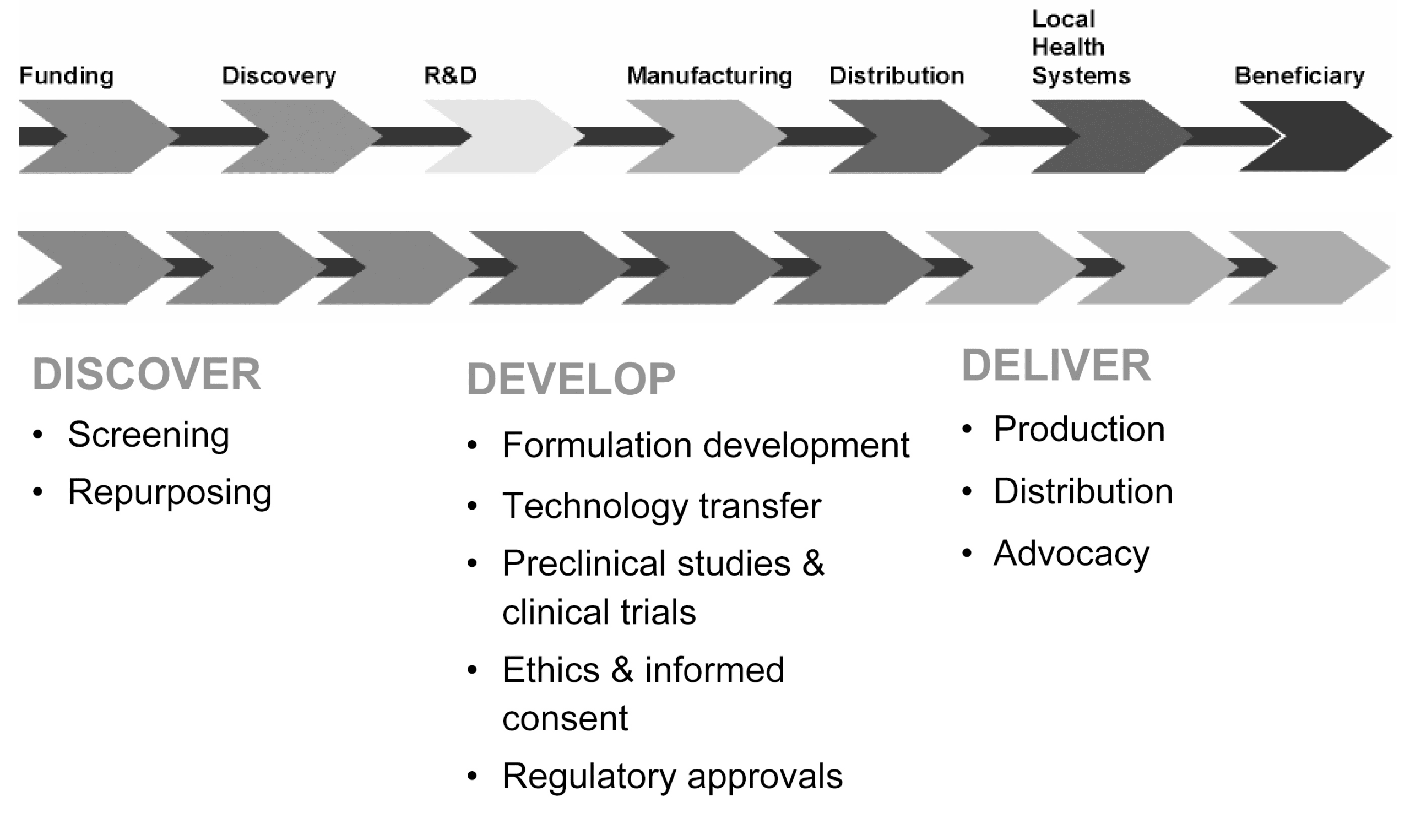
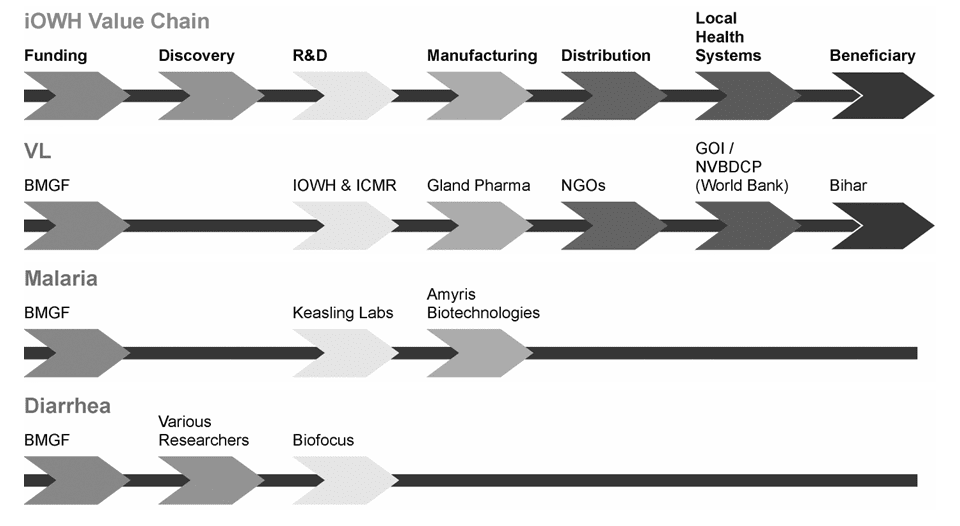
$20. Because my staff and I had experience with drug development and the regula- tory process in various settings around the world, we entered into the project with full awareness of the obstacles that faced us in seeking to turn paromomycin into a drug for Kala-Azar, and then getting it approved. Among the many obstacles, one had more to do with politics than science: it might be termed the “Constant Gardener” factor. The Constant Gardener, a novel by John le Carre, tells the tale of a multinational drug company that took advantage of the political vulnerability of a particular group of people in Africa to test a new drug with known adverse con- sequences. Precisely because the novel reflects aspects of reality and past experi- ence, Western pharmaceutical companies seeking to test drugs on populations in poor places anywhere in the world are often received immediately with suspicion. Lack of trust makes such projects difficult for for-profit pharmaceutical compa- nies—in some cases, simply infeasible. We also came to Bihar as outsiders. But we came with a goal not of increasing the value of shares, but instead sharing the value of cures. With our public health mission irrevocably encoded into our non-profit form of organization, we were able to overcome the Constant Gardener factor. The mutual trust that we cultivat- ed over a period of time with the government of India allowed us to move forward with our trials even in the most challenging rural environments in Bihar. Reaching our initial goal—conducting clinical trials in Bihar for treatment of VL—took four years. Cuando, at last in 2004, I went to a hospital in India during a trial of our drug, the experience was exciting but also frightening. We had one chance to get this right and show that we could repurpose a drug to treat a disease the world had forgotten. To fail would in some ways be worse than not having tried at all, as we would potentially discourage future efforts. Seeing patients treated with our drug suddenly sitting up, awake, aware, even hungry, provoked an inde- 64 innovaciones / caer 2007 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Seeking a Cure for Inequity in Access to Medicines scribable feeling of elation. We submitted the drug to the Indian government for regulatory approval in 2006. In August of 2006, the Paromomycin IM Injection was approved by the Drug Controller General of India for the treatment of Visceral Leishmaniasis. The approval of Paromomycin IM Injection came less than three months after the sub- mission of the application for approval, which was prepared by iOWH in collabo- ration with our partner, Hyderabad-based drug manu- facturer Gland Pharma Limited. The drug is expected to be a key tool for India’s National Vector Borne Disease Control Program (NVBDCP), which aims to rid the country of leishmaniasis by 2010. We also expect the drug will be used in disease control programs in other leishmania- sis-endemic countries. Gland Pharma will make the medicine available at cost, for approxi- mately $10 -$20 per treatment course, a significantly lower price than currently approved leishmaniasis therapies with marginal efficacy and severe toxicities. In August of 2006, the Paromomycin IM Injection was approved by the Drug Controller General of India for the treatment of visceral leishmaniasis (VL), the medical name for Kala-Azar. While we saw the approval of Paromomycin IM Injection for treatment of leishmaniasis as a sufficient proof-of-concept for a non-profit pharmaceutical model, the following months brought further validation of our work. In May 2007 the WHO announced the inclusion of Paromomycin IM Injection on their list of Essential Medicines. Entonces, in June 2007 the New England Journal of Medicine pub- lished our Phase 3 clinical trial results. THE PHARMACEUTICAL VALUE CHAIN For all the milestones we reached and the corresponding sense of accomplishment we experienced in 2006, we also ended the year facing a stark reality: it is one thing to develop and manufacture a drug that works, but it is quite another to get that drug to those who need it. As difficult as it is to discover a promising approach and then develop a drug, the final stage of delivering treatment can be the most diffi- cult. Drug distribution must be done by local healthcare workers in local clinics. It involves getting the drug to the right places, storing it safely, administering it to people who have been properly diagnosed, and finally, monitoring patients close- ly for safety and treatment results. In the case of Kala-Azar, our strategy of matching an orphaned drug to a neg- lected disease had worked, but it remained unfinished. As we sought avenues for addressing the challenge of delivery, we began to broaden our thinking about how innovations / caer 2007 65 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Victoria Hale to approach the challenge of reducing inequities in treatment. It became clear to us that, in order to have our desired impact, we would need to develop the capa- bility to engage at multiple stages along the pharmaceutical value chain. [See Figure 2. The Pharmaceutical value chain] In the case of paromomycin and visceral leishmaniasis, we started out in the late stages of research and development with our Phase 3 ensayos. [See Figure 3. Placing iOWH Initiatives Along the Value Chain.] Then we partnered with Gland Pharma and the International Dispensary Association (AIF) for manufacturing. Ahora, we are working on a plan to distribute and deliver those drugs to the benefi- ciaries, the people of Bihar and South Asia more broadly. To test our plan, we opened a liaison field office in the capital city of Patna in Bihar, India to oversee a Phase 4 pharmacovigilance and access program for the paromomycin treatment, which is administered as a once-a-day injection for 21 días. Working with the principal investigators who are experts in the treatment of visceral leishmaniasis, government and nongovernmental organization (NGO) partners, this Phase 4 Program will investigate the safety and efficacy of treatment with the Paromomycin IM Injection in progressively more rural areas in Bihar. The first module of the program will enroll approximately 500 patients to provide addition- al safety data on the treatment. Over the course of the two-year trial, up to 1500 additional patients will be included in two subsequent access modules that will extend the network of treat- ment facilities, providers, and related logistics systems into the most rural areas of Bihar. This is an innovative access model for administering Paromomycin IM Injection that uses an outpatient setting to diagnose and treat impoverished patients and advanced data transmission technologies for pharmacovigilence in the remote areas where visceral leishmaniasis is endemic. To deliver drugs to these remote and difficult-to-reach locations, iOWH is seeking to make use of existing infrastructure already put in place by an innovative local NGO named Janani. In this model, an existing force of healthcare providers that provide women with prenatal care will use a hub and spoke model to carry drugs from a central location to outlying destinations. We will train the clinicians and rural healthcare providers at local centers in the administration of the drug. The trial is an example of how iOWH is extending its partnerships all the way to the village level. En efecto, our work would be nearly impossible without local part- ners and our in-country presence. When we leave, the work will be carried on by local organizations. While establishing a distribution and delivery network is extremely challeng- ing due to the unpredictable nature of these rural areas and the lack of services in them, this step is also the most critical of all those that iOWH takes in terms of its mission to save lives. Beyond the obvious effect of the drugs and their ability to cure patients, the very existence of the drugs can have a ripple effect in a commu- nity. It brings hope to family members who no longer face the choice between extreme debt and the loss of a family member. It also brings new knowledge and power to clinicians, who can now diagnose people, knowing that there is an acces- 66 innovaciones / caer 2007 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Seeking a Cure for Inequity in Access to Medicines Figure 2. The Pharmaceutical Value Chain. sible cure to their devastating disease. Our goal is to refine an effective and transferable access model, enabling us to saves lives, to bring social change to families and communities and to expand our reach beyond India and into other regions burdened by infectious disease. If we are successful, this new product will build demand for new markets along the way. From the manufacturing center in Hyderabad to the bedsides of patients, this drug will create a demand for transport, delivery, and storage. Local commu- nities become partners with iOWH by providing these services and providing medical care. When a local community becomes healthier both physically and eco- nomically, the result can be a profound and far-reaching. In addition to affecting change in rural areas, projects in this part of our value chain also affect positive change in the developed world by addressing the emerg- ing problem of what we call innovation pile-up. There are so many innovations coming from scientists and engineers who are developing new tools to prevent and treat patients. But getting these drugs and innovations out of the warehouse and to the patient is often the most challenging part of the problem. When this prob- lem isn’t tackled, these innovations pile-up and become a burden and a disap- pointment that could, eventually, squelch the creativity of those scientists who invented them. By building channels for these innovations to flow through, iOWH can help prevent innovation pile-up. innovaciones / caer 2007 67 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Victoria Hale Figure 3. Placing iOWH Initiatives Along the Value Chain. THE DOORS ARE OPEN As we have sought a non-profit approach to working with innovators to find treat- ments for neglected diseases, we have observed a change in the attitudes of our for- profit counterparts. En 2000 y 2001, when we first began talking with pharma- ceutical companies about our vision for a different approach to drug development, the response to the pitch was skeptical, to say the least. We were asking for these companies to surrender to us parcels of hard-won intellectual property. Even if they weren’t using the property, the request was bound to meet with considerable resistance—which it did. Over the past six years, the reception we receive has changed considerably. Pharmaceutical scientists within conventional drug companies understand the challenge we are seeking to address, y, more importantly, can see the value of the approach we propose. Some want to participate in iOWH during a sabbatical or through fellowships. Others offer themselves as voluntary resources to be available to help guide us. Even at the executive level, there is an openness and willingness to talk. We now have access to these companies. They want to know how they can contribute. Where the doors of collaboration appeared less than a decade ago to be shut, today they are open. The result of this turn-around is that it makes our search for the next match- up of an orphaned drug with a neglected disease that much easier. We have two more in the works already. These new partnerships hold the promise of produc- ing therapies that will cure people afflicted with malaria—the most deadly para- sitic disease in the world—and diarrhea. Our malaria program efforts fall solidly on the manufacturing and distribu- tion links of the value chain. We are focusing on developing a supply chain for a 68 innovaciones / caer 2007 Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023 Seeking a Cure for Inequity in Access to Medicines crucial malaria drug ingredient. The project involves a unique three-way partner- ship between the iOWH, the University of California, Berkeley and Amyris Biotechnologies, a for-profit biotechnology company funded by iOWH to accom- plish this program. The partnership leverages new technology from Berkeley pro- fessor Jay Keasling and Amyris Biotechnologies that allows an anti-malarial drug precursor, artemisinic acid, to be manufactured very inexpensively using genetical- ly engineered yeast.1 Prior to that discovery, only plants produced the compound, making it an expensive and unreliable ingredient for a mass-produced drug. Despite this technological advancement, challenges remain. The yield of to forward [I]t is one thing to develop and manufacture a drug that works, but it is quite another to get that drug to those who need it. As difficult as it is to discover a promising approach and then develop a drug, the final stage of delivering treatment can be the most difficult. artemisinic acid will need to be improved further in order to be economically acceptable for large- scale manufacturing. Además, iOWH must guide the resulting drug through regulatory approval and contribute to its effective inte- gration into the global market. We look continued progress this year with Amyris and UC Berkeley toward our goal of introducing microbially-derived semisynthetic artemisinin into Artemisinin-based Combination Therapies (ACTs) por 2010, reduc- ing the cost of ACTs by up to 90%. Our diarrhea program falls on the other end of the value chain. It focuses on discovery. En 2006 la factura & Melinda Gates Foundation awarded us a US$46 million grant to develop wholly new treatments to comple-
ment traditional approaches for fighting diarrhea. Diarrheal diseases are a leading
cause of death in children under the age of five worldwide, killing an estimated 2
million children each year. Typically, children die of dehydration. Therapies exist
that help rehydrate these children, but no effective therapy exists to stem the loss
of fluids in the first place.
Our efforts will focus on developing safe, effective and affordable new anti-
secretory drugs that inhibit intestinal fluid loss. These novel anti-secretory drugs
will be deployed as an adjunct to oral rehydration therapy for the treatment of
acute secretory diarrhea, which is responsible for nearly 40% of reported cases of
diarrheal disease globally. During 2006, the iOWH Diarrheal Disease Program ini-
tiated several new collaborations which include BioFocus DPI, who will apply their
medicinal chemistry and early stage drug development expertise to identify new
anti-secretory drugs, and the International Center for Diarrheal Disease Research
in Bangladesh (ICDDR,B), who will conduct pre-clinical studies.
innovaciones / caer 2007
69
Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023
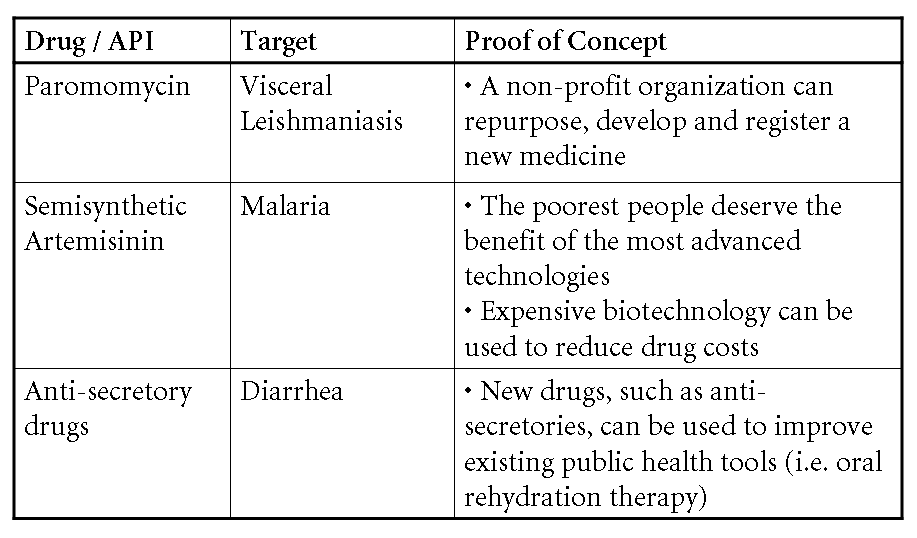
Cifra 4. Proofs-of-concept.
BUSINESS SUSTAINABILITY: THE MONEY CHALLENGE
The business of creating new drugs is slow and expensive. It involves great dili-
gence and care because of both cultural and ethical considerations involved in
treating patients with new medicines. We have proven that our model is effective
[see figure 4: proofs-of-concept], but not yet that it is sustainable. A critical chal-
lenge in our next stage of development will be to transition from exclusive reliance
on philanthropic support and to a model which combines grant-funding with rev-
enues through sales to select subpopulations.
With regard to philanthropic gifts and grants, we are increasingly aware of our
need to develop a funding pipeline to support our products development in each
stage. iOWH could, por ejemplo, invest its funds in identifying good leads for the
Western orphaned disease match-ups with the most potential. We would then
bring these leads and targets to outside funders who would help fund the develop-
ment of the drug, and to a likely different set of partners who would help manu-
facture and distribute it.
With regard to sales, we have started to consider the applicability of a cross-
subsidization strategy: sales of a product to those able to pay can help cover costs
of providing therapies to those unable to do so. The approach is sound and well-
probado. (Ver, Por ejemplo, the case in this issue on the Aravind Eye Hospital.) Mientras
visceral leishmaniasis almost exclusively afflicts the poorest of people, such is not
the case is not with all neglected diseases. Malaria affects the middle and upper
classes. So does diarrhea. Similarmente, a compound could be developed for the same
indication in two regions of the world. This so-called dual market approach has
the potential to earn revenue and have public health impact.
Por supuesto, we did not create iOWH to be yet another revenue-maximizing
drug company. Our non-profit model enables us to fulfill our mission to make
70
innovaciones / caer 2007
Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023
Seeking a Cure for Inequity in Access to Medicines
drugs that are not only safe and effective, but also affordable and accessible to all.
In order to do this important work far into the future, expanding our reach and
impacto, we must continue to seek innovative ways to grow and sustain the organ-
ización.
NEGLECTED NO MORE
The Institute for OneWorld Health is not the cure to global inequities of access to
medicines. If it is part of the solution, it will not be because of what we are able to
accomplish in isolation. Bastante, it will be because others innovate at least as aggres-
sively as we have sought to, mobilizing resources, forming partnerships, affecting
changes in policy, and creating new paradigms that work for the poor, en vez de
against them.
My own belief, sin embargo, is that new technologies, creative organizational
estructuras, and necessary re-alignments of incentives will be insufficient to bring
about such change unless all are combined with one other essential element: moral
outrage. When even a single life is wasted for want of a treatment that, si está disponible,
could be provided for less than the cost of a box of Band-Aids, we as a global com-
munity have failed.
To address this failure will require an effort distributed across the globe, de
village clinics to corporate boardrooms—and it will necessitate great humility and
compassion. It may begin with the work of organizations such as ours in building
awareness and creating new opportunities for action. But it ends only when neg-
lected diseases, and the people they afflict, are neglected no more. Insert updated
graphic
1 Naturaleza, Abril 13, 2006
innovaciones / caer 2007
71
Descargado de http://direct.mit.edu/itgg/article-pdf/2/4/59/704219/itgg.2007.2.4.59.pdf by guest on 08 Septiembre 2023