RESEARCH ARTICLE
Leukoaraiosis is Not Associated With Recovery
From Aphasia in the First Year After Stroke
Alexandra C. Brito1, Deborah F. Levy2
, Sarah M. Schneck2
, Jillian L. Entrup2
,
Caitlin F. Onuscheck2, Marianne Casilio2
, Michael de Riesthal2
,
l. Taylor Davis3
, and Stephen M. Wilson2,3,4
1School of Medicine, Vanderbilt University, Nashville, TN, USA
2Department of Hearing and Speech Sciences, Vanderbilt University Medical Center, Nashville, TN, USA
3Department of Radiology, Vanderbilt University Medical Center, Nashville, TN, USA
4School of Health and Rehabilitation Sciences, University of Queensland, Brisbane, Australia
Keywords: aphasia, brain health, cerebral small vessel disease, leukoaraiosis, stroke
ABSTRACT
After a stroke, individuals with aphasia often recover to a certain extent over time. Questo
recovery process may be dependent on the health of surviving brain regions. Leukoaraiosis
(white matter hyperintensities on MRI reflecting cerebral small vessel disease) is one indication
of compromised brain health and is associated with cognitive and motor impairment. Previous
studies have suggested that leukoaraiosis may be a clinically relevant predictor of aphasia
outcomes and recovery, although findings have been inconsistent. We investigated the
relationship between leukoaraiosis and aphasia in the first year after stroke. We recruited
267 patients with acute left hemispheric stroke and coincident fluid attenuated inversion
recovery MRI. Patients were evaluated for aphasia within 5 days of stroke, E 174 patients
presented with aphasia acutely. Of these, 84 patients were evaluated at ∼3 months post-stroke
or later to assess longer-term speech and language outcomes. Multivariable regression
models were fit to the data to identify any relationships between leukoaraiosis and initial
aphasia severity, extent of recovery, or longer-term aphasia severity. We found that
leukoaraiosis was present to varying degrees in 90% of patients. Tuttavia, leukoaraiosis did
not predict initial aphasia severity, aphasia recovery, or longer-term aphasia severity. The lack
of any relationship between leukoaraiosis severity and aphasia recovery may reflect the
anatomical distribution of cerebral small vessel disease, which is largely medial to the white
matter pathways that are critical for speech and language function.
INTRODUCTION
Aphasia, an acquired impairment of language, is a common and debilitating consequence of
many left hemispheric strokes. Frequently, patients with aphasia recover language function
over time to varying extents. Prior work investigating the course of language recovery demon-
strated that the most rapid gains in speech and language function are made in the first year
after stroke
(Kertesz & McCabe, 1977; Pedersen et al., 1995, Swinburn et al., 2004; Wilson
et al., 2023). A wide range of patient-related and stroke-related factors have been evaluated as
predictors of aphasia recovery, with lesion location and extent proving most influential (Basso,
1992; Plowman et al., 2012; Watila & Balarabe, 2015; Wilson et al., 2023). Aphasia recovery
is thought to be driven by neural plasticity, questo è, the functional reorganization of surviving
a n o p e n a c c e s s
j o u r n a l
Citation: Brito, UN. C., Levy, D. F.,
Schneck, S. M., Entrup, J. L.,
Onuscheck, C. F., Casilio, M., Di
Riesthal, M., Davis L. T., & Wilson, S. M.
(2023). Leukoaraiosis is not associated
with recovery from aphasia in the first
year after stroke. Neurobiology of
Language. Advance publication.
https://doi.org/10.1162/nol_a_00115
DOI:
https://doi.org/10.1162/nol_a_00115
Supporting Information:
https://doi.org/10.1162/nol_a_00115
Received: 14 ottobre 2022
Accepted: 28 Giugno 2023
Competing Interests: The authors have
declared that no competing interests
exist.
Corresponding Author:
Stephen M. Wilson
smwilson@uq.edu.au
Handling Editor:
Julius Fridriksson
Copyright: © 2023
Istituto di Tecnologia del Massachussetts
Pubblicato sotto Creative Commons
Attribuzione 4.0 Internazionale
(CC BY 4.0) licenza
The MIT Press
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
l
/
.
/
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
.
/
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Q1
Leukoaraiosis and recovery from aphasia
brain regions such that they take on new or enhanced roles in language processing (Hartwigsen &
Saur, 2019; Wilson & Schneck, 2021). The potential for neuroplastic recovery from aphasia
may depend in part on the health of surviving brain regions (Basilakos et al., 2019; Johnson
et al., 2022; Varkanitsa et al., 2020; Wright et al., 2018).
A major contributor to brain health is cerebral small vessel disease (cSVD), which is a lead-
ing cause of cognitive decline and functional impairment in older adults (Pantoni, 2010;
ter Telgte et al., 2018). Neuroimaging biomarkers associated with cSVD include leukoaraiosis,
lacunar infarcts, and microhemorrhages. Leukoaraiosis refers to diffuse bilateral and symmet-
rical white matter abnormalities localized to periventricular and subcortical white matter that
are hyperintense on fluid attenuated inversion recovery (FLAIR) magnetic resonance imaging
(MRI) and hypodense on computed tomography (CT). Leukoaraiosis is very common in older
individuals, and is associated with age, hypertension, and other cardiovascular risk factors
(de Leeuw et al., 2001; Longstreth et al., 1996). The clinical findings associated with leukoar-
aiosis include cognitive decline (Au et al., 2006; de Groot et al., 2000), depression (Teodorczuk
et al., 2010), apathy (Hollocks et al., 2015), gait disturbances (Baezner et al., 2008), poorer
stroke outcomes (Arsava et al., 2009; Kissela et al., 2009; Ryu et al., 2017), and increased risk
of stroke and dementia (Debette et al., 2010; Debette & Markus, 2010).
While the association between leukoaraiosis and cognition is robust, only a few studies
have investigated whether leukoaraiosis is predictive of recovery from aphasia after stroke.
One recent well-powered study found that leukoaraiosis contributes to aphasia severity in
chronic stroke patients (Johnson et al., 2022). Several smaller studies have reported associa-
tions between leukoaraiosis and naming (Wright et al., 2018), aphasia severity (Wilmskoetter
et al., 2019), longitudinal change in aphasia severity in the chronic post-stroke period
(Basilakos et al., 2019), and improvement on trained items in the context of aphasia treatment
(Varkanitsa et al., 2020). Only one study has investigated the effect of leukoaraiosis on the
presence of acute aphasia, finding no relationship (Flowers et al., 2017). No study to our
knowledge has explored whether leukoaraiosis is associated with the extent of recovery from
aphasia in the early post-stroke period. This phase is particularly important to investigate,
because the majority of behavioral gains take place in the first year after stroke (Kertesz &
McCabe, 1977; Pedersen et al., 1995, Swinburn et al., 2004; Wilson et al., 2023).
To explore the hypothesis that recovery from aphasia depends on the health of surviving
brain regions, we examined leukoaraiosis as a predictor of initial aphasia severity, aphasia
recovery, and longer-term aphasia severity in the context of a large prospective study of indi-
viduals recovering from aphasia after stroke. We hypothesized that more extensive leukoaraio-
sis might be associated with more severe aphasia in the acute phase, less recovery over time,
and/or poorer longer-term aphasia outcomes. A better understanding of the factors that con-
tribute to recovery from aphasia will enhance the accuracy of prognoses and may provide
clues as to how recovery can be maximized.
METHODS
This study is one component of a prospective longitudinal study of the neural correlates of
recovery from aphasia; see Wilson et al. (2023) for additional methodological details. Nostro
study was conducted in accordance with the principles of the 1964 Declaration of Helsinki
and was approved by the Institutional Review Board at Vanderbilt University Medical Center.
All patients or their legally authorized representatives provided written informed consent to
participate in the study.
Neurobiology of Language
2
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
l
/
/
.
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
/
.
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Leukoaraiosis and recovery from aphasia
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
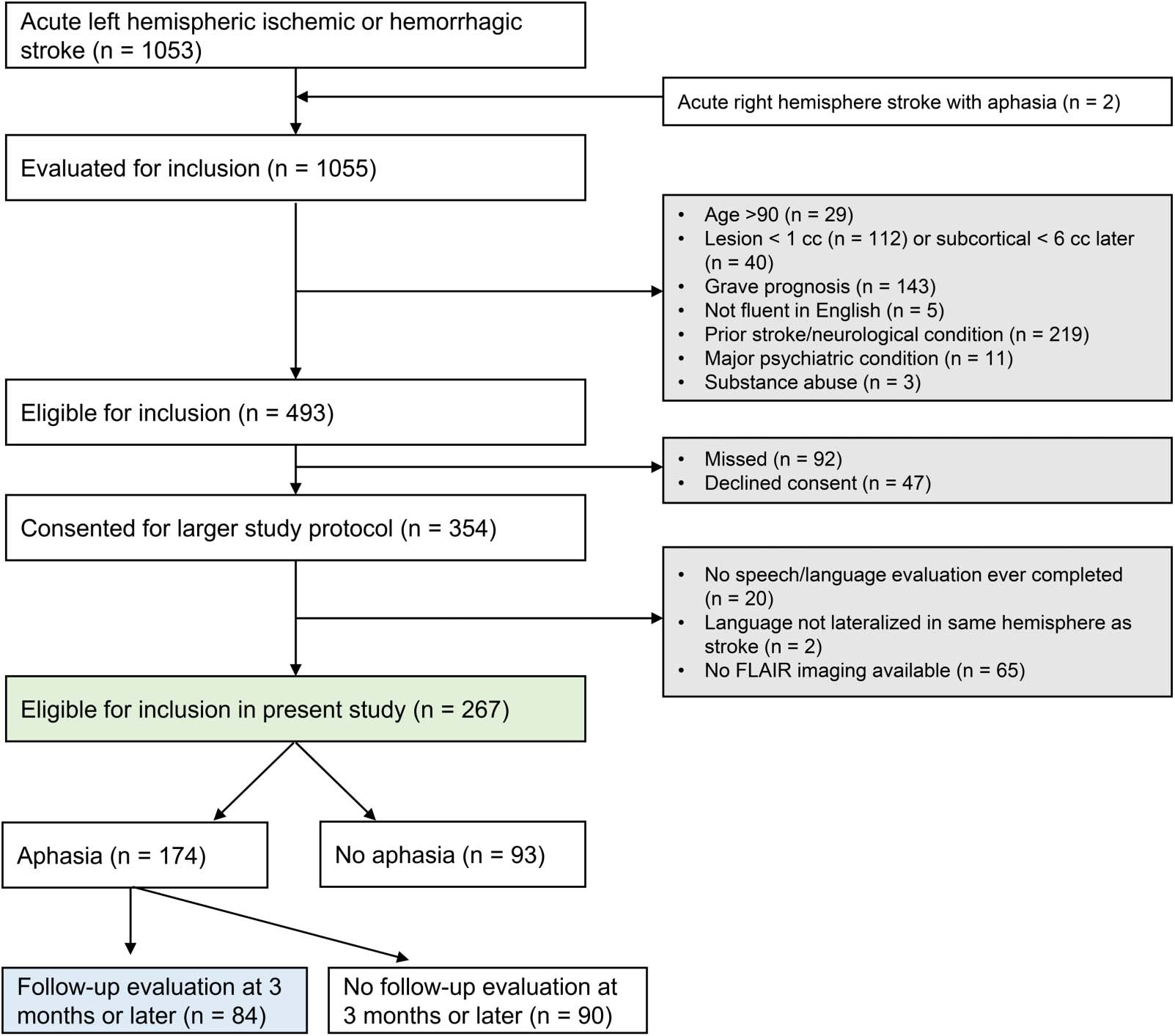
Figura 1. Consort diagram. The green shading signifies patients included in the first analyses (cioè., initial aphasia severity). The blue shading
indicates patients included in the second and third analyses (cioè., patients with longitudinal follow-up). FLAIR = fluid attenuated inversion recovery.
l
.
/
/
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
.
/
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Participants
We considered for inclusion all patients presenting at Vanderbilt University Medical Center
between late 2016 and early 2020. Our inclusion criteria were: (1) acute ischemic or intrace-
rebral hemorrhagic stroke predominantly confined to left hemisphere supratentorial regions, O
right hemisphere stroke with aphasia clearly indicating right hemisphere language dominance;
(2) age 18–90 years; E (3) infarct at least 1 cm3 except (io) thalamic infarcts were included
regardless of extent; (ii) starting after ∼21 months of data collection, basal ganglia and/or sub-
cortical white matter infarcts were included only if they exceeded ∼6 cm3. Our exclusion cri-
teria were: (1) unconscious with grave prognosis; (2) not fluent in English premorbidly, COME
determined by interview with the patient and/or caregiver; (3) prior symptomatic stroke signif-
icantly impacting language regions or homotopic regions, neurodegenerative disease, or any
other neurological condition impacting language or cognition; (4) major psychiatric disorder;
E (5) substance abuse serious enough to interfere with study participation.
As detailed in Figure 1, 1,055 patients met the first inclusion criterion and were evaluated
for inclusion, and ultimately 354 met all criteria and consented to participate. For the present
analysis of leukoaraiosis in relation to aphasia outcomes, we additionally required (1) almeno
one speech/language evaluation; (2) availability of acute FLAIR imaging; E (3) lingua
Neurobiology of Language
3
Leukoaraiosis and recovery from aphasia
lateralized to stroke hemisphere. A total of 20 patients had no speech/language evaluation, 65
did not have FLAIR imaging (most of these had only CT), E 2 patients had left hemisphere
strokes but strong evidence for right hemisphere language dominance, in partenza 267 included
participants. Demographic and key medical history data for the included patients are shown in
Tavolo 1.
Aphasia Assessment
Speech and language function were initially assessed at the bedside within the first 5 days after
stroke, on mean day 2.7 (SD = 1.3, range = 0, 5). We used the Quick Aphasia Battery (QAB),
which is a time-efficient aphasia assessment that has been validated in the acute care context
(Wilson, Eriksson, et al., 2018). The QAB shows excellent sensitivity, specificity, test–retest
reliability, and concurrent validity with respect to the Western Aphasia Battery ( WAB), E
is sensitive to change in the acute period and beyond (Wilson et al., 2019, 2023). Aphasia
severity was quantified with the QAB overall score, which ranges from 0 A 10 con 10 rep-
resenting a perfect score and 0 reflecting the most severe aphasia; patients who were untest-
able were also scored as 0. The overall score reflects performance on multiple speech and
language domains including word and sentence comprehension, word finding, grammatical
construction, phonological encoding, speech motor programming, and reading aloud. Tutto
language evaluations were administered by certified speech-language pathologists (SMS,
JLE, CFO). Audio and video recordings were made of all sessions, which were transcribed
and scored offline. All scores were reviewed in consensus meetings of from four to six of
the authors.
For all patients who presented with acute aphasia per clinical impression, we then
attempted to obtain additional speech-language evaluations at ∼1 month, ∼3 months and
∼12 months. Note that we considered clinical impression to be the gold standard for aphasia
diagnosis and that some patients with aphasia per clinical impression scored above the QAB
cutoff for aphasia (Wilson, Eriksson, et al., 2018). Most follow-up evaluations were performed
at Vanderbilt University Medical Center, inpatient rehabilitation facilities, or patients’ homes.
Some of the final time point evaluations were obtained considerably later than 12 months due
to the COVID-19 pandemic. For the present study, we were concerned with longer term apha-
sia outcomes, so we included in our longitudinal analyses all patients who were seen at the ∼3
month time point or later; for each patient we used the latest time point available. The ratio-
nale for this was that language recovery was relatively modest between 3 months and 12
months (Wilson et al., 2023), and it was straightforward to include in models the time post
onset that the final speech-language evaluation was obtained. There were 174 patients with
initial aphasia, of whom 84 were included in the analysis of longer-term outcomes. These
longer-term evaluations were acquired on mean day 315 (SD = 163, range = 85, 665).
Information regarding the amount of speech-language therapy received between discharge
from acute care and the final assessment was available for 76 out of 84 patients: Patients
received a mean of 54.7 min of treatment per week (SD = 57.7, range = 0, 215); note that
20 patients reported receiving no treatment.
Evaluation of Leukoaraiosis
Acute FLAIR images obtained in the course of routine clinical care were evaluated for degree
of leukoaraiosis on acute MRI scans using the Fazekas visual rating scale (Fazekas et al., 1987).
There are several techniques for assessing leukoaraiosis by visual inspection. A meta-analysis
of the six most commonly used rating scales showed an overall high correlation among all
Neurobiology of Language
4
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
l
.
/
/
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
.
/
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Leukoaraiosis and recovery from aphasia
Tavolo 1.
Participant demographics.
All participants
Participants with longitudinal follow-up
Number of participants, N
Age in years, mean (SD)
Female, N (%)
Handedness
Right-handed, N (%)
Left-handed or ambidextrous, N (%)
Race
Black, N (%)
White, N (%)
Other, N (%)
Education in years, mean (SD)
Comorbidities
Hypertension, N (%)
Diabetes mellitus, N (%)
Hyperlipidemia, N (%)
Tobacco use (current or former), N (%)
Lesion extent in cm3, mean (SD)
Damage to core language areas in cm3, mean (SD)
NIHSS on admission, mean (SD)*
Stroke subtype
Hemorrhagic, N (%)
Cardioembolic, N (%)
Large vessel, N (%)
Small vessel, N (%)
Other/undetermined etiology, N (%)
Hemorrhagic transformation
Yes, N (%)
No, N (%)
267
62.6 (14.3)
138 (51.7%)
234 (87.6%)
33 (12.4%)
35 (13.6%)
231 (86.5%)
1 (0.4%)
13.1 (3.1)
205 (76.8%)
76 (28.4%)
147 (55.1%)
148 (55.4%)
40.2 (56.2)
9.2 (15.9)
7.7 (7.2)
33 (12.4%)
84 (31.5%)
50 (18.7%)
15 (5.6%)
85 (31.8%)
31 (11.6%)
236 (88.4%)
84
62.5 (13.4)
38 (45.2%)
72 (85.7%)
12 (14.3%)
9 (10.7%)
74 (88.1%)
1 (1.2%)
13.3 (2.9)
64 (76.2%)
25 (29.8%)
53 (63.1%)
50 (59.5%)
69.1 (77.8)
17.3 (22.0)
9.0 (7.2)
11 (12.9%)
28 (32.9%)
15 (17.6%)
2 (2.4%)
28 (32.9%)
10 (11.8%)
74 (87.1%)
Note. *NIHSS scores missing on chart review for 31 patients in the overall patient group and for 12 patients with longitudinal follow-up. NIHSS = National
Institutes of Health Stroke Scale.
Neurobiology of Language
5
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
l
.
/
/
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
.
/
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Leukoaraiosis and recovery from aphasia
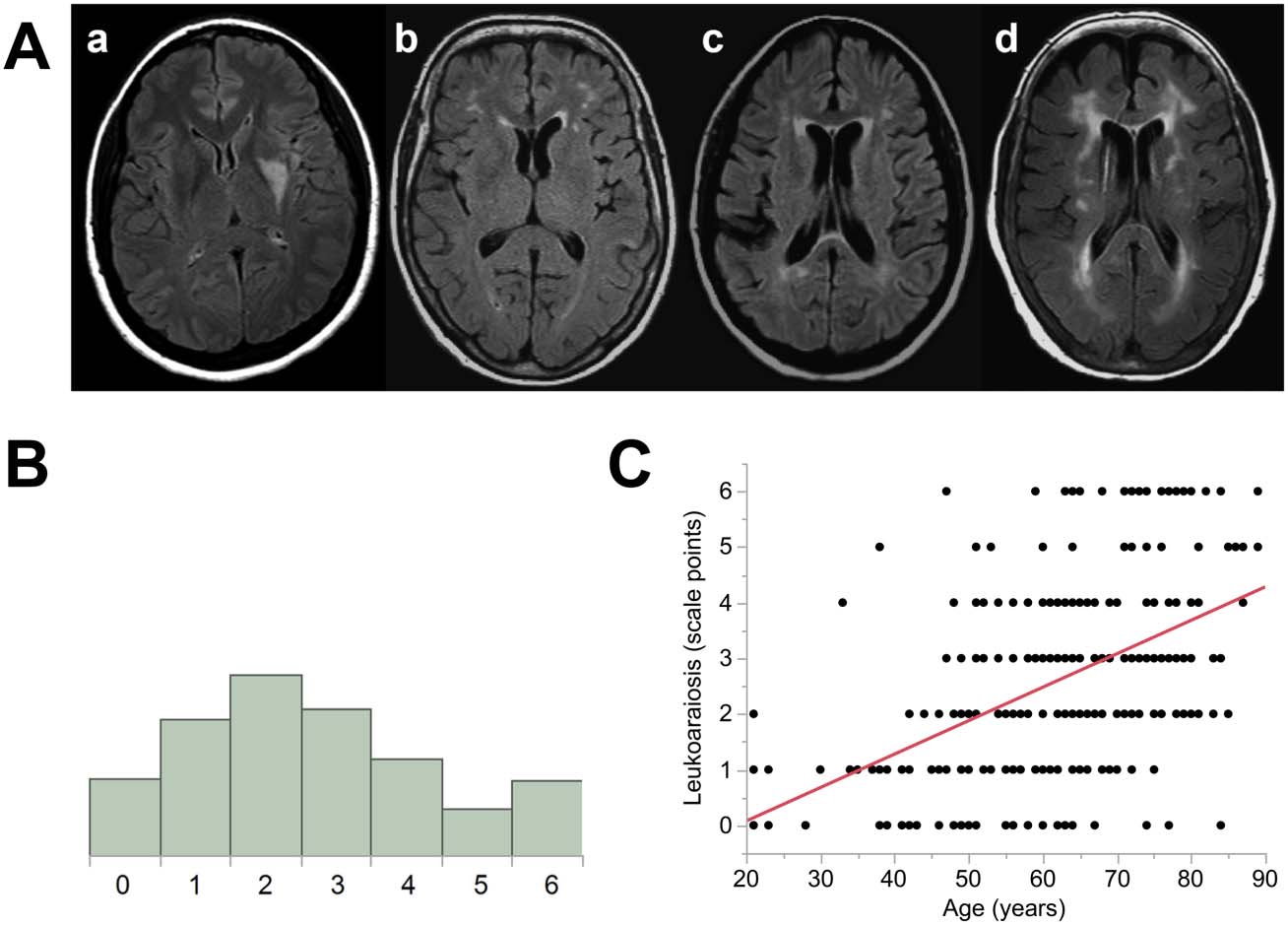
Leukoaraiosis in participant data. (UN) Range of leukoaraiosis severity. Written as [peri-
Figura 2.
ventricular-deep]. a = [0–0], b = [1–1], c = [2–2], d = [3–3]. (B) Distribution of leukoaraiosis ratings.
(C) Correlation between age and leukoaraiosis ratings for all patients.
rating scales and no benefit of using one scale over another (Pantoni et al., 2002). We decided
to use the Fazekas scale because it is most commonly used clinically and because it takes into
account both periventricular and deep white matter hyperintensities, which are scored
separately.
In the Fazekas scale, periventricular and deep white matter hyperintensities are rated on a
scale from 0 A 3, which are summed for a composite score ranging from 0 A 6. For periven-
tricular ratings, the following criteria were used: 0 = no lesions, 1 = caps or thin line, 2 =
smooth halo around ventricles, 3 = extension into the white matter. For deep white matter
hyperintensities, we scored as follows: 0 = no lesions, 1 = punctate foci, 2 = beginning con-
fluence of foci, 3 = large confluent areas. See Figure 2A for four representative MRI scans.
Raters were members of the research team (ACB, DFL), who were trained on the assessment
of leukoaraiosis by a neuroradiologist (LTD). They were blinded to all clinical information
besides the MR images. Leukoaraiosis was examined in both hemispheres, except that hyper-
intensities in the immediate vicinity of the infarct were not interpreted as leukoaraiosis.
Initial ratings from the two raters exhibited excellent inter-rater reliability (Cicchetti, 1994),
with an inter-class correlation coefficient of 0.83 (type A-1). All discrepancies in ratings were
resolved by discussion between the two raters, in consultation with the neuroradiologist as
necessary, to derive final ratings that were used in subsequent analyses.
Lesion Mapping
Lesion location and extent are the most important determinants of aphasia outcome. A
include these factors in our models, stroke lesions were manually delineated on acute clinical
imaging and normalized to standard space (Wilson et al., 2023). Lesion extent was calculated
in all of dominant hemisphere supratentorial cortex. Damage to key language areas was quan-
tified as lesion extent within regions activated by either of two language mapping paradigms,
Neurobiology of Language
6
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
l
/
/
.
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
/
.
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Leukoaraiosis and recovery from aphasia
one using a semantic decision task and the other using a phonological decision task (Wilson,
Yen, & Eriksson, 2018; Yen et al., 2019). These functional maps were based on 16 neurolog-
ically normal individuals (Yen et al., 2019) and were thresholded at a voxelwise threshold
of p < 0.005, then corrected at p < 0.05 based on cluster extent using permutation analysis.
The language areas identified included the inferior frontal gyrus, ventral precentral gyrus,
superior temporal sulcus, middle temporal gyrus, posterior inferior temporal gyrus, supramar-
ginal gyrus, and midline superior frontal gyrus (Yen et al., 2019).
Statistical Analysis
Three linear models were constructed in order to evaluate the effect of leukoaraiosis on
(1) initial QAB scores, (2) aphasia recovery, and (3) longer-term QAB scores. Our statistical
approach was closely based on Wilson et al. (2023). All three models included leukoaraiosis
as the independent variable of interest, along with the following covariates: age, sex, handed-
ness, education, stroke type (ischemic/hemorrhagic), lesion extent, and lesion extent in lan-
guage areas. The last two of these covariates were modeled as polynomials of degree 2 since
their effects are likely to be nonlinear.
The model of aphasia recovery included two additional covariates known to be predictive
of recovery: initial QAB score and days post stroke of the final evaluation, both modeled as
polynomials of degree 2 due to expected nonlinear effects. The dependent variable was trans-
formed with an inverse hyperbolic sine function (λ = 4) to reduce heteroscedasticity, since
lower starting scores entail more room for improvement, so there was more variance when
starting scores were lower. The model of final QAB scores also included days post stroke of
the final evaluation, as a polynomial of degree 2.
Statistical significance of single terms was assessed using t statistics, while statistical signif-
icance of sets of related terms was assessed with likelihood ratio tests comparing full and
reduced models. One-tailed p values are reported for measures of brain health (leukoaraiosis,
age) because there were directional hypotheses associated with these measures, while two-
tailed p values are reported for all other variables.
RESULTS
Leukoaraiosis
Evidence of at least some leukoaraiosis was present on 240 out of 267 (90%) FLAIR images.
The mean leukoaraiosis rating was 2.6 points (SD = 1.7, range = 0, 6), on the Fazekas scale.
The distribution of leukoaraiosis ratings is shown in Figure 2B. As expected, leukoaraiosis was
highly correlated with age, r = 0.50, p < 0.0001 (Figure 2C). A linear model of leukoaraiosis as
a function of demographic and medical history variables and stroke type showed that there
was a medium sized effect of age, f 2 = 0.271, β = 0.058 Fazekas points per year, 95% CI =
0.044, 0.072, p < 0.0001; a small effect of hypertension, f 2 = 0.034, β = 0.696 Fazekas points,
95% CI = 0.231, 1.162, p = 0.0035, and a small effect of hemorrhagic stroke, f 2 = 0.036, β =
0.848 Fazekas points, 95% CI = 0.297, 1.398, p = 0.0027. No other variables were significant
predictors of leukoaraiosis.
Aphasia
At the acute time point, among individuals with and without aphasia, the mean initial
QAB overall score was 6.8 (SD = 3.1, range = 0, 10). In the 84 patients with aphasia
who were included in the longitudinal analyses, the mean initial QAB overall score was
Neurobiology of Language
7
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
d
o
i
/
l
/
.
/
1
0
1
1
6
2
n
o
_
a
_
0
0
1
1
5
2
1
5
5
7
1
1
n
o
_
a
_
0
0
1
1
5
p
d
.
/
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Leukoaraiosis and recovery from aphasia
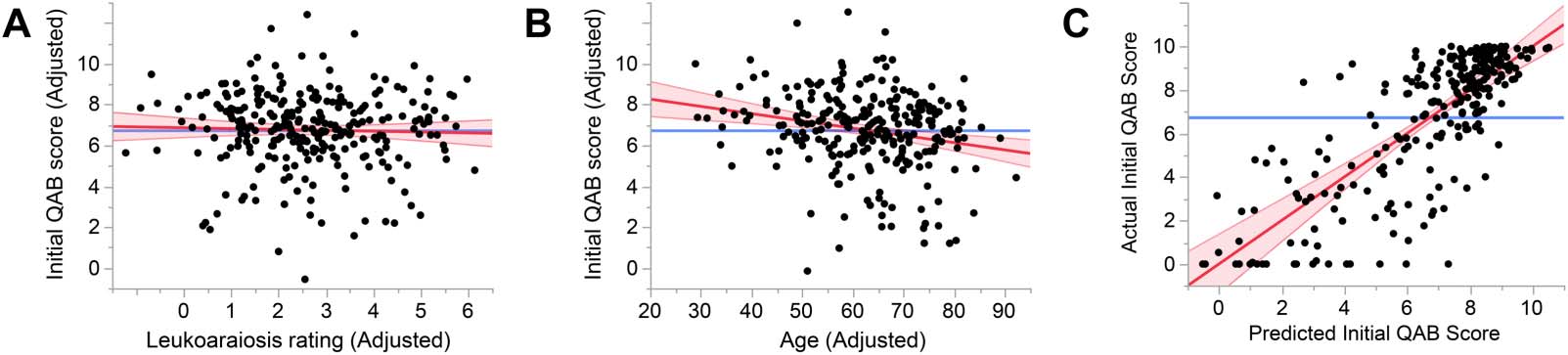
Figure 3. Predictors of initial aphasia severity. (A) Added variable plot (partial regression residual leverage plot) showing the lack of relation-
ship between adjusted leukoaraiosis rating and adjusted initial QAB score. Note that each variable was adjusted by accounting for the effects
of other variables in the model, which is why adjusted scores could fall outside the actual range of the scales. (B) Added variable plot showing
a significant negative relationship between age and initial QAB score. (C) Whole model plot showing the predictive power of the model.
QAB = Quick Aphasia Battery.
5.1 (SD = 0.3, range = 0, 9.75). These patients recovered by a mean of 2.9 points (SD = 2.2,
range 0, 9.1), obtaining a mean longer term QAB overall score of 8.0 (SD = 2.1, range =
0.7, 9.9).
Effect of Leukoaraiosis on Initial Aphasia Severity
There was no effect of leukoaraiosis on initial aphasia severity, n = 267, Cohen’s f 2 = 0.0006,
β = −0.03 QAB points per Fazekas scale point, 95% CI = −0.19, 0.13, p = 0.35 (Figure 3A).
There was a small negative effect of age, f 2 = 0.045, β = −0.033 QAB points per year, 95%
CI = −0.052, −0.014, p = 0.0004 (Figure 3B). The full model explained 63.8% of the var-
iance, with significant effects (besides age) of total lesion extent, damage to the language
network, stroke type, and education (Figure 3C; see Supplemental Table 1 in the Supporting
Information, available at https://doi.org/10.1162/nol_a_00115, for details). When periventri-
cular and deep white matter involvement were modeled separately, neither were associated
with initial aphasia severity, periventricular: β = −0.035, p = 0.41; deep: β = −0.069, p =
0.32. In the subset of 234 patients with ischemic stroke, there was no effect of leukoaraiosis
on initial aphasia severity, β = −0.078, p = 0.18.
Because of the observed correlation between leukoaraiosis and age, we also ran a
follow-up model in which age was omitted. In this model, there was a small negative effect
of leukoaraiosis on initial aphasia severity, f 2 = 0.02, β = −0.17 QAB points per Fazekas
scale point, 95% CI = −0.31, −0.03, p = 0.0088. However, the fact that leukoaraiosis had
no effect in the full model indicates that this effect is secondary to the correlation between
leukoaraiosis and age.
Effect of Leukoaraiosis on Recovery From Aphasia
There was no effect of leukoaraiosis on recovery from aphasia (the extent of improvement
in QAB overall score from the acute time point to the longer-term time point), n = 84,
Cohen’s f 2 = 0.03, β = 0.016 transformed QAB points per Fazekas scale point, that is,
numerically greater recovery in patients with worse leukoaraiosis, 95% CI = −0.006,
0.037, p = 0.93 (Figure 4A). There was a small negative effect of age on recovery, f 2 =
0.11, β = −0.0035 transformed QAB points per year, 95% CI = −0.0060, −0.0009, p =
0.0039 (Figure 4B). The full model explained 75.0% of the variance, with significant effects
(besides age) of initial aphasia severity, total lesion extent, damage to the language network,
and handedness (Figure 4C; see Supplemental Table 2 for details).
Neurobiology of Language
8
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
d
o
i
/
l
/
/
.
1
0
1
1
6
2
n
o
_
a
_
0
0
1
1
5
2
1
5
5
7
1
1
n
o
_
a
_
0
0
1
1
5
p
d
.
/
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Leukoaraiosis and recovery from aphasia
Figure 4. Predictors of recovery from aphasia. (A) Added variable plot (partial regression residual leverage plot) showing the lack of relation-
ship between adjusted leukoaraiosis rating and adjusted transformed recovery. (B) Added variable plot showing a significant negative relation-
ship between age and transformed recovery. (C) Whole model plot showing the predictive power of the model.
When periventricular and deep white matter involvement were modeled separately, neither
were associated with recovery from aphasia, periventricular: β = 0.043, p = 0.99; deep: β =
−0.0075, p = 0.65, nor was leukoaraiosis associated with recovery in the subset of 73 patients
with ischemic stroke, β = 0.020, p = 0.94. There was no effect of leukoaraiosis in a follow-up
model with age omitted.
Effect of Leukoaraiosis on Longer-Term Aphasia Outcome
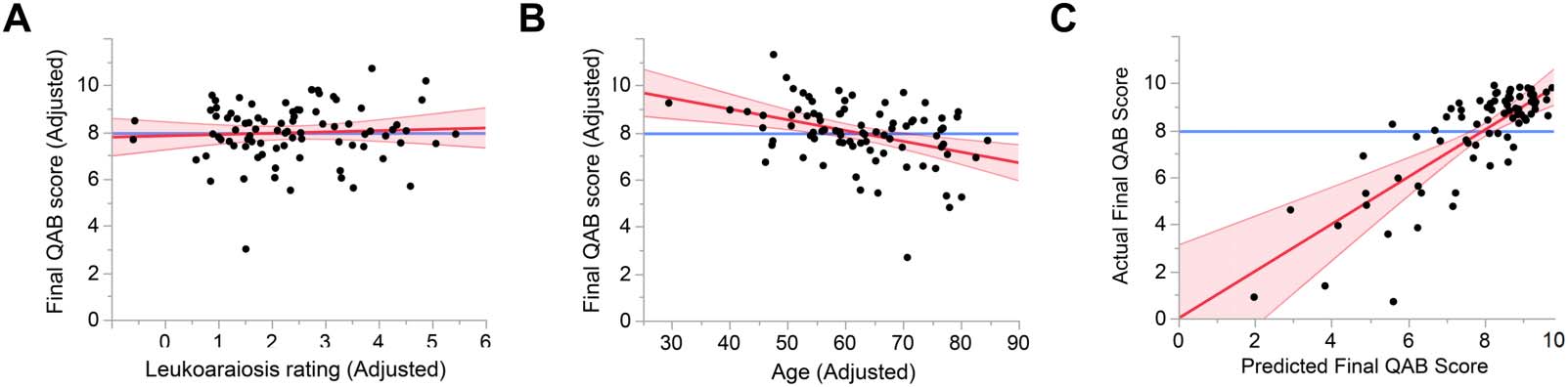
There was no effect of leukoaraiosis on longer-term aphasia outcome (QAB overall score at
∼3 months or later), n = 84, Cohen’s f 2 = 0.004, β = 0.062 QAB points per Fazekas scale point,
that is, numerically better outcomes in patients with worse leukoaraiosis, 95% CI = −0.166,
0.290, p = 0.70 (Figure 5A). There was a medium-sized negative effect of age on final aphasia
outcome, f 2 = 0.17, β = −0.045 QAB points per year, 95% CI = −0.071, −0.019, p = 0.0005
(Figure 5B). The full model explained 66.1% of the variance, with significant effects (besides
age) of total lesion extent and damage to the language network (Figure 5C; see Supplemental
Table 3 for details).
When periventricular and deep white matter involvement were modeled separately, neither
were associated with longer term aphasia outcome, periventricular: β = 0.147, p = 0.76; deep:
β = 0.049, p = 0.40, nor was leukoaraiosis associated with outcome in the subset of 73 patients
with ischemic stroke, β = 0.075, p = 0.74. There was no effect of leukoaraiosis in a follow-up
model with age omitted.
Figure 5. Predictors of longer-term aphasia outcome. (A) Added variable plot (partial regression residual leverage plot) showing the lack of
relationship between adjusted leukoaraiosis ratings and adjusted final QAB score. (B) Added variable plot showing a significant negative
relationship between age and adjusted final QAB score. (C) Whole model plot showing the predictive power of the model. QAB = Quick
Aphasia Battery.
Neurobiology of Language
9
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
d
o
i
/
l
.
/
/
1
0
1
1
6
2
n
o
_
a
_
0
0
1
1
5
2
1
5
5
7
1
1
n
o
_
a
_
0
0
1
1
5
p
d
.
/
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Leukoaraiosis and recovery from aphasia
DISCUSSION
In this study, we evaluated the impact of leukoaraiosis on three outcomes of interest: initial aphasia
severity, aphasia recovery, and longer-term aphasia severity. We observed no significant associa-
tions between baseline leukoaraiosis severity, as measured by the Fazekas visual rating scale, and
any of these outcome measures. Strengths of our study include its prospective and longitudinal
design, representative sample of ischemic and hemorrhagic stroke patients, reliable quantification
of leukoaraiosis, and careful quantification of aphasia using a validated battery. The confidence
intervals around the estimates of the effect of leukoaraiosis on these three outcome measures were
quite narrow, indicating that any effect of leukoaraiosis is at most modest. Moreover, our study was
sufficiently well powered to demonstrate robust negative effects of age on aphasia outcomes.
There is strong and unequivocal evidence that leukoaraiosis is associated with cognitive
deficits and cognitive decline (Au et al., 2006; de Groot et al., 2000). Why then, would leu-
koaraiosis not show an association with language deficits or their resolution? One possible
explanation is that language is anatomically and functionally distinct from other aspects of
cognition (Blank et al., 2014; Fedorenko et al., 2012; Fedorenko & Varley, 2016; Woolgar
et al., 2018). The anatomical distribution of leukoaraiosis is relatively conserved across indi-
viduals: primarily periventricular and particularly concentrated around the frontal and occip-
ital horns of the ventricles. This characteristic distribution of cSVD is largely medial to critical
language tracts, which may explain the lack of association between leukoaraiosis and aphasia
recovery that we observed. Figure 6 shows the location of the superior longitudinal fasciculus,
the most dorsal of the white matter pathways that are critical for language (Wilson et al., 2011),
in relation to the distribution of white matter hyperintensities in an individual with severe peri-
ventricular and deep white matter leukoaraiosis. This illustrates how even severe leukoaraiosis
impinges only minimally on the language network.
However, this potential explanation for our null findings should be considered tentative,
because cSVD has been shown to have network effects well beyond its visible markers (leukoar-
aiosis, microbleeds, enlarged perivascular spaces, etc.; ter Telgte et al., 2018; Wilmskoetter et al.,
2019). These more global effects may include disruption of white matter pathways, abnormal
functional connectivity, and atrophy. Therefore, the fact that leukoaraiosis is largely localized
medial to the language network does not imply that cSVD spares the language network entirely.
Several previous studies have investigated the relationship between leukoaraiosis and
aphasia. The largest and most comprehensive of these reported that, in contrast to our findings,
severity of leukoaraiosis was negatively associated with aphasia outcome in 106 chronic
stroke patients (Johnson et al., 2022; see also two previous smaller studies from the same
group: Basilakos et al., 2019; Wilmskoetter et al., 2019). We calculated the effect size of leu-
koaraiosis based on the data set provided (Johnson et al., 2022) and found that the effect size
of the association between leukoaraiosis and aphasia was small, Cohen’s f 2 = 0.06, β = −2.8 WAB
points per Fazekas scale point, 95% CI = −5.1, −0.5. Note that the WAB is on a 100-point scale
in contrast to the 10-point scale of the QAB in the present study.
Figure 6. The superior longitudinal fasciculus (from the JHU atlas, Hua et al., 2008) overlaid on a FLAIR image from an individual with severe
leukoaraiosis. FLAIR = fluid attenuated inversion recovery.
Neurobiology of Language
10
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
d
o
i
/
l
/
/
.
1
0
1
1
6
2
n
o
_
a
_
0
0
1
1
5
2
1
5
5
7
1
1
n
o
_
a
_
0
0
1
1
5
p
d
.
/
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Leukoaraiosis and recovery from aphasia
One potentially important difference between this study and ours is that in Johnson et al.
(2022), patients were recruited because they expressed an interest in taking part in aphasia treat-
ment studies, and as such they generally had significant chronic aphasia. The mean WAB aphasia
quotient was 62.2 and the mean lesion extent was 121 cm3, indicating that this cohort was con-
siderably more severe than our longitudinal cohort, who had recovered to a mean QAB overall
score of 8.0 by our final timepoint, and had a mean lesion extent of 69 cm3. It is possible that
leukoaraiosis is more of a predictor of recovery in patients with the kind of substantial damage to
core language regions that leads to chronic moderate to severe aphasia, but less of a factor for the
majority of left hemisphere stroke patients, who tend to recover quite well (Wilson et al., 2023).
Another possibility is that leukoaraiosis modulates treated recovery but not spontaneous
recovery. This would be plausible because many forms of aphasia treatment draw on cognitive,
attentional, and executive processes that are distinct from the language network, and these are
the kinds of cognitive processes that have been shown to be impacted by leukoaraiosis. The
patients in Johnson et al. (2022) had mostly received substantial aphasia treatment, and their
mean time post stroke was just over 3 years, so these patients had spent a longer period of time
in the recovery process. In contrast, our cohort of patients were a more representative sample of
left hemisphere stroke survivors, who had mostly received relatively low intensity speech-
language therapy, or none at all, so their recovery was largely spontaneous in nature.
Two other smaller studies have reported associations between leukoaraiosis and aphasia. In
42 patients who had presented with aphasia acutely after stroke, leukoaraiosis was associated
with naming and verbal fluency measures when patients were assessed later in the subacute or
chronic phase (Wright et al., 2018). Besides its small sample size, this study had several meth-
odological limitations including ceiling effects on the naming measure, dichotomization of
outcomes, and failure to include age as a covariate. In the other study, leukoaraiosis was asso-
ciated with an improvement on trained items in the context of aphasia treatment (Varkanitsa
et al., 2020). This positive finding may again reflect the impact of leukoaraiosis on the cogni-
tive abilities that underpin successful response to treatment, though it was not reported
whether leukoaraiosis had any impact on generalization to untrained items, or other measures
of aphasia severity. Finally, one previous study of the association between leukoaraiosis and
acute aphasia did not find any relationship (Flowers et al., 2017). This result is consistent with
our findings; however, this study had several limitations including binary diagnoses of aphasia
and a narrow range of leukoaraiosis scores for most of the patients.
Our study had several noteworthy limitations. First, although we had a large sample of
acute stroke patients (N = 267), our sample of patients with longer term speech-language
evaluations was smaller (n = 84). It remains possible that there is a small effect of leukoaraiosis
on recovery from aphasia that we did not detect in our sample. Furthermore, we did not study
patients who were missed in the hospital (e.g., due to rapid discharge), who declined consent,
or for whom FLAIR imaging was not acquired. Second, the Fazekas scale is a subjective visual
rating scale. While this scale is widely used clinically and has high inter-rater reliability, future
work would benefit from a volumetric assessment of leukoaraiosis. Third, we focused only on
leukoaraiosis and did not investigate other potential measures of brain health, such as atrophy,
microhemorrhages, or lacunar strokes.
Despite these limitations, our study demonstrates that leukoaraiosis likely is not a major
contributor to language outcomes after stroke, either acutely or throughout the first year, dur-
ing which the majority of behavioral gains take place. The major determinants of aphasia after
stroke are lesion location and extent (Wilson et al., 2023). Age has a modest negative effect on
outcomes, though what aspect(s) of aging are responsible for this effect remain unknown.
Neurobiology of Language
11
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
d
o
i
/
l
/
/
.
1
0
1
1
6
2
n
o
_
a
_
0
0
1
1
5
2
1
5
5
7
1
1
n
o
_
a
_
0
0
1
1
5
p
d
/
.
l
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Leukoaraiosis and recovery from aphasia
Despite our negative findings for leukoaraiosis in this study, it remains plausible that the health
of surviving brain regions is a contributing factor to unexplained variance in aphasia recovery.
Further research is needed to discover whether there may be other imaging biomarkers that
may capture the variability of surviving brain regions in their potential for neuroplasticity.
ACKNOWLEDGMENTS
The authors thank Annie Burchfield, Wayneho Kam, Howard Kirshner, Maysaa Rahman,
Emma Willey, Melodie Yen, two anonymous reviewers, and the many stroke survivors, care-
givers, and clinicians who helped make the study possible.
FUNDING INFORMATION
Stephen M. Wilson, National Institute on Deafness and Other Communication Disorders
(https://dx.doi.org/10.13039/100000055), Award ID: R01 DC013270.
AUTHOR CONTRIBUTIONS
Alexandra C. Brito: Conceptualization; Investigation; Formal analysis; Visualization; Writing –
original draft; Writing – review & editing. Deborah F. Levy: Investigation; Writing – review &
editing. Sarah M. Schneck: Investigation; Writing – review & editing. Jillian L. Entrup: Inves-
tigation; Writing – review & editing. Caitlin F. Onuscheck: Investigation; Writing – review &
editing. Marianne Casilio: Investigation; Writing – review & editing. Michael de Riesthal:
Supervision; Writing – review & editing. L. Taylor Davis: Investigation; Supervision; Writing –
review & editing. Stephen M. Wilson: Conceptualization; Formal analysis; Funding acquisition;
Methodology; Supervision; Writing – original draft; Writing – review & editing.
DATA AVAILABILITY STATEMENT
The data and code for the key analyses described are available at: https://doi.org/10.17605
/OSF.IO/D45CF.
REFERENCES
Arsava, E. M., Rahman, R., Rosand, J., Lu, J., Smith, E. E., Rost,
N. S., Singhal, A. B., Lev, M. H., Furie, K. L., Koroshetz, W. J.,
Sorensen, A. G., & Ay, H. (2009). Severity of leukoaraiosis corre-
lates with clinical outcome after ischemic stroke. Neurology,
7 2 ( 1 6 ) , 1 4 0 3 – 1 4 1 0 . h t t p s : / / d o i . o r g / 1 0 . 1 2 1 2 / W N L
.0b013e3181a18823, PubMed: 19380699
Au, R., Massaro, J. M., Wolf, P. A., Young, M. E., Beiser, A., Seshadri,
S., D’Agostino, R. B., & DeCarli, C. (2006). Association of white
matter hyperintensity volume with decreased cognitive function-
ing: The Framingham Heart Study. Archives of Neurology, 63(2),
246–250. https://doi.org/10.1001/archneur.63.2.246, PubMed:
16476813
Baezner, H., Blahak, C., Poggesi, A., Pantoni, L., Inzitari, D., Chabriat,
H., Erkinjuntti, T., Fazekas, F., Ferro, J. M., Langhorne, P., O’Brien,
J., Scheltens, P., Visser, M. C., Wahlund, L. O., Waldemar,
G., Wallin, A., Hennerici, M. G., & LADIS Study Group.
(2008). Association of gait and balance disorders with
age-related white matter changes: The LADIS study. Neurology,
70(12), 935–942. https://doi.org/10.1212/01.wnl.0000305959
.46197.e6, PubMed: 18347315
Basilakos, A., Stark, B. C., Johnson, L., Rorden, C., Yourganov, G.,
Bonilha, L., & Fridriksson, J. (2019). Leukoaraiosis is associated
with a decline in language abilities in chronic aphasia.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Neurorehabilitation and Neural Repair, 33(9), 718–729. https://
doi.org/10.1177/1545968319862561, PubMed: 31315507
Basso, A. (1992). Prognostic factors in aphasia. Aphasiology, 6(4),
337–348. https://doi.org/10.1080/02687039208248605
Blank, I., Kanwisher, N., & Fedorenko, E. (2014). A functional dis-
sociation between language and multiple-demand systems
revealed in patterns of BOLD signal fluctuations. Journal of Neu-
rophysiology, 112(5), 1105–1118. https://doi.org/10.1152/jn
.00884.2013, PubMed: 24872535
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for
evaluating normed and standardized assessment instruments in
psychology. Psychological Assessment, 6(4), 284–290. https://
doi.org/10.1037/1040-3590.6.4.284
Debette, S., Beiser, A., DeCarli, C., Au, R., Himali, J. J., Kelly-Hayes,
M., Romero, J. R., Kase, C. S., Wolf, P. A., & Seshadri, S. (2010).
Association of MRI markers of vascular brain injury with incident
stroke, mild cognitive impairment, dementia, and mortality: The
Framingham Offspring Study. Stroke, 41(4), 600–606. https://doi
.org/10.1161/STROKEAHA.109.570044, PubMed: 20167919
Debette, S., & Markus, H. S. (2010). The clinical importance of
white matter hyperintensities on brain magnetic resonance imag-
ing: Systematic review and meta-analysis. BMJ, 341, Article
c3666. https://doi.org/10.1136/bmj.c3666, PubMed: 20660506
Neurobiology of Language
12
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
n
o
/
l
/
l
a
r
t
i
c
e
-
p
d
f
/
d
o
i
/
l
.
/
/
1
0
1
1
6
2
n
o
_
a
_
0
0
1
1
5
2
1
5
5
7
1
1
n
o
_
a
_
0
0
1
1
5
p
d
/
.
l
Leukoaraiosis and recovery from aphasia
de Groot, J. C., de Leeuw, F. E., Oudkerk, M., van Gijn, J., Hofman,
A., Jolles, J., & Breteler, M. M. (2000). Cerebral white matter
lesions and cognitive function: The Rotterdam Scan Study.
Annals of Neurology, 47(2), 145–151. https://doi.org/10.1002
/1531-8249(200002)47:2<145::AID-ANA3>3.0.CO;2-P,
PubMed: 10665484
de Leeuw, F. E., de Groot, J. C., Achten, E., Oudkerk, M., Ramos,
l. M., Heijboer, R., Hofman, A., Jolles, J., van Gijn, J., & Breteler,
M. M. (2001). Prevalence of cerebral white matter lesions in
elderly people: A population based magnetic resonance imaging
study. The Rotterdam Scan Study. Journal of Neurology, Neuro-
surgery, and Psychiatry, 70(1), 9–14. https://doi.org/10.1136
/jnnp.70.1.9, PubMed: 11118240
Fazekas, F., Chawluk, J., Alavi, A., Hurtig, H., & Zimmerman, R.
(1987). MR signal abnormalities at 1.5 T in Alzheimer’s dementia
and normal aging. American Journal of Roentgenology, 149(2),
351–356. https://doi.org/10.2214/ajr.149.2.351, PubMed:
3496763
Fedorenko, E., Duncan, J., & Kanwisher, N. (2012). Language-
selective and domain-general regions lie side by side within
Broca’s area. Current Biology, 22(21), 2059–2062. https://doi
.org/10.1016/j.cub.2012.09.011, PubMed: 23063434
Fedorenko, E., & Varley, R. (2016). Language and thought are not
the same thing: Evidence from neuroimaging and neurological
patients. Annals of the New York Academy of Sciences,
1369(1), 132–153. https://doi.org/10.1111/nyas.13046,
PubMed: 27096882
Flowers, H. L., AlHarbi, M. A., Mikulis, D., Silver, F. L., Rochon, E.,
Streiner, D., & Martino, R. (2017). MRI-based neuroanatomical
predictors of dysphagia, dysarthria, and aphasia in patients with
first acute ischemic stroke. Cerebrovascular Diseases Extra, 7(1),
21–34. https://doi.org/10.1159/000457810, PubMed: 28208139
Hartwigsen, G., & Saur, D. (2019). Neuroimaging of stroke recov-
ery from aphasia – Insights into plasticity of the human language
rete. NeuroImage, 190, 14–31. https://doi.org/10.1016/j
.neuroimage.2017.11.056, PubMed: 29175498
Hollocks, M. J., Lawrence, UN. J., Brookes, R. L., Barrick, T. R., Morris,
R. G., Husain, M., & Markus, H. S. (2015). Differential relationships
between apathy and depression with white matter microstruc-
tural changes and functional outcomes. Brain, 138(Pt. 12),
3803–3815. https://doi.org/10.1093/ brain/awv304, PubMed:
26490330
Hua, K., Zhang, J., Wakana, S., Jiang, H., Li, X., Reich, D. S., Calabresi,
P. A., Pekar, J. J., van Zijl, P. C. M, & Mori, S. (2008). Tract
probability maps in stereotaxic spaces: Analyses of white matter
anatomy and tract-specific quantification. NeuroImage, 39(1),
336–347. https://doi.org/10.1016/j.neuroimage.2007.07.053,
PubMed: 17931890
Johnson, L., Nemati, S., Bonilha, L., Rorden, C., Busby, N., Basilakos,
A., Newman-Norlund, R., Hillis, UN. E., Hickok, G., & Fridriksson,
J. (2022). Predictors beyond the lesion: Health and demographic
factors associated with aphasia severity. Cortex, 154, 375–389.
https://doi.org/10.1016/j.cortex.2022.06.013, PubMed:
35926368
Kertesz, A., & McCabe, P. (1977). Recovery patterns and prognosis
in aphasia. Brain, 100(1), 1–18. https://doi.org/10.1093/ brain
/100.1.1, PubMed: 861709
Kissela, B., Lindsell, C. J., Kleindorfer, D., Alwell, K., Moomaw,
C. J., Woo, D., Flaherty, M. L., Air, E., Broderick, J., & Tsevat, J.
(2009). Clinical prediction of functional outcome after ischemic
stroke: The surprising importance of periventricular white matter
disease and race. Stroke, 40(2), 530–536. https://doi.org/10.1161
/STROKEAHA.108.521906, PubMed: 19109548
Longstreth, W. T., Jr., Manolio, T. A., Arnold, A., Burke, G. L.,
Bryan, N., Jungreis, C. A., Enright, P. L., O’Leary, D., & Fried,
l. (1996). Clinical correlates of white matter findings on cranial
magnetic resonance imaging of 3301 elderly people. Stroke,
27(8), 1274–1282. https://doi.org/10.1161/01.STR.27.8.1274,
PubMed: 8711786
Pantoni, l. (2010). Cerebral small vessel disease: From pathogene-
sis and clinical characteristics to therapeutic challenges. IL
Lancet Neurology, 9(7), 689–701. https://doi.org/10.1016/S1474
-4422(10)70104-6, PubMed: 20610345
Pantoni, L., Simoni, M., Pracucci, G., Schmidt, R., Barkhof, F., &
Inzitari, D. (2002). Visual rating scales for age-related white mat-
ter changes (leukoaraiosis): Can the heterogeneity be reduced?
Stroke, 33(12), 2827–2833. https://doi.org/10.1161/01.STR
.0000038424.70926.5E, PubMed: 12468777
Pedersen, P. M., Jørgensen, H. S., Nakayama, H., Raaschou, H. O.,
& Olsen, T. S. (1995). Aphasia in acute stroke: Incidence, deter-
minants, and recovery. Annals of Neurology, 38(4), 659–666.
https://doi.org/10.1002/ana.410380416, PubMed: 7574464
Plowman, E., Hentz, B., & Ellis, C., Jr. (2012). Post-stroke aphasia
prognosis: A review of patient-related and stroke-related factors.
Journal of Evaluation in Clinical Practice, 18(3), 689–694. https://
doi.org/10.1111/j.1365-2753.2011.01650.x , PubMed:
21395923
Ryu, W.-S., Woo, S.-H., Schellingerhout, D., Jang, M. U., Park, K.-J.,
Hong, K.-S., Jeong, S.-W., Na, J.-Y., Cho, K.-H., Kim, J.-T., Kim,
B. J., Han, M.-K., Lee, J., Cha, J.-K., Kim, D.-H., Lee, S. J., Ko, Y.,
Cho, Y.-J., Lee, B.-C., … Kim, D.-E. (2017). Stroke outcomes are
worse with larger leukoaraiosis volumes. Brain, 140(1), 158–170.
https://doi.org/10.1093/brain/aww259, PubMed: 28008000
Swinburn, K., Porter, G., & Howard, D. (2004). Comprehensive
aphasia test. Psychology Press. https://doi.org/10.1037/t13733
-000
Teodorczuk, A., Firbank, M. J., Pantoni, L., Poggesi, A., Erkinjuntti,
T., Wallin, A., Wahlund, L.-O., Scheltens, P., Waldemar, G.,
Schrotter, G., Ferro, J. M., Chabriat, H., Bazner, H., Visser, M.,
Inzitari, D., O’Brien, J. T., & LADIS Group. (2010). Relationship
between baseline white-matter changes and development of
late-life depressive symptoms: 3-year results from the LADIS
study. Psychological Medicine, 40(4), 603–610. https://doi.org
/10.1017/S0033291709990857, PubMed: 19671212
ter Telgte, A., van Leijsen, E. M. C., Wiegertjes, K., Klijn, C. J. M.,
Tuladhar, UN. M., & de Leeuw, F.-E. (2018). Cerebral small vessel
disease: From a focal to a global perspective. Nature Reviews
Neurology, 14(7), 387–398. https://doi.org/10.1038/s41582-018
-0014-sì, PubMed: 29802354
Varkanitsa, M., Peñaloza, C., Charidimou, A., Caplan, D., & Kiran,
S. (2020). White matter hyperintensities predict response to lan-
guage treatment in poststroke aphasia. Neurorehabilitation and
Neural Repair, 34(10), 945–953. https://doi.org/10.1177
/1545968320952809, PubMed: 32924765
Watila, M. M., & Balarabe, S. UN. (2015). Factors predicting
post-stroke aphasia recovery. Journal of the Neurological Sci-
enze, 352(1–2), 12–18. https://doi.org/10.1016/j.jns.2015.03
.020, PubMed: 25888529
Wilmskoetter, J., Marebwa, B., Basilakos, A., Fridriksson, J., Rorden,
C., Stark, B. C., Johnson, L., Hickok, G., Hillis, UN. E., & Bonilha,
l. (2019). Long-range fibre damage in small vessel brain disease
affects aphasia severity. Brain, 142(10), 3190–3201. https://doi
.org/10.1093/brain/awz251, PubMed: 31501862
Wilson, S. M., Entrup, J. L., Schneck, S. M., Onuscheck, C. F., Levy,
D. F., Rahman, M., Willey, E., Casilio, M., Yen, M., Brito, A.,
Kam, W., Davis, l. T., de Riesthal, M., & Kirshner, H. S.
Neurobiology of Language
13
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
l
.
/
/
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
/
.
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Leukoaraiosis and recovery from aphasia
(2023). Recovery from aphasia in the first year after stroke. Brain,
146(3), 1021–1039. https://doi.org/10.1093/ brain/awac129,
PubMed: 35388420
Wilson, S. M., Eriksson, D. K., Brandt, T. H., Schneck, S. M., Lucanie,
J. M., Burchfield, UN. S., Charney, S., Quillen, IO. A., de Riesthal,
M., Kirshner, H. S., Beeson, P. M., Ritter, L., & Kidwell, C. S.
(2019). Patterns of recovery from aphasia in the first 2 weeks after
stroke. Journal of Speech, Language, and Hearing Research,
62(3), 723–732. https://doi.org/10.1044/2018_JSLHR-L-18
-0254, PubMed: 30950735
Wilson, S. M., Eriksson, D. K., Schneck, S. M., & Lucanie, J. M.
(2018). A quick aphasia battery for efficient, reliable, and multi-
dimensional assessment of language function. PLOS ONE, 13(2),
Article e0192773. https://doi.org/10.1371/journal.pone.0192773,
PubMed: 29425241
Wilson, S. M., Galantucci, S., Tartaglia, M. C., Rising, K., Patterson,
D. K., Henry, M. L., Ogar, J. M., DeLeon, J., Mugnaio, B. L., &
Gorno-Tempini, M. l. (2011). Syntactic processing depends on
dorsal language tracts. Neuron, 72(2), 397–403. https://doi.org
/10.1016/j.neuron.2011.09.014, PubMed: 22017996
Wilson, S. M., & Schneck, S. M. (2021). Neuroplasticity in
post-stroke aphasia: A systematic review and meta-analysis of
functional imaging studies of reorganization of language pro-
cessazione. Neurobiology of Language, 2(1), 22–82. https://doi.org
/10.1162/nol_a_00025, PubMed: 33884373
Wilson, S. M., Yen, M., & Eriksson, D. K. (2018). An adaptive
semantic matching paradigm for reliable and valid language
mapping in individuals with aphasia. Human Brain Mapping,
39(8), 3285–3307. https://doi.org/10.1002/ hbm.24077,
PubMed: 29665223
Woolgar, A., Duncan, J., Manes, F., & Fedorenko, E. (2018). IL
multiple-demand system but not the language system supports
fluid intelligence. Nature Human Behaviour, 2(3), 200–204.
https://doi.org/10.1038/s41562-017-0282-3, PubMed:
31620646
Wright, A., Tippett, D., Saxena, S., Sebastian, R., Breining, B., Faria,
A., & Hillis, UN. E. (2018). Leukoaraiosis is independently associated
with naming outcome in poststroke aphasia. Neurology, 91(6),
e526–e532. https://doi.org/10.1212/ WNL.0000000000005945,
PubMed: 29980639
Yen, M., DeMarco, UN. T., & Wilson, S. M. (2019). Adaptive para-
digms for mapping phonological regions in individual partici-
pants. NeuroImage, 189, 368–379. https://doi.org/10.1016/j
.neuroimage.2019.01.040, PubMed: 30665008
l
D
o
w
N
o
UN
D
e
D
F
R
o
M
H
T
T
P
:
/
/
D
io
R
e
C
T
.
M
io
T
.
e
D
tu
N
o
/
l
/
l
UN
R
T
io
C
e
–
P
D
F
/
D
o
io
/
l
.
/
/
1
0
1
1
6
2
N
o
_
UN
_
0
0
1
1
5
2
1
5
5
7
1
1
N
o
_
UN
_
0
0
1
1
5
P
D
/
.
l
F
B
sì
G
tu
e
S
T
T
o
N
0
7
S
e
P
e
M
B
e
R
2
0
2
3
Neurobiology of Language
14