ARTÍCULO DE INVESTIGACIÓN
Perilesional Perfusion in Chronic Stroke-Induced
Aphasia and Its Response to Behavioral
Treatment Interventions
un acceso abierto
diario
Swathi Kiran2,6
, Brenda Rapp2,7
, Todd B. Parrish2,3
Matthew Walenski1,2
, Yufen Chen2,3
, Kaitlyn A. Litcofsky2,4
,
, and Cynthia K. Thompson2,4,8
, David Caplan2,5
1Department of Communication Sciences and Disorders, East Carolina University, Greenville, CAROLINA DEL NORTE
2Center for the Neurobiology of Language Recovery, Northwestern University, Evanston, IL
3Department of Radiology, Feinberg School of Medicine, Northwestern University, Evanston, IL
4Department of Communication Sciences and Disorders, School of Communication, Northwestern University, Evanston, IL
5Massachusetts General Hospital, Department of Neurology, Harvard Medical School, Bostón, MAMÁ
6Department of Speech, Idioma, and Hearing, College of Health & Rehabilitation, Boston University, Bostón, MAMÁ
7Department of Cognitive Science, Krieger School of Arts & Ciencias, Universidad Johns Hopkins, baltimore, Maryland
8Department of Neurology, Feinberg School of Medicine, Northwestern University, Evanston, IL
Palabras clave: aphasia, stroke, perfusion, resonancia magnética, treatment
ABSTRACTO
Stroke-induced alterations in cerebral blood flow (perfusion) may contribute to functional
language impairments in chronic aphasia, particularly in perilesional tissue. Abnormal
perfusion in this region may also serve as a biomarker for predicting functional improvements
with behavioral treatment interventions. Using pseudo-continuous arterial spin labeling in
magnetic resonance imaging (resonancia magnética), we examined perfusion in chronic aphasia, in perilesional
rings in the left hemisphere and their right hemisphere homologues. In the left hemisphere we
found a gradient pattern of decreasing perfusion closer to the lesion. The opposite pattern was
found in the right hemisphere, with significantly increased perfusion close to the lesion
homologue. Perfusion was also increased in the right hemisphere lesion homologue region
relative to the surrounding tissue. We next examined changes in perfusion in two groups: uno
group who underwent MRI scanning before and after three months of a behavioral treatment
intervention that led to significant language gains, and a second group who was scanned twice
at a three-month interval without a treatment intervention. For both groups, there was no
difference in perfusion over time in either the left or the right hemisphere. Además, within the
treatment group pre-treatment perfusion scores did not predict treatment response; neither did
pre-treatment perfusion predict post-treatment language performance. These results indicate
that perfusion is chronically abnormal in both hemispheres, but chronically abnormal
perfusion did not change in response to our behavioral treatment interventions, and did
not predict responsiveness to language treatment.
INTRODUCCIÓN
Alterations in vascular physiology are common sequela of acute stroke and persist into chronic
stages (Fridriksson et al., 2006; Hillis, 2007; Richardson et al., 2011). Evidence from multiple
sources suggests that restoration of cerebral blood flow (CBF; the rate at which blood perfuses
a neural region) is critically associated with functional recovery due to natural recovery and
Citación: Walenski, METRO., Chen, y.,
Litcofsky, k. A., Caplan, D., Kiran, S.,
Rapp, B., Parrish, t. B., & Thompson,
C. k. (2022). Perilesional perfusion in
chronic stroke-induced aphasia and its
response to behavioral treatment
intervenciones. Neurobiology of
Idioma, 3(2), 345–363. https://doi.org
/10.1162/nol_a_00068
DOI:
https://doi.org/10.1162/nol_a_00068
Recibió: 21 December 2020
Aceptado: 2 Febrero 2022
Conflicto de intereses: Los autores tienen
declaró que no hay intereses en competencia
existir.
Autor correspondiente:
Cynthia K. Thompson
ckthom@northwestern.edu
Editor de manejo:
Stephen M. wilson
Derechos de autor: © 2022
Instituto de Tecnología de Massachusetts
Publicado bajo Creative Commons
Atribución 4.0 Internacional
(CC POR 4.0) licencia
La prensa del MIT
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
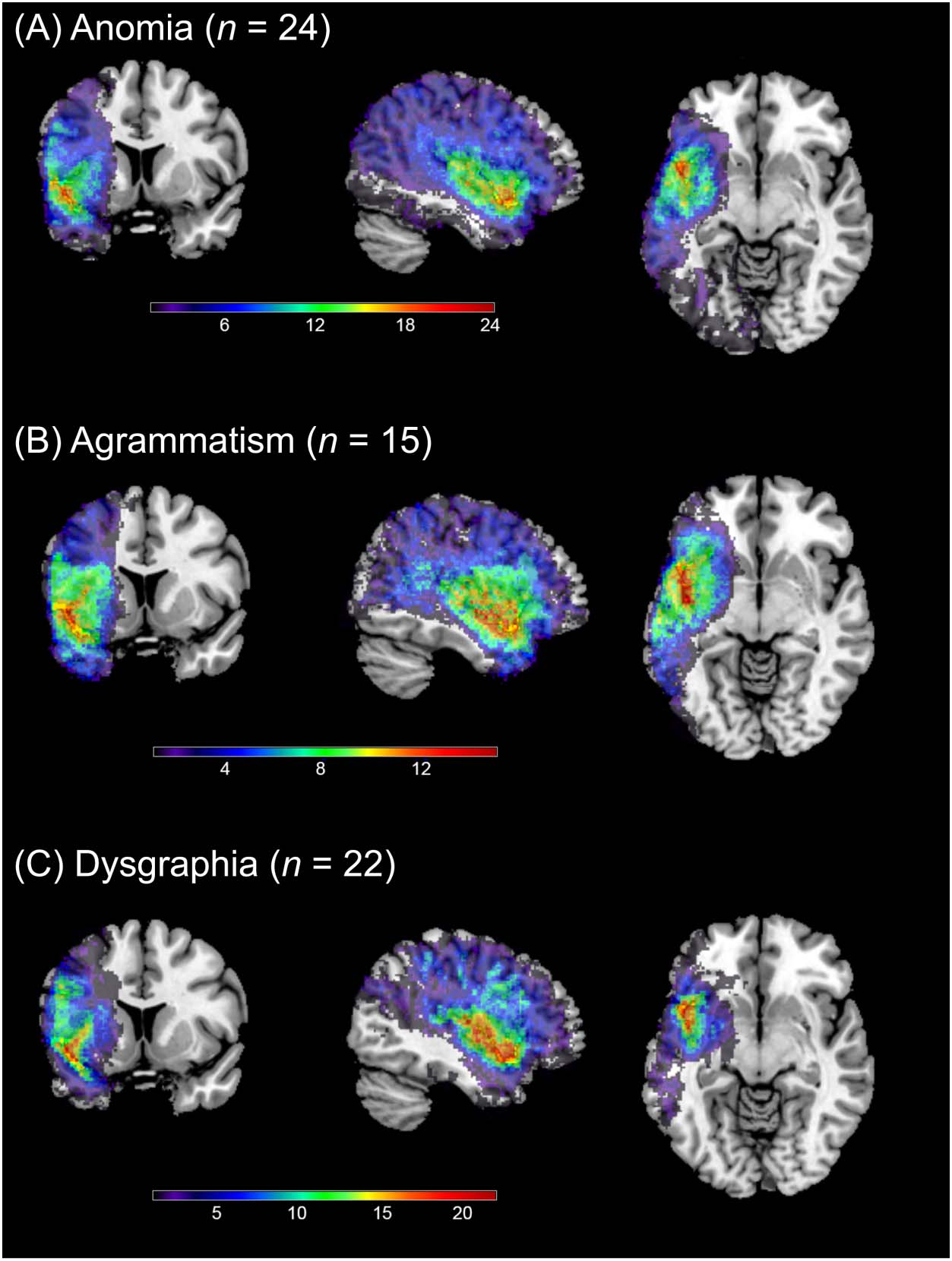
Perilesional perfusion in aphasia
Anomia:
The impaired ability to produce or
recognize the spoken or written
names of an object.
Neurobiology of Language
reperfusion of damaged regions, especially in the hyperacute stage (Hamilton et al., 2011; Saur
et al., 2006). Sin embargo, chronic reductions in CBF (hypoperfusion) in specific regions may
contribute to long-term language impairments in individuals with aphasia (Brumm et al.,
2010; Love et al., 2002; Richardson et al., 2011; Thompson et al., 2010, 2017).
One region that may be important for understanding chronic functional impairments, y
which may therefore also provide a fruitful avenue for recovery, is perilesional tissue. Cómo-
alguna vez, what constitutes a “perilesional” region has never been precisely defined (Thompson
et al., 2017), and some authors refer to perilesional regions strictly in terms of rings of tissue
surrounding the lesion. Here we focus on studies examining such perilesional rings in chronic
aphasia, where the extent of the rings identified as perilesional have varied across reports, de
6.88 (left/right, anterior/posterior) o 13.88 mm (inferior/superior) depending on direction
(Brumm et al., 2010), to 3–8 mm (Richardson et al., 2011), 3–15 mm (Fridriksson et al.,
2012), 0–6 mm (Thompson et al., 2017), 0–5 mm (Boukrina et al., 2019), and 0–3 mm (Abbott
et al., 2021).
Despite variable definitions of how far perilesional tissue extends, multiple results indicate
that perfusion in perilesional rings is abnormally low relative to regions of the ipsilesional
hemisphere that are further from the lesion (Boukrina et al., 2019; Fridriksson et al., 2012;
Thompson et al., 2017). Fridriksson and colleagues (2012) report a gradient pattern, con
significant reductions in perfusion across multiple successive 3 mm rings surrounding the
lesion—perfusion in a 3–6 mm ring was lower than in a 6–9 mm ring, which was in turn lower
than in a 9–12 mm ring, again in turn lower than in a 12–15 mm ring. Perfusion in perilesional
rings is also consistently found to be abnormally low relative to undamaged homologue
regions in the contralesional hemisphere (Brumm et al., 2010; Richardson et al., 2011;
Thompson et al., 2017), though only marginally so in one study (Boukrina et al., 2019).
En tono rimbombante, reperfusion of hypoperfused tissue has been shown to provide a notable avenue
for recovery of function, in animals and humans in the acute stage of language impairments
(Chollet et al., 1991; Hillis, 2005; Sotavento & van Donkelaar, 1995), and treatment interventions
for motor impairments in chronic stroke have led to improved perfusion in motor areas (Hara
et al., 2013; Könönen et al., 2005). In chronic aphasia as well, treatment with transcranial mag-
netic stimulation has led to improved language function and a leftward (es decir., ipsilesional) shift in
perfusion in specific language areas of interest (notably BA44, with right hemisphere stimula-
ción), measured with single photon-emission computed tomography (SPECT; Hara et al., 2015).
Sin embargo, we are aware of only one prior study in chronic aphasia that measured changes in
perfusion in perilesional rings over time. In this natural recovery study, no changes in perile-
sional perfusion between subacute (1–5 weeks) and chronic periods were found (Boukrina
et al., 2019). We are not aware of any prior studies of chronic aphasia that have found changes
in perfusion in perilesional rings in response to behavioral treatment interventions.
Prior studies that examined the relationship between pre-treatment perfusion in perile-
sional rings and recovery of function in chronic aphasia produced mixed results. Boukrina
et al. (2019) examined longitudinal recovery (without treatment) between subacute (en
5 weeks post-stroke) and chronic (greater than 3 months post) periods in 15 participants with
single-word reading deficits, and found that subacute perilesional perfusion levels in the left
hemisphere were not predictive of subsequent (chronic) word reading accuracy. Similarmente, a
study of 30 chronic-state patients with anomia (minimum 6 months post-stroke) reported that
pre-treatment cortical perfusion in perilesional cortex (3–15 mm from the lesion) was not
associated with changes in correct naming in response to treatment (Fridriksson et al.,
2012). Sin embargo, Boukrina et al. (2019) reported a negative correlation: Increased subacute
346
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
perfusion in right hemisphere (RH) homologous perilesional rings was associated with worse
chronic word reading accuracy.
Note that while perfusion in the unlesioned right hemisphere has been used as a “normal”
standard of comparison for left hemisphere (LH) perilesional rings, we are aware of only two
studies that report comparisons across RH homologue regions. In one study, no difference in
perfusion levels was seen between an RH homologue ring (3–8 mm) and the distal remainder
of the right hemisphere (Richardson et al., 2011). In another, no difference in RH perfusion
levels was seen between 0–6 mm, 6–12 mm, and 12–18 mm homologue rings (Thompson
et al., 2017).
Here we focus on three main questions. In experiment 1, we examine the status of perfusion
in chronic aphasia in LH perilesional rings and their RH counterparts. In experiment 2, nosotros
examine the extent to which perilesional perfusion levels in these rings change in response
to behavioral language interventions. In experiment 2 we also examine whether the pre-
treatment perilesional perfusion levels in the left hemisphere, or their RH homologues,
predict a treatment-modulated improvement in language. Based on prior results, we expect
LH perilesional perfusion to be abnormally low, relative both to RH homologue regions and
to more distal LH tissue. Además, perfusion levels in these rings may not change in response
to our behavioral treatment interventions. Finalmente, previous results suggest that perilesional
hypoperfusion should not predict treatment efficacy, whereas there may be a maladaptive
relationship for RH homologue rings, such that increased perfusion predicts a worse treat-
ment outcome.
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
.
/
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Agrammatism:
Speech production that is
characterized by short, syntactically
impoverished utterances with
frequent pauses and the omission of
function words, along with an
impaired ability to produce and
comprehend syntactically complex
oraciones.
Dysgraphia:
The impaired ability to produce
written language.
EXPERIMENT 1
Método
Participantes
probamos 71 participants with aphasia subsequent to a single LH ischemic stroke (Table 1A).
Participants with different aphasias were recruited from three research sites, Northwestern
Universidad (agrammatism; norte = 17), Boston University (anomia; norte = 30), and Johns Hopkins
Universidad (dysgraphia; norte = 24), as part of a large-scale Clinical Research Center funded by
the NIDCD (National Institute on Deafness and Other Communication Disorders). El estudio
was approved by the Institutional Review Boards of all three universities, and all participants
Mesa 1.
Participant information (mean and standard deviation)
Age (años)
Sex
Educación (años)
Months post-stroke
WAB-AQ
(A)
Aphasia (norte = 71)
58.3 (10.3)
48 METRO / 23 F
15.8 (2.1)
62.1 (50.4)
68.1 (22.2)
(B)
Tratamiento (norte = 45)
59.3 (10.0)
30 METRO / 15 F
Control (norte = 16)
56.8 (12.3)
12 METRO / 4 F
15.8 (2.2)
15.8 (2.0)
58.5 (43.8)
58.4 (50.9)
65.0 (24.1)
74.1 (18.0)
Nota. WAB-AQ = Western Aphasia Battery—Aphasia Quotient (Kertesz, 2006).
Neurobiology of Language
347
Perilesional perfusion in aphasia
provided informed consent. Note that pre-treatment perfusion data from 35 of these partici-
pants was previously reported (Thompson et al., 2017). Note that an additional 10 Participantes
were tested, but their data were excluded due to artifacts (see Data Processing, abajo). El
demographic details here include only the 71 participants in the final data set.
Participants were all in the chronic stage of aphasia, and were at least eight months post-
stroke-onset (m = 62.1 meses, DE = 50.4, range: 8–209 months). All participants were (pre-
morbid) right-handed native English speakers (48 METRO, 23 F; edad: range = 39–79 yr, m = 58.8,
DE = 10.3; education: m = 15.8 yr, DE = 2.1); 6 of the participants with anomia were bilin-
gual, though English was their dominant language. Participants passed vision and hearing
screenings (pure-tone audiometric screening at 40 dB, 1000 Hz), and had no other diagnosed
brain disorders and no history of drug or alcohol abuse.
The characterization, diagnosis, and overall severity of aphasia was based on administration
of the Western Aphasia Battery—Revised ( WAB-R; Kertesz, 2006); WAB-AQ (Aphasia Quotient)
scores ranged from 11.7 a 97.5 (m = 68.1, DE = 22.2); and a battery of standard language tests,
which included measures of spoken and written comprehension and production of words and
oraciones. Note that while the WAB-AQ scores for some participants (norte = 5, 1 with anomia and
4 with dysgraphia) were above the standard cutoff for a diagnosis of aphasia (93.8), our partic-
ipants with high WAB-AQ scores were nevertheless characterized as aphasic based on their
scores on our standard language battery.
Our standard language battery consisted of language tasks chosen to identify individuals
with agrammatism, anomia, or dysgraphia. Single word production and comprehension were
tested using 26 items from the Confrontation Naming and Auditory Comprehension subtests of
the Northwestern Naming Battery (NNB; Thompson & Weintraub, 2014) (10 low frequency
nouns from the “Other” category on the NNB and 16 verbos). Word production performance
osciló entre 0% a 100% (m = 58%, DE = 31%); word comprehension performance ranged
de 24% a 97% (m = 75%, DE = 17%). We used the Psycholinguistic Assessments of
Language Processing in Aphasia (PALPA; Kay et al., 1996) to evaluate spelling-to-dictation
of words with high and low frequency (subtest 40) (m = 36%, DE = 31%, range: 0% a
98%). Finalmente, we used the Sentence Production Priming Test (SPPT) and the Sentence
Comprehension Test (SCT) from the Northwestern Assessment of Verbs and Sentences (NAVS;
Thompson, 2011) to evaluate production and comprehension of sentences of different syntac-
tic complexity. Each test includes 30 items to test canonical and noncanonical structures.
Performance on sentence comprehension for noncanonical sentences ranged from 27% a
100% (m = 64%, DE = 20%), and for canonical sentences performance ranged from 33%
a 100% (m = 79%, DE = 20%). For sentence production, performance for noncanonical
sentences ranged from 0% a 100% (m = 33%, DE = 34%), and for canonical sentences
performance ranged from 0% a 100% (m = 49%, DE = 37%).
Data Acquisition
Images were collected on four different 3.0T systems: a Siemens TIM Trio with a 32-channel
head coil (Northwestern University), a Siemens Prisma with a 64-channel head/neck coil
(Northwestern University), a Skyra with 20-channel head/neck coil (Boston University), y
a Philips Intera with a 32-channel head coil ( Universidad Johns Hopkins). Prior to the study,
a study team member acted as a travel phantom to all sites, where trial data were collected
and inspected to ensure identical imaging parameters.
Resting CBF maps were collected using a pseudo-continuous arterial spin labeling (pCASL)
secuencia (Dai et al., 2008) with two-dimensional gradient echo-planar imaging (EPI) readout:
Neurobiology of Language
348
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
field of view (FOV) = 220 mm, in-plane resolution = 3.4 × 3.4 mm2, 25 slices, thickness = 4 mm
con 1 mm gap, TE/TR = 11 EM / 4,500 EM. The labeling plane was situated 90 mm below the
center of the imaging volume, and labeling pulses were applied for 1.5 s. The post labeling
delay was set to 1,900 ms to balance between potential slow flow and adequate signal-to-noise
ratio (Alsop et al., 2015). Sixty pairs of interleaved control and tag images were acquired for
signal averaging. In addition to the ASL scan, high resolution T1-weighted anatomical images
were acquired using an MPRAGE (magnetization-prepared rapid acquisition with gradient
echo) secuencia (Mugler & Brookeman, 1990): FOV = 256 mm, TE/ TR/ TI = 2.91 EM /
2300 EM / 900 EM, 176 sagittal slices, resolution 1 mm3.
Data Processing
Perfusion-weighted images from the pCASL scan were processed at a single site by an expert
in perfusion imaging, using a pipeline incorporating commands from Statistical Parametric
Cartografía (SPM8; Wellcome Trust Centre for Neuroimaging, Londres, Reino Unido), and code developed
in-house with Matlab R2013a (Matemáticas, Natwick, MAMÁ), and implemented on the North-
western University Neuroimaging Data Archive (NUNDA; Alpert et al., 2016). Brevemente, el
raw EPI images were aligned to the first image of the time series to extract six motion-related
measures for the time series. The motion parameters and signal from voxels containing 99%
cerebrospinal fluid were regressed out of the time series to remove motion-related and phys-
iological fluctuations in the signal (Wang, 2012). Perfusion weighted time series were gener-
ated using pairwise subtraction, and outliers were removed based on the following criteria
(Wang y cols., 2008): (a) translation greater than 0.8 mm; (b) rotation greater than 0.8°;
y (C) global signal or noise greater than 2 times the standard deviation. Based on these
criteria, an average of 7 pairs of images was discarded from each ASL scan for participants with
agrammatism or anomia, y 8 pairs of images for participants with dysgraphia.
After processing, participant data were visually inspected and were assessed based on
summary statistics including the number of images discarded due to motion, raw signal-to-
noise ratio of mean perfusion weighted images, and global CBF values. Data sets with global
CBF values less than 20 ml / 100 gramo / min or discarded images more than 2 times the standard
desviación + mean number of discard images were labeled as unusable and excluded from
final analysis. This resulted in the exclusion of data from 10 Participantes (2 with agrammatism,
5 with anomia, y 3 with dysgraphia).
The final perfusion weighted time series were then converted into quantitative flow (F )
maps in units of ml / 100 gramo / min using the following equation:
f ¼
λ ∙ ΔM
2αM0 ∙ T1b ∙ e−PLD=T1b − e− τþPLD
d
d
;
Þ=T1b
Þ
where λ is the blood/tissue partition coefficient = 0.9 ml / gramo (Herscovitch & Raichle, 1985), ΔM
is the perfusion-weighted signal, α is the inversion efficiency = 0.85 (Dai et al., 2008), M0 is the
equilibrium signal of tissue, PLD is the post-labeling delay, τ the labeling duration, and T1b is
the T1 of blood = 1,664 EM (Lu et al., 2004).
Due to the low resolution of CBF maps, partial volume effects are prominent and need to be
corrected before any further analysis. This was implemented as another NUNDA pipeline
based on the following equation derived from positron emission tomography CBF studies
(Du et al., 2006):
fGM ¼ funcorr − PWM ∙ fWM
PGM
;
Neurobiology of Language
349
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
where funcorr is the uncorrected flow value, PGM and PWM denote gray and white matter prob-
ability in the voxel, extracted from tissue segmentation of the high-resolution anatomical
imagen, and fGM and fWM are the corresponding tissue-specific flow values. fWM was extracted
from voxels containing 99% white matter. To minimize artifactually high CBF due to division
by small numbers, the above calculation was limited to voxels containing at least 30% gray
asunto (Chen et al., 2011; Hu et al., 2010). The partial volume corrected CBF maps were then
spatially normalized to MNI (Instituto Neurológico de Montreal) space using the transformation
matrix calculated from the high-resolution anatomical image after co-registering the ASL data
to the native T1 scan. We removed any voxels that were left with negative values after these
processing steps, as these could only reflect noise in the data.
Finalmente, as CBF is a physiological parameter that fluctuates with many factors such as vaso-
active agents in food, beverages, and drugs, and varies widely between subjects (Clement
et al., 2018), we normalized all CBF values to the mean CBF of each individual’s right occip-
ital lobe region, in order to reduce between-subject variation. We based the definition of the
right occipital lobe cortical region on the Harvard Oxford atlas (https://neurovault.org
/collections/262/), processed as above for the perilesional regions of interest (ROI). Nota
that this choice assumes that CBF in this region is not compromised by an LH stroke resulting
in aphasia.
Lesion Volume
Lesion volume was derived from lesion maps, developed by manual drawings measured using
MRIcron software (https://www.nitrc.org/projects/mricron; Rorden & Brett, 2000), rastreado (y
confirmed) by lab members with extensive experience with MRI and lesion tracing. To delin-
eate the borders of necrotic tissue in each patient, we first determined intensity measures for
white and grey matter ( WM and GM, respectivamente) in the contralateral (bien) hemisphere for
each axial slice. The minimum right hemisphere WM intensity was determined. Left hemi-
sphere lesioned tissue, on each slice, was drawn using the pen tool of MRIcron. Then the min-
imum WM intensity from the right hemisphere was applied to the outlined area in the left
hemisphere using the intensity filter function, to avoid including voxels in the lesion mask that
were potentially white matter. Additional manual correction was applied using lesion outlines
in multiple corresponding coronal and sagittal views. Total lesion volume was calculated by
summing the number of lesioned voxels in the left hemisphere for each participant. En nuestro
analyses the size of each voxel was 1 mm3 and therefore lesion volume is reported in mm3.
Regions of Interest
Regions of interest and their RH homologues were created by first identifying the ROI of the
lesion in the left hemisphere (taking the homologous RH region), and then dilating the lesion
a 6 mm, a 12 mm, y para 18 mm beyond its boundaries and subtracting the original lesion
and smaller perilesional volumes for each ROI (Cifra 1). Thus we created three perilesional
rings that were 0–6 mm, 6–12 mm, and 12–18 mm from the lesion, which were confined to
the LH grey matter. The size of the rings was chosen to be consistent with our previous work
(Thompson et al., 2017). Mean CBF within each ROI was only computed from voxels with
30% or more gray matter, as division by a small number (PGM, see partial volume correction
equation above) yields unrealistically high CBF values. In addition to correcting for partial
volumen, the ROIs also accounted for the lesion mask (voxels where the lesion value is set
a 1 were excluded from the analysis) and the FOV of the perfusion scan (an FOV mask
was created to exclude all voxels not covered by the perfusion scan).
Neurobiology of Language
350
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
.
/
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
Cifra 1. An axial slice from a representative participant showing the lesion and perilesional ROI
masks for (A) the left hemisphere (LH) y (B) the right hemisphere (RH) homologue regions. El
lesion and its homologue are in white; 0–6 mm ring in blue, 6–12 mm in green, and 12–18 mm
in pink. The rings are outlined in their respective colors to show the boundary of each ring; el
filled-in portions of each ring reflect gray matter within each ring (only gray matter voxels within
each ring were used to calculate perfusion). Note that the rings reflect distance from the lesion in
three dimensions—that is, portions of a ring that are visible in this slice may reflect lesioned tissue
that is above or below the plane of this image slice, making the rings appear larger than expected for
the lesion visible in the image.
Análisis de los datos
Data from the full pre-treatment cohort (norte = 71) were analyzed with mixed effects linear
modelos de regresión (proc glimmix; SAS 9.4 for Windows; SAS Institute, 2012) with a random
effect of participant on the intercept and fixed effects of Hemisphere (LH, RH), Ring (0–6 mm,
6–12 mm, 12–18 mm), and their interaction. We included additional random effects by par-
ticipant if their inclusion improved model fit, based on the Bayesian information criteria (BIC).
Reductions to BIC greater than 10 (as a chi-square with 1 degree of freedom) were considered
an improved fit. Based on these criteria, Hemisphere was included as a random effect (BIC
changed from −597.17 in the intercept only model to −642.58 when Hemisphere was added);
but Ring (BIC = −636.05) and the Hemisphere by Ring interaction (BIC = −609.82) no lo hizo
improve model fit, and so were included as fixed effects only.
We also included several additional predictor variables as fixed effects, to account for
potential sources of variability in the data. We included participant age and sex, y dado
that our participants were tested on 4 different scanners, we included scanner as well. Nosotros también
incluido (square root transformed) lesion volume. The transformation was applied to remove
the positive skew in the distribution of lesion volumes.
Follow-up contrasts were assessed for ring differences within each hemisphere and for the
same rings across hemispheres. For these contrasts we report the regression coefficient (B) con
its standard error, the t test of the difference, y el 95% confidence interval. We applied the
Benjamini-Hochberg false discovery rate (FDR) correction (Benjamini & Hochberg, 1995) para
multiple comparisons (with an FDR of 0.05) to these contrasts, and report q values (two-tailed)
instead of p values.
Neurobiology of Language
351
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
We assessed the comparison of perfusion in the RH lesion homologue against the 0–6 mm
RH ring with an additional regression model, with random effects of participant on the inter-
cept, and a fixed effect of Region (lesion homologue vs. 0–6 mm ring). Adding Region as a
random effect did not improve model fit (BIC for intercept only model = −132.64; BIC with
region added as random effect = −126.25), so it was included in the model as a fixed effect
solo. Square root transformed lesion volume, scanner, edad, and sex were included as addi-
tional independent predictor variables.
All models were fit with an unstructured covariance matrix. We report F and p values from
Type III tests of the main effects and interactions of these factors. Degrees of freedom were
computed using the Satterthwaite approximation (note that these degrees of freedom are cal-
culated based on the variance, and are not the same as in ANOVA). Significance of all com-
parisons was assessed with α = 0.05. All of the reported p values are two-tailed.
Resultados
We examined CBF in perilesional tissue in all participants (norte = 71) prior to treatment (Cifra 2).
There were significant main effects of Hemisphere (lower perfusion in LH than RH; F(1, 70) =
177.16, pag < 0.0001), and Ring (F(2, 70) = 18.5, p < 0.0001), but also a significant Hemisphere ×
Ring interaction (F(2, 140) = 148.55, p < 0.0001). The effects of lesion volume (F(1, 64) = 0.04,
p = 0.83), scanner (F(3, 64) = 1.0, p = 0.40), age (F(1, 64) = 0.2, p = 0.66), and sex (F(1, 64) =
0.00, p = 0.95) were not significant.
Follow-up contrasts confirmed that within the left hemisphere, perfusion was significantly
lower in the 0–6 mm perilesional ring relative to the 6–12 mm (B = −0.14, SE = 0.01, t(170) =
13.1, 95% CI [−0.16, −0.12], q = 0.0001); perfusion in the 6–12 mm ring was also significantly
lower than in the 12–18 mm ring (B = −0.04, SE = 0.01, t(176) = 4.28, 95% CI [−0.06, −0.02],
q = 0.0001). However, the opposite pattern was found within the right hemisphere, with
significantly greater perfusion in the 0–6 mm ring relative to the 6–12 mm ring (B = 0.05,
SE = 0.01, t(170) = 4.51, 95% CI [0.03, 0.07], q = 0.0001), but the 6–12 mm ring did not differ
from the 12–18 mm ring (B = 0.005, SE = 0.01, t(176) = 0.53, 95% CI [−0.01, 0.03], q = 0.6).
Across hemispheres, contrasts revealed that perfusion in the left hemisphere was signif-
icantly lower than perfusion in the right hemisphere, in the 0–6 mm ring (B = −0.31, SE =
0.016, t(121) = 20.15, 95% CI [−0.34, −0.28], q = 0.0001), as well as the 6–12 mm ring
(B = −0.13, SE = 0.015, t(121) = 8.29, 95% CI [−0.16, −0.10], q = 0.0001), and the 12–18 mm
ring (B = −0.09, SE = 0.015, t(121) = 5.83, 95% CI [−0.12, −0.06], q = 0.0001).
Perfusion in the RH lesion homologue region was significantly elevated beyond the elevated
perfusion found in the 0–6 mm RH perilesional ring (homologue M = 1.04, SE = 0.02; 0–6 mm
ring M = 1.00, SE = 0.02; F(1, 70) = 17.25, p = < 0.0001; Figure 2D). Effects of lesion volume,
scanner, age, and sex were all nonsignificant (all ps > 0.39).
Discusión
We examined blood flow in a cohort of individuals with chronic aphasia prior to treatment, en
three LH perilesional rings and their RH homologues, as well as in the RH lesion homologue
región.
In the absence of treatment, the results for all three perilesional rings revealed that perfusion
in the damaged left hemisphere was lower than in the undamaged right hemisphere, consistent
with previous findings (Boukrina et al., 2019; Brumm et al., 2010; Richardson et al., 2011;
Thompson et al., 2017). Within the left hemisphere as well, tissue closer to the lesion was
Neurobiology of Language
352
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
.
/
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
Cifra 2. Pre-treatment perilesional perfusion in left hemisphere (LH) perilesional rings (A) and their right hemisphere (RH) homologues (B).
Ring color is scaled to perfusion values, with lighter grays for lower perfusion values and darker grays for higher perfusion values. A table (C)
shows normalized perfusion values and standard error for each perilesional ring and its RH homologue, with scaled colors corresponding to
the rings in (A) y (B). Values with * and in bold indicate that the smaller ring is significantly different from the next larger ring within the same
hemisferio (q < 0.05). For all three rings, perfusion was significantly lower in the LH than the RH (q < 0.05; see text). An additional analysis (D)
revealed significantly elevated perfusion for lesion-homologous tissue in the right hemisphere relative to the RH 0–6 mm ring (p < 0.0001). All
perfusion values are normalized to a right occipital cortical ROI.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
reduced in perfusion relative to more distant areas—for the 0–6 mm ring compared to the
6–12 mm ring, and for 6–12 mm vs. 12–18 mm. This is again consistent with prior findings
(Abbott et al., 2021; Boukrina et al., 2019; Fridriksson et al., 2012; Thompson et al., 2017), but
is most consistent with one prior study that reports a similar gradient across successive 3 mm
rings (Fridriksson et al., 2012).
The finding that there is a similar gradient pattern across different size rings suggests that the
gradient may be continuous—that is, perfusion may gradually increase the further one gets
from the lesion. Dividing such a smoothly changing variable into discrete chunks would yield
effects consistent with those we and others have observed. It is not clear how steep such a
gradient may be (i.e., how quickly it changes with distance from the lesion, if indeed it
Neurobiology of Language
353
Perilesional perfusion in aphasia
changes linearly), or how uniform it may be (i.e., the gradient may be steeper or shallower in
different directions).
In the right (contralesional) hemisphere we observed that perfusion in the lesion homologue
region was elevated relative to the tissue surrounding it (0–6 mm homologue ring). Cerebral
blood flow was also elevated in the innermost perilesional homologue ring (0–6 mm) relative
to the next more distal ring (6–12 mm). There was no difference beyond that (6–12 mm vs.
12–18 mm). Thus the right hemisphere seems to capture an inverse echo of the lesion, in a region
of locally increased perfusion, extending to the immediate perilesional space. This effect was not
seen in prior studies, which report no difference between RH perilesional homologue regions
(Richardson et al., 2011; Thompson et al., 2017). This may be because the effect was relatively
small (0–6 mm vs. 6–12 mm, Hedge’s gav = 0.30), and prior studies had fewer participants.
These prior studies also did not examine perfusion in the RH lesion homologue region.
These results are unlikely to reflect individual variability due to factors known (or suspected)
to modify perfusion measurements. These perfusion modifiers, related to physiology (e.g., age,
sex, blood pressure), blood components (e.g., gasses such as O2 and CO2, cholesterol), mental
state (e.g., mood, stress, anxiety), and drugs (e.g., caffeine and other legal or illegal substances)
can introduce large sources of inter-individual variability (Clement et al., 2018). We took several
steps to mitigate the impact of these factors. First, we asked participants to maintain their normal
caffeine levels prior to testing, to avoid issues due to unusual drowsiness, alertness, or other
effects on mood or cognition. Most important, however, because it was not possible for us to
obtain objective measures for most of these factors, we normalized each participant’s data to
a region of their brain that was most likely to have been undisturbed by their lesion. We also
included age and sex in the analyses, to further reduce the impact of individual differences
due to these factors, though we note that these factors were not significant in our analyses.
The findings also do not appear to reflect differences in the scanners that were used to acquire
the data, or differences in lesion volume across participants, as neither factor was a significant
predictor of perfusion values in any analysis. Therefore, we argue that our results are unlikely to
reflect random variation across participants due to these (or other) perfusion modifiers.
It has been previously suggested that chronically abnormal CBF in aphasia may reflect an
autoregulatory change to altered LH vasculature, particularly with respect to regions that
appear to be hyperperfused (Thompson et al., 2017). That is, blood typically directed automat-
ically to the LH middle cerebral artery could be shifted elsewhere, for example, to the right
middle cerebral artery, leading to increased perfusion in regions supplied by that artery. While
autoregulatory disturbances in ischemic stroke are typically of short duration, such disturbances
have been observed in chronic stroke (Kunz & Iadecola, 2008). Consistent with this argument,
contralesional hyperperfusion has been observed in a small number of prior studies in cortical
and subcortical regions (Miao et al., 2018; Thompson et al., 2017; Wang et al., 2019). How-
ever, the current findings suggest that there may be a more specific pattern that persists in
chronic aphasia, with a regional increase in perfusion in the undamaged hemisphere that
mirrors the lesion homologue and proximate perilesional tissue.
EXPERIMENT 2
Method
Participants
The same participants from experiment 1 were randomly assigned either to a treatment group
or to a control group that did not receive treatment. Randomization of participants to the
Neurobiology of Language
354
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
n
o
_
a
_
0
0
0
6
8
p
d
/
.
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Perilesional perfusion in aphasia
treatment or control group occurred independently at each recruitment site, and was carried
out by a staff member other than the person who performed the language assessment. The
principal investigator(s) at each recruitment site were not blinded to allocation of participants.
Individuals in the treatment (n = 45: 10 with agrammatism, 19 with anomia, 16 with dysgra-
phia) and control (n = 16: 5 from Northwestern University, 5 from Boston University, 6 from
Johns Hopkins University) groups (Table 1B) were scanned at baseline (pre-treatment) and
again 12 weeks later (after the end of treatment for the treatment group). Note that 8 partici-
pants did not complete their second scan, and so are not included here. Data from an addi-
tional 2 participants were excluded after data processing, due to excessive artifacts in the
data, based on the same criteria described above. The treatment and control groups did not
differ with respect to age (2-sample unequal variance t test: t(22) = 0.74, p = 0.47), pro-
portion of male and female participants (χ2 = 0.38, p = 0.54), years of education (t(29) =
0.07, p = 0.94), or months post-stroke onset (t(23) = 0.01, p = 0.99). The participants in
the treatment group had lower WAB-AQ scores than the participants in the control group
(treatment Mean: 65.0, control Mean: 74.1), but this difference was not significant (t(35) =
1.58, p = 0.12).
Data Acquisition
Data in each scan was acquired as described for experiment 1. Pre-treatment and post-
treatment scans were taken approximately 3 months apart. Participants were asked to maintain
their normal caffeine levels for each scan, which were conducted at the same time of day
across sessions for each participant.
Data Processing, Lesion Volume, ROI Calculation
These were all the same as for experiment 1.
Treatment Interventions
Different treatment interventions were given to participants at each of the three sites, corre-
sponding to their aphasia profile. Treatment at each site was administered in 90-minute sessions
twice per week for 12 weeks. At all sites, treatment was provided by trained research assistants
and monitored for fidelity, with an independent observer scoring half of the treatment sessions
for adherence to the treatment protocol. All sites also monitored treatment progress through
weekly probe tasks that assessed trained and untrained items. Different tasks were used at each
site to assess pre-treatment and post-treatment accuracy on the trained items. These tasks were
sentence production and comprehension (agrammatism), spelling-to-dictation (dysgraphia), or
picture naming (anomia). Because different treatments and assessment tasks were used at each
site, we computed treatment efficacy for each participant in terms of the change in their per-
centage correct scores from pre-treatment to post-treatment. Details of the specific treatment
and treatment schedule for participants at each site follow. Additional details are provided else-
where for agrammatism (Barbieri et al., 2019), anomia (Gilmore et al., 2020; Johnson et al.,
2019), and dysgraphia (Shea et al., 2020; Wiley & Rapp, 2019).
Participants with agrammatism were given Treatment of Underlying Forms (Barbieri et al.,
2019; Thompson & Shapiro, 2005), a treatment approach that uses a series of metalinguistic
steps focused on verbs, verb argument structure, and thematic-syntactic mapping in active and
passive sentences to improve sentence comprehension and production. Participants were
trained on 10 different semantically reversible passive sentences (e.g., The boy was shaved
by the man in the barbershop). Treatment efficacy was assessed with computer-based sentence
Neurobiology of Language
355
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
n
o
_
a
_
0
0
0
6
8
p
d
.
/
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Perilesional perfusion in aphasia
production priming (production) and sentence-picture matching (comprehension) tasks. The
average of the scores from the two tasks was used to quantify treatment efficacy.
Participants with dysgraphia were given treatment for spelling deficits using an individually
tailored set of words for each participant (Shea et al., 2020; Wiley & Rapp, 2019). For each
individual we selected forty training words such that baseline letter accuracy on each word
was between 25% and 85%. The treatment consisted of a spell-study-spell technique. Treat-
ment efficacy was assessed with a spelling-to-dictation task.
Participants with anomia were given a treatment for anomia using typicality-based semantic
features analysis, in which either typical (e.g., pigeon) or atypical (e.g., penguin) exemplars of
a certain semantic category (e.g., birds) were trained (Gilmore et al., 2020; Johnson et al.,
2019). Treatment efficacy was assessed with a confrontation naming test consisting of 180
items (in random order) from five semantic categories (i.e., birds, vegetables, fruit, clothing,
and furniture) including 36 exemplars of each category, and further divided into half-
categories by typicality (i.e., 18 typical; 18 atypical).
Data Analysis
We assessed changes in perfusion over time in treated and untreated groups with the same
approach as in experiment 1, using mixed effects linear regression models (SAS 9.4, proc
glimmix) with a random effect of participant on the intercept and fixed effects of Hemisphere
(LH, RH), Ring (0–6 mm, 6–12 mm, 12–18 mm), Group (treatment, control), Time (pre-treatment,
post-treatment), and their interactions.
We included additional random effects by participant based on whether their inclusion
improved model fit, based on the BIC. Reductions to BIC greater than 10 (as a chi-square with
1 degree of freedom) were considered an improved fit. Based on these criteria, Hemisphere was
included as a random effect (BIC changed from −842.61 in the intercept only model to −861.57
when Hemisphere was added); but Ring (BIC = −837.81) did not and so was included as a fixed
effect only. Time also improved model fit (BIC = −1,161.48) and so was included as a random
effect. Interactions were not considered for inclusion as random effects, given that they did not
improve model fit in experiment 1, and that there was a much larger set of interactions here. As
in experiment 1, (square root transformed) lesion volume, scanner, age, and sex were included
as additional independent predictor variables.
Significance of the change in behavioral treatment scores (post- minus pre- difference scores)
was assessed with a t test of this difference against 0. Finally, we used regression models to examine
whether pre-treatment perfusion values in any of our 3 left hemisphere or 3 right hemisphere-
homologue perilesional rings predicted either changes in behavioral treatment scores or
post-treatment scores (in separate models), adjusting in all cases for the (square root trans-
formed) lesion volume, scanner, age, and sex, and correcting for multiple comparisons using
the Benjamini-Hochberg FDR correction (Benjamini & Hochberg, 1995), with an FDR of 0.05.
Results
We examined changes in perfusion in the participants who were scanned at both time points,
comprising a treatment group (n = 45) and an untreated control group with aphasia (n = 16)
(Table 2). Consistent with the results from the full group (above), there were significant main
effects of Hemisphere (left lower than right: F(1, 59) = 136.14, p < 0.0001), Ring (0–6 mm vs.
6–12 mm vs. 12–18 mm: (F(2, 531) = 51.29, p = < 0.0001), and a significant Hemisphere by
Ring interaction (rings closer to the lesion are increasingly hypoperfused in the left
Neurobiology of Language
356
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
n
o
_
a
_
0
0
0
6
8
p
d
/
.
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Perilesional perfusion in aphasia
Table 2. Mean normalized perfusion (and standard error) in left hemisphere perilesional rings and their right hemisphere homologues for the
treatment and no-treatment groups at the two time points
Group
Treatment (n = 45)
Time
Baseline (pre)
0–6 mm
0.69 (0.03)
Left hemisphere
6–12 mm
0.82 (0.03)
12–18 mm
0.86 (0.03)
0–6 mm
1.01 (0.03)
Right hemisphere
6–12 mm
0.94 (0.02)
12–18 mm
0.95 (0.02)
3-months (post)
0.71 (0.02)
0.85 (0.02)
0.90 (0.02)
1.02 (0.02)
0.96 (0.02)
0.96 (0.02)
change
0.02ns
0.03ns
0.04ns
0.01ns
0.02ns
0.01ns
No-treatment (n = 16)
Baseline
0.68 (0.03)
0.82 (0.03)
0.86 (0.03)
0.96 (0.04)
0.93 (0.03)
0.94 (0.02)
3-months
0.70 (0.04)
0.83 (0.03)
0.86 (0.02)
1.00 (0.05)
0.96 (0.03)
0.95 (0.02)
change
0.02ns
0.01ns
0.00ns
0.04ns
0.03ns
0.01ns
Note. Perfusion change scores (3-months – baseline) were all non-significant. ns = non-significant.
hemisphere, 0–6 mm hyperperfused in the right: F(2, 531) = 135.42, p < 0.0001). The main
effect of Time was not significant (F(1, 59) = 0.57, p = 0.46). The effects of lesion volume (F(1,
53) = 1.31, p = 0.26), scanner (F(3, 57) = 2.05, p = 0.12), age (F(1, 53) = 0.01, p = 0.94) and
sex (F(1, 53) = 0.51, p = 0.48) were all nonsignificant.
While the overall pattern was therefore consistent with the results of experiment 1, there
were no significant main effects or interactions with Group (treatment vs. control): Group
(F(1, 53) = 0.26, p = 0.61), Group × Time (F(1, 59) = 0.06, p = 0.81), Group × Hemisphere
(F(1, 59) = 0.02, p = 0.90), Group × Hemisphere × Time (F(1, 531) = 2.7, p = 0.10), Group ×
Ring (F(2, 531) = 1.26, p = 0.28), Group × Time × Ring (F(2, 531) = 0.24, p = 0.78), Group ×
Hemisphere × Ring (F(2, 531) = 0.97, p = 0.38), and Group × Hemisphere × Time × Ring
(F(2, 531) = 0.14, p = 0.87). Also not significant were interactions of Time × Ring (F(2, 531) =
0.22, p = 0.80) and Hemisphere × Time × Ring (F(2, 531) = 0.14, p = 0.87). In addition,
follow-up contrasts to examine changes in perfusion over time revealed no significant effect
of Time in any perilesional ring in either hemisphere, for both the treatment and the control
group (all qs > 0.96).
Despite the finding of no evidence of a change in perilesional perfusion over time in
either the treatment or the control group, the treatment group did show a significant post-
treatment gain in language performance: post- minus pre- difference score against 0: m =
0.28, DE = 0.17; t0(44) = 11.1, pag < 0.0001; Hedge’s gav effect size: 0.95, a large effect
(Lakens, 2013). There was no change in performance for the control group (M = 0.02,
SD = 0.06; t0(15) = 1.03, p = 0.32; Hedge’s gav effect size: 0.07; only a small, nonsignificant
effect). However, there was no relationship between their treatment gain (post-treatment –
pre-treatment difference scores) and their pre-treatment perfusion, in the left hemisphere
0–6 mm perilesional region (B = 0.01, t(37) = 0.08, q = 0.95) or the 6–12 mm (B =
0.12, t(37) = 0.8, q = 0.93) or 12–18 mm rings (B = 0.11, t(37) = 0.75, q = 0.93), adjusted
for (square root transformed) lesion volume, scanner, age, and sex. The same analyses in the
right hemisphere were not significant in the 0–6 mm homologue ring (B = −0.03, t(37) =
0.24, q = 0.95), the 6–12 mm ring (B = −0.04, t(37) = 0.21, q = 0.95), and the 12–18 mm
ring (B = 0.01, t(37) = 0.06, q = 0.95). Likewise, pre-treatment perfusion did not predict
post-treatment test scores in any perilesional ring in the LH or in their RH homologues (all
qs > 0.92).
Neurobiology of Language
357
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
To examine the possibility that different treatment protocols may have been more or less
effective, we repeated the analyses examining perfusion changes over time, but including par-
ticipant Testing site and its interactions with Group, Ring, Hemisphere, and Time. For these
analyses we included age, sexo, y (square root) lesion volume as predictor variables, pero
excluded scanner, given its collinearity with testing site. With respect to the random effects,
including Testing site as a random effect did not improve model fit, so only Participant, Hemi-
sphere, and Time were included as random effects, as above. The results revealed no signif-
icant effects or interactions with testing Site and Time (main effect of site: pag = 0.52; Site × Time
interacción: pag = 0.80; Group × Site × Time: pag = 0.67; Hemisphere × Site × Time: pag = 0.59;
Group × Hemisphere × Site × Time: pag = 0.29; Ring × Site × Time: pag = 0.54; Group × Ring × Site ×
Time: pag = 0.12; Hemisphere × Ring × Site × Time: pag = 0.99; Group × Hemisphere × Ring × Site ×
Time: pag = 0.95). Follow-up contrasts to examine changes in perfusion over time revealed no
significant effect of Time in any perilesional ring in either hemisphere, for both the treatment
and the control group, at any of the three sites (all qs > 0.97).
Discusión
In experiment 2 we looked at whether perfusion in perilesional regions changed in response to
behavioral interventions targeting each person’s diagnosed language impairment (agramma-
tismo, anomia, dysgraphia). Finalmente, we also examined whether pre-treatment perfusion levels
in these regions might predict either the response to treatment or post-treatment language
actuación.
We did not observe any change in resting state perfusion in response to our behavioral
treatment interventions, despite large improvements in language performance on our treat-
ment measures. These results are consistent with the one prior study that examined perfusion
changes in perilesional rings (Boukrina et al., 2019). These null findings did not reflect the fact
that we combined data across three testing sites, where participants were given different treat-
ment protocols and may have had different lesion profiles. Primero, the lesion locations do not
appear to be markedly different across sites (Cifra 3). Además, in our analyses we found no
interactions between perfusion changes over time with site, and no significant changes over
time for any of our ROIs at any site. Thus it seems that the overall null finding reflects consis-
tent results across sites.
Our finding that perfusion did not change over time is unlikely to reflect between-participant
variability due to scanner, lesion volume, or perfusion modifiers, as we followed the same testing
and data processing and analysis procedures as in experiment 1 (see above). These findings are
also unlikely to reflect uncontrolled variability across sessions. Participants were scanned at the
same time of day across sessions, and were asked to maintain their normal caffeine intake for each
session. While we took no special measures to ensure that participants were positioned identically
in the scanner for each session, the pads we added for their comfort and the tight fit of the head
coils allowed for very little variation on this score. To further attempt to quantify the variation across
sessions, we computed the within-subject coefficient of variation (wsCV) over the 16 Participantes
en el grupo de control. Results indicate coefficients of variation from 9.7% a 15.9% across our peri-
lesional rings (Mesa 3). The coefficient of variation was highest for the right hemisphere 0–6 mm
ring (15.9%). Coefficients of variation less than 20% are considered “good” for measures of treat-
ment effects (Quan & Shih, 1996). Thus between-session variability seemed to be low and within
reasonable bounds for us to have been able to detect a treatment effect on perfusion.
These estimates of wsCV also provide an estimate of test–retest reliability for our measure.
This is important to establish, because paradigms with good reliability are better suited to
Neurobiology of Language
358
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
.
/
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
.
/
yo
Cifra 3. Coronal (izquierda), sagittal (mid), and axial (bien) images showing lesion overlap for 61 par-
ticipants in experiment 2, separately for each site. The sagittal view shows the left hemisphere
viewed from the midline.
detect systematic changes over time (p.ej., in response to treatment), whereas paradigms with
poor reliability may be unsuited to detect such systematic changes. Previous findings with
healthy and cognitively impaired adults indicate high test–retest reliability of pCASL
sequences at intervals as long as 4 semanas, using intra-class correlation coefficients (Almeida
et al., 2018; Kilroy et al., 2014). Sin embargo, to our knowledge no prior study has examined
perfusion reliability in any population at an interval as long as 3 meses. While our estimates
Mesa 3. Within-subject coefficient of variation (wsCV) for perilesional perfusion values
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional ring
0–6 mm
6–12 mm
12–18 mm
Left hemisphere
11.8%
10.9%
10.3%
Right hemisphere
15.9%
11.4%
9.7%
359
Neurobiology of Language
Perilesional perfusion in aphasia
of wsCV indicated good reliability, they might nevertheless be improved. One possibility to
improve reliability might be to use multiple post-labeling delay times and 3D imaging
sequences (Kilroy et al., 2014), though we leave this investigation for future work.
We also found that baseline levels of resting state perfusion in our perilesional rings did not
predict responsiveness to treatment, nor did baseline resting state perfusion in these rings pre-
dict post-treatment test scores. These results are consistent with one prior study that also found
no relation between baseline perfusion in perilesional rings and treatment response (Fridriksson
et al., 2012), but are at odds with another that reports a negative effect between treatment
response and perfusion in RH regions homologous to LH perilesional rings (Boukrina et al.,
2019). We saw no relation between RH perfusion and treatment, despite our finding of
abnormally increased perfusion in our RH rings.
One possibility for these findings is that our treatments did not lead to a change in vascular
physiology that affects resting state perfusion in the perilesional rings that we examined. Este
seems clear from the distinct lack of a perfusion change over time. Sin embargo, our treat-
ments were effective at improving language. It may be that perilesional tissue was re-engaged,
but only during active language processing. En ese caso, it may be that responsiveness to our
language treatments in these perilesional rings would be better predicted by measures of
CBF that capture local vascular dilations that occur during a task, such as the time-to-peak
of the hemodynamic response function (Bonakdarpour et al., 2007, 2015; Thompson et al.,
2010). Such measures might reflect improved neural activity or metabolism (Ogoh et al.,
2014). A second possibility is that our participants had already undergone some degree of
functional reorganization prior to our treatment interventions. En ese caso, regions other than the
perilesional tissue may have been compensating for the impaired functions. Our treatments
could therefore have improved the efficiency of such compensation by these other regions,
potentially leading to changes in resting state perfusion outside of the perilesional regions
we examined here. These issues, and the discrepancy between our findings and Boukrina
et al.’s (2019) prior findings in the right hemisphere, require further research.
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
.
/
yo
CONCLUSIONS
En suma, we report four findings related to cerebral perfusion in chronic aphasia subsequent to
stroke. Primero, we find a gradient pattern of perilesional hypoperfusion, with decreasing perfu-
sion with increasing nearness to the lesion. Segundo, we find an island of relatively increased
perfusion in the right (contralesional) hemisferio, that echoes the lesion and, to a lesser
degree, the most proximal perilesional tissue. The behavioral treatments that our participants
were given did effectively improve their language performance on the treatment materials.
Sin embargo, our behavioral treatment interventions did not entail any concomitant changes in
perfusion in our perilesional rings or their RH homologue regions. Finalmente, abnormal baseline
perfusion levels in these perilesional rings or their RH homologues did not predict either
language improvement or post-treatment language performance.
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
EXPRESIONES DE GRATITUD
This work was supported by the NIH-NIDCD, Clinical Research Center Grant, P50DC012283
(PI: Cynthia K. Thompson), and was completed while the first author (Matthew Walenski) era
at Northwestern University. The authors wish to thank Xue Wang, Elena Barbieri, Sladjana
Lukic, and Brianne Dougherty for assistance with data collection and analysis, and to thank
Neda Mohammadi for assistance with literature review.
Neurobiology of Language
360
Perilesional perfusion in aphasia
INFORMACIÓN DE FINANCIACIÓN
Cynthia K. Thompson, National Institute on Deafness and Other Communication Disorders
(https://dx.doi.org/10.13039/100000055), Award ID: P50DC012283.
CONTRIBUCIONES DE AUTOR
Matthew Walenski: Conceptualización; Análisis formal; Visualización; Writing – original
borrador; Writing – review and editing. Yufen Chen: Curación de datos; Metodología; Visualización;
Escritura – borrador original; Writing – review and editing. Kaitlyn A. Litcofsky: Curación de datos.
David Caplan: Conceptualización; Adquisición de financiación; Writing – review and editing. Swathi
Kiran: Conceptualización; Adquisición de financiación; Administración de proyecto; Supervisión. Brenda
Rapp: Conceptualización; Adquisición de financiación; Administración de proyecto; Supervisión. Todd B.
Parrish: Conceptualización; Adquisición de financiación; Administración de proyecto; Supervisión; Writing –
review and editing. Cynthia K. Thompson: Conceptualización; Adquisición de financiación; Proyecto
administración; Supervisión; Writing – review and editing.
REFERENCIAS
Abbott, norte. T., Panadero, C. J., Chen, C., Liu, t. T., & Amar, t. mi.
(2021). Defining hypoperfusion in chronic aphasia: An individ-
ualized thresholding approach. Brain Sciences, 11(4), Article
491. https://doi.org/10.3390/ brainsci11040491, PubMed:
33924446
Almeida, j. r., Greenberg, T., Lu, h., Chase, h. w., Fournier, j. C.,
Cooper, C. METRO., Deckersbach, T., Adams, PAG., Carmody, T., Fava,
METRO., Kurian, B., McGrath, PAG. J., McInnis, METRO. GRAMO., Oquendo, METRO. A.,
Parsey, r., Weissman, METRO., Trivedi, METRO., & Phillips, METRO. l. (2018).
Test-retest reliability of cerebral blood flow in healthy individuals
using arterial spin labeling: Findings from the EMBARC study.
Imagen de resonancia magnética, 45, 26–33. https://doi.org/10
.1016/j.mri.2017.09.004, PubMed: 28888770
alperto, K., Kogan, A., Parrish, T., marco, D., & Wang, l. (2016).
The Northwestern University neuroimaging data archive
(NUNDA). NeuroImagen, 124(Part B), 1131–1136. https://doi.org
/10.1016/j.neuroimage.2015.05.060, PubMed: 26032888
Alsop, D. C., Detre, j. A., Golay, X., Gunther, METRO., Hendrikse, J.,
Hernandez-Garcia, l., Lu, h., MacIntosh, B. J., parque, l. METRO.,
Smits, METRO., van Osch, METRO. j. PAG., Wang, D. j. J., Wong, mi. C., &
Zaharchuk, GRAMO. (2015). Recommended implementation of arterial
spin-labeled perfusion MRI for clinical applications: A consensus
of the ISMRM perfusion study group and the European consor-
tium for ASL in dementia. Resonancia Magnética en Medicina,
73(1), 102–116. https://doi.org/10.1002/mrm.25197, PubMed:
24715426
Barbieri, MI., Mack, J., Chiappetta, B., Europa, MI., & Thompson, C. k.
(2019). Recovery of offline and online sentence processing in
aphasia: Language and domain-general network neuroplasticity.
Corteza, 120, 394–418. https://doi.org/10.1016/j.cortex.2019.06
.015, PubMed: 31419597
Benjamini, y., & Hochberg, Y. (1995). Controlling the false discov-
ery rate: A practical and powerful approach to multiple testing.
Journal of the Royal Statistical Society. Serie B (Methodological),
57(1), 289–300. https://doi.org/10.1111/j.2517-6161.1995
.tb02031.x
Bonakdarpour, B., Beeson, PAG. METRO., DeMarco, A. T., & Rapcsak, S. z.
(2015). Variability in blood oxygen level dependence (BOLD)
signal in patients with stroke-induced and primary progressive
aphasia. NeuroImagen: Clinical, 8, 87–94. https://doi.org/10
.1016/j.nicl.2015.03.014, PubMed: 26106531
Bonakdarpour, B., Parrish, t. B., & Thompson, C. k. (2007). Hemo-
dynamic response function in patients with stroke-induced
aphasia: Implications for fMRI data analysis. NeuroImagen, 36(2),
322–331. https://doi.org/10.1016/j.neuroimage.2007.02.035,
PubMed: 17467297
Boukrina, o., Barrett, A. METRO., & Tumbas, W.. W.. (2019). Cerebral per-
fusion of the left reading network predicts recovery of reading in
subacute to chronic stroke. Mapeo del cerebro humano, 40(18),
5301–5314. https://doi.org/10.1002/ hbm.24773, PubMed:
31452284
Brumm, k. PAG., Perthen, j. MI., Liu, t. T., Haist, F., Ayalon, l., & Amar,
t. (2010). An arterial spin labeling investigation of cerebral blood
flow deficits in chronic stroke survivors. NeuroImagen, 51(3),
995–1005. https://doi.org/10.1016/j.neuroimage.2010.03.008,
PubMed: 20211268
Chen, y., Wolk, D. A., Reddin, j. S., Korczykowski, METRO., Martinez,
PAG. METRO., Musiek, mi. S., Newberg, A. B., Julin, PAG., arnold, S. MI.,
Greenberg, j. h., & Detre, j. A. (2011). Voxel-level comparison
of arterial spin-labeled perfusion MRI and FDG-PET in Alzheimer
enfermedad. Neurología, 77(22), 1977–1985. https://doi.org/10.1212
/ WNL.0b013e31823a0ef7, PubMed: 22094481
Chollet, F., Di Piero, v., Inteligente, R. J., Arroyos, D. J., Dolan, R. J., &
Frackowiak, R. S. (1991). The functional anatomy of motor
recovery after stroke in humans: A study with positron emission
tomography. Annals of Neurology, 29(1), 63–71. https://doi.org
/10.1002/ana.410290112, PubMed: 1996881
Clement, PAG., Mutsaerts, H.-J., Václavů, l., Ghariq, MI., Pizzini, F. B.,
Smits, METRO., Acou, METRO., Jovicich, J., Vanninen, r., Kononen, METRO.,
Wiest, r., Rostrup, MI., Bastos-Leite, A. J., Larsson, E.-M., &
Achten, mi. (2018). Variability of physiological brain perfusion
in healthy subjects: A systematic review of modifiers. Considerar-
ations for multi-center ASL studies. Journal of Cerebral Blood
Flow and Metabolism, 38(9), 1418–1437. https://doi.org/10
.1177/0271678X17702156, PubMed: 28393659
dai, w., Garcia, D., de Bazelaire, C., & Alsop, D. C. (2008). Estafa-
tinuous flow-driven inversion for arterial spin labeling using
pulsed radio frequency and gradient fields. Resonancia magnetica
Neurobiology of Language
361
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
En medicina, 60(6), 1488–1497. https://doi.org/10.1002/mrm
.21790, PubMed: 19025913
Du, A. T., Jahng, GRAMO. h., Hayasaka, S., Kramer, j. h., rosa, h. J.,
Gorno-Tempini, METRO. l., Rankin, k. PAG., Molinero, B. l., Weiner, METRO. w.,
& Schuff, norte. (2006). Hypoperfusion in frontotemporal dementia
and Alzheimer disease by arterial spin labeling MRI. Neurología,
67(7), 1215–1220. https://doi.org/10.1212/01.wnl.0000238163
.71349.78, PubMed: 17030755
Fridriksson, J., Richardson, j. D., Fillmore, PAG., & Cai, B. (2012). Left
hemisphere plasticity and aphasia recovery. NeuroImagen, 60(2),
854–863. https://doi.org/10.1016/j.neuroimage.2011.12.057,
PubMed: 22227052
Fridriksson, J., Rorden, C., morgan, PAG. S., Morrow, k. l., & Baylis,
GRAMO. C. (2006). Measuring the hemodynamic response in chronic
hypoperfusion. Neurocase, 12(3), 146–150. https://doi.org/10
.1080/13554790600598816, PubMed: 16801150
Gilmore, NORTE., Meier, mi. l., Johnson, j. PAG., & Kiran, S. (2020). Typicality-
based semantic treatment for anomia results in multiple levels
of generalisation. Neuropsychological Rehabilitation, 30(5),
802–828. https://doi.org/10.1080/09602011.2018.1499533,
PubMed: 30027828
hamilton, R. h., Chrysikou, mi. GRAMO., & Coslett, B. (2011). Mecha-
nisms of aphasia recovery after stroke and the role of noninvasive
brain stimulation. Brain and Language, 118(1–2), 40–50. https://
doi.org/10.1016/j.bandl.2011.02.005, PubMed: 21459427
Hara, T., Abo, METRO., Kobayashi, K., Watanabe, METRO., Kakuda, w., &
Senoo, A. (2015). Effects of low-frequency repetitive transcranial
magnetic stimulation combined with intensive speech therapy
on cerebral blood flow in post-stroke aphasia. Translational
Stroke Research, 6(5), 365–374. https://doi.org/10.1007/s12975
-015-0417-7, PubMed: 26245774
Hara, y., Obayashi, S., Tsujiuchi, K., & Muraoka, Y. (2013). El
effects of electromyography-controlled functional electrical stim-
ulation on upper extremity function and cortical perfusion in
stroke patients. Clinical Neurophysiology, 124(10), 2008–2015.
https://doi.org/10.1016/j.clinph.2013.03.030, PubMed:
23706813
Herscovitch, PAG., & Raichle, METRO. mi. (1985). What is the correct value
for the brain-blood partition coefficient for water? Diario de
Cerebral Blood Flow and Metabolism, 5(1), 65–69. https://doi
.org/10.1038/jcbfm.1985.9, PubMed: 3871783
Hillis, A. mi. (2005). Brain/language relationships identified with dif-
fusion and perfusion MRI: Clinical applications in neurology and
neurosurgery. Annals of the New York Academy of Sciences,
1064, 149–161. https://doi.org/10.1196/annals.1340.027,
PubMed: 16394154
Hillis, A. mi. (2007). Magnetic resonance perfusion imaging in the
study of language. Brain and Language, 102(2), 165–175.
https://doi.org/10.1016/j.bandl.2006.04.016, PubMed:
16757020
Hu, w., Wang, Z., Sotavento, V.-Y., Trojanowski, J., Detre, J., & Grossman,
METRO. (2010). Distinct cerebral perfusion patterns in FTLD and AD.
Neurología, 75(10), 881–888. https://doi.org/10.1212/ WNL
.0b013e3181f11e35, PubMed: 20819999
Johnson, j. PAG., Meier, mi. l., Cacerola, y., & Kiran, S. (2019). Tratamiento-
related changes in neural activation vary according to treatment
response and extent of spared tissue in patients with chronic
aphasia. Corteza, 121, 147–168. https://doi.org/10.1016/j.cortex
.2019.08.016, PubMed: 31627014
kay, J., Menor, r., & Coltheart, METRO. (1996). Psycholinguistic assess-
ments of language processing in aphasia (PALPA): An introduc-
ción. Aphasiology, 10(2), 159–180. https://doi.org/10.1080
/02687039608248403
Kertesz, A. (2006). Western Aphasia Battery—Revised ( WAB-R).
Pearson. https://doi.org/10.1037/t15168-000
Kilroy, MI., Apostolova, l., Liu, C., yan, l., Ringman, J., & Wang, D. j.
(2014). Reliability of two dimensional and three dimensional
pseudo-continuous arterial spin labeling perfusion MRI in elderly
poblaciones: Comparison with 15O-water positron emission
tomography. Journal of Magnetic Resonance Imaging, 39(4),
931–939. https://doi.org/10.1002/jmri.24246, PubMed: 24038544
Könönen, METRO., Kuikka, j. T., Husso-Saastamoinen, METRO., Vanninen, MI.,
Vanninen, r., Soimakallio, S., Mervaala, MI., Sivenius, J., Pitkänen,
K., & Tarkka, I. METRO. (2005). Increased perfusion in motor areas
after constraint-induced movement therapy in chronic stroke:
A single-photon emission computerized tomography study.
Journal of Cerebral Blood Flow and Metabolism, 25(12),
1668–1674. https://doi.org/10.1038/sj.jcbfm.9600158, PubMed:
15931162
Kunz, A., & Iadecola, C. (2008). Cerebral vascular dysregulation
in the ischemic brain. Handbook of Clinical Neurology, 92,
283–305. https://doi.org/10.1016/S0072-9752(08)01914-3,
PubMed: 18790280
Lakens, D. (2013). Calculating and reporting effect sizes to facilitate
cumulative science: A practical primer for t-tests and ANOVAs.
Fronteras en psicología, 4, 863. https://doi.org/10.3389/fpsyg
.2013.00863, PubMed: 24324449
Sotavento, R. GRAMO., & van Donkelaar, PAG. (1995). Mechanisms underlying
functional recovery following stroke. Canadian Journal of Neuro-
logical Sciences/Journal Canadien des Sciences Neurologiques,
22(4), 257–263. https://doi.org/10.1017/S0317167100039445,
PubMed: 8599767
Amar, T., Swinney, D., Wong, MI., & Buxton, R. (2002). Perfusion
imaging and stroke: A more sensitive measure of the brain bases
of cognitive deficits. Aphasiology, 16(9), 873–883. https://doi.org
/10.1080/02687030244000356, PubMed: 30906100
Lu, h., Clingman, C., Golay, X., & van Zijl, PAG. C. METRO. (2004). Deter-
mining the longitudinal relaxation time (T1) of blood at 3.0 Tesla.
Resonancia Magnética en Medicina, 52(3), 679–682. https://doi.org
/10.1002/mrm.20178, PubMed: 15334591
Miao, PAG., Wang, C., li, PAG., Wei, S., Deng, C., Zheng, D., & cheng, j.
(2018). Altered gray matter volume, cerebral blood flow and
functional connectivity in chronic stroke patients. Neurociencia
Letras, 662, 331–338. https://doi.org/10.1016/j.neulet.2017.05
.066, PubMed: 28919535
Mugler, j. PAG., & Brookeman, j. R. (1990). Three-dimensional
magnetization-prepared rapid gradient-echo imaging (3D MP
RAGE). Resonancia Magnética en Medicina, 15(1), 152–157.
https://doi.org/10.1002/mrm.1910150117, PubMed: 2374495
Ogoh, S., Tsukamoto, h., Hirasawa, A., Hasegawa, h., Hiros, NORTE., &
Hashimoto, t. (2014). The effect of changes in cerebral blood
flow on cognitive function during exercise. Physiological
Informes, 2(9), Article e12163. https://doi.org/10.14814/phy2
.12163, PubMed: 25263210
Quan, h., & Shih, W.. j. (1996). Assessing reproducibility by the
within-subject coefficient of variation with random effects
modelos. Biometrics, 52(4), 1195–1203. https://doi.org/10.2307
/2532835, PubMed: 8962450
Richardson, j. D., Panadero, j. METRO., morgan, PAG. S., Rorden, C., Bonilha,
l., & Fridriksson, j. (2011). Cerebral perfusion in chronic stroke:
Implications for lesion-symptom mapping and functional MRI.
Behavioral Neurology, 24, Article 380810. https://doi.org/10
.3233/BEN-2011-0283, PubMed: 21606572
Rorden, C., & Brett, METRO. (2000). Stereotaxic display of brain lesions.
Behavioural Neurology, 12(4), 191–200. https://doi.org/10.1155
/2000/421719, PubMed: 11568431
Neurobiology of Language
362
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Perilesional perfusion in aphasia
SAS Institute. (2012). SAS 9.4 for Windows [software]. https://
support.sas.com
Saur, D., Lange, r., Baumgartner, A., Schraknepper, v., Willmes, K.,
Rijntjes, METRO., & Weiller, C. (2006). Dynamics of language reorga-
nization after stroke. Cerebro, 129(6), 1371–1384. https://doi.org/10
.1093/brain/awl090, PubMed: 16638796
Shea, J., wiley, r., Moss, NORTE., & Rapp, B. (2020). Pseudoword spell-
ing ability predicts response to word spelling treatment in
acquired dysgraphia. Neuropsychological Rehabilitation, 1–37.
https://doi.org/10.1080/09602011.2020.1813596, PubMed:
33047661
Thompson, C. k. (2011). Northwestern assessment of verbs and sen-
tenencias (NAVS). Northwestern University.
Thompson, C. K., den Ouden, D. B., Bonakdarpour, B., Garibaldi,
K., & Parrish, t. B. (2010). Neural plasticity and treatment-
induced recovery of sentence processing in agrammatism.
Neuropsicología, 48(11), 3211–3227. https://doi.org/10.1016/j
.neuropsychologia.2010.06.036, PubMed: 20603138
Thompson, C. K., & Shapiro, l. (2005). Treating agrammatic apha-
sia within a linguistic framework: Treatment of underlying forms.
Aphasiology, 19(10–11), 1021–1036. https://doi.org/10.1080
/02687030544000227, PubMed: 17410280
Thompson, C. K., Walenski, METRO., Chen, y., Caplan, D., Kiran, S., Rapp,
B., Grunewald, K., Núñez, METRO., Zinbarg, r., & Parrish, t. B. (2017).
Intrahemispheric perfusion in chronic stroke-induced aphasia.
Neural Plasticity, 2017, Article 2361691. https://doi.org/10.1155
/2017/2361691, PubMed: 28357141
Thompson, C. K., & Weintraub, S. (2014). Northwestern naming
battery. Northwestern University.
Wang, C., Miao, PAG., Liu, J., Wei, S., guo, y., li, Z., Zheng, D., &
cheng, j. (2019). Cerebral blood flow features in chronic subcor-
tical stroke: Lesion location-dependent study. Brain Research,
1706, 177–183. https://doi.org/10.1016/j.brainres.2018.11.009,
PubMed: 30419222
Wang, z. (2012). Improving cerebral blood flow quantification for
arterial spin labeled perfusion MRI by removing residual motion
artifacts and global signal fluctuations. Resonancia magnetica
Imaging, 30(10), 1409–1415. https://doi.org/10.1016/j.mri.2012
.05.004, PubMed: 22789842
Wang, Z., Aguirre, GRAMO. K., Rao, h., Wang, J., Fernández-Seara,
METRO. A., Childress, A. r., & Detre, j. A. (2008). Empirical optimiza-
tion of ASL data analysis using an ASL data processing toolbox:
ASLtbx. Imagen de resonancia magnética, 26(2), 261–269. https://
doi.org/10.1016/j.mri.2007.07.003, PubMed: 17826940
wiley, R. w., & Rapp, B. (2019). Statistical analysis in Small-N
Designs: Using linear mixed-effects modeling for evaluating
intervention effectiveness. Aphasiology, 33(1), 1–30. https://doi
.org/10.1080/02687038.2018.1454884, PubMed: 33012945
yo
D
oh
w
norte
oh
a
d
mi
d
F
r
oh
metro
h
t
t
pag
:
/
/
d
i
r
mi
C
t
.
metro
i
t
.
mi
d
tu
norte
oh
/
yo
/
yo
a
r
t
i
C
mi
–
pag
d
F
/
/
/
/
3
2
3
4
5
2
0
2
2
8
2
3
norte
oh
_
a
_
0
0
0
6
8
pag
d
/
.
yo
F
b
y
gramo
tu
mi
s
t
t
oh
norte
0
7
S
mi
pag
mi
metro
b
mi
r
2
0
2
3
Neurobiology of Language
363