INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 52
Seth Berkley
Ending an Epidemic
The International AIDS Vaccine Initiative
Pioneers a Public-Private Partnership
Since Acquired Immunodeficiency Syndrome (AIDS) was identified in 1981, it has killed more
than 25 million people and more than 40 million are infected today with HIV, the virus that
causes AIDS. The spread has been worldwide but it is the developing world that is now bear-
ing the brunt of the epidemic with 95% of the new infections. Despite increasing efforts at pre-
vention and treatment, the epidemic, continues to accelerate. This year, according to UNAIDS,
has seen the largest number of deaths to date, más que 3 millón, with more than 5 millón
new infections. Con 14,000 new infections a day, HIV is already reversing decades of progress
in these developing countries and has the potential to be even more catastrophic. Only a vac-
cine has any hope of ending the AIDS epidemic, yet through the mid-1990s AIDS vaccine work
was limited on the world’s richer nations, and even this work had slowed to a standstill.
En 1996 I founded the International AIDS Vaccine Initiative (IAVI), a public-private part-
nership to advance the development of HIV vaccines for use globally, and particularly in the
areas most affected by HIV and AIDS. IAVI faced great skepticism that a non profit could
advance vaccine research and development. Yet only four years later, in August 2000, British
physician and parliamentarian Evan Harris became the first person to be vaccinated with an
HIV vaccine designed for Africa, using strains of the virus circulating in that region. En 2001,
trials of this product began in Kenya, the first time an AIDS vaccine was tested in that coun-
intentar. The vaccine turned out to be ineffective—but IAVI’s model of working with academia,
gobiernos, and companies to speed product development and ensure an international focus
was clearly effective.
Today IAVI, a fully integrated vaccine development effort managed by experienced indus-
trial project managers, is the second largest global program in HIV vaccine research and devel-
opment, with more than forty active R&D relationships. IAVI has successfully translated inno-
vative technologies into seven novel vaccine candidates that have entered human trials in the
last six years, and has conducted clinical studies at 15 trial sites located in 11 countries. El
the International AIDS Vaccine Initiative (ver
Seth Berkley, President and founder of
tional health. Prior to founding the initiative, Dr. Berkley was the Associate Director of the Health
Sciences Division at The Rockefeller Foundation. Dr. Berkley is also an adjunct Professor of Public
Health at Columbia University and an adjunct Professor of Medicine at Brown University.
© 2006 Tagore LLC
innovaciones / invierno 2006
52
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023
INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 53
Ending an Epidemic
organization’s 160 staff members work out of four regional offices in Amsterdam, New Delhi,
Nairobi, and New York, and are active in 23 countries. IAVI has contributed not only to
advancing the required sci-
ence and developing novel
candidate HIV vaccines,
but also to changing the
terms of the public discus-
sion regarding the develop-
mento,
financiación
and delivery of a preventa-
tive HIV/AIDS vaccine on
a global scale.
Only a vaccine has any hope of ending
the AIDS epidemic. Yet through the mid-
1990s AIDS vaccine work focused on the
world’s richer nations, and even this
work had slowed to a standstill.
pruebas,
This paper discusses
IAVI’s approach to AIDS
vaccine development. El
first section briefly discusses IAVI’s origins and mission. The second section, on how IAVI
operates, describes many of the innovative decisions that IAVI made at the outset to bridge the
gap between private and public endeavors and to fulfill its international mission. A final sec-
tion assesses IAVI’s impact, both on AIDS vaccine research and as a model of public-private
collaboration to solve pressing global problems.
IAVI’S ORIGINS
My strong interest in the international HIV epidemic began in the late 1980s when I worked
in Uganda as the epidemiologist for the Ministry of Health, helping efforts to rebuild the
Ugandan immunization and public health system. Uganda was the first country in Africa
where the disease was recognized as “AIDS,” and the global health community was slowly
drawing parallels between the Ugandan epidemic and the one decimating the homosexual
population in the U.S.. The Ministry undertook some simple studies aimed at assessing the
epidemiology of HIV, which culminated in a national sero-survey. The results were staggering:
17 percent of the adult population in Kampala and 10.6 percent in the country as a whole were
infected with HIV. Soon similar data from other countries confirmed that AIDS had become
a global pandemic.
After more than two years of working with the Uganda Ministry of Health I joined the
Rockefeller Foundation and soon was approached by a colleague in industry who was con-
cerned that research and development (R&D) on vaccines for AIDS was moribund. While I
was aware of the scientific challenges involved in developing a vaccine, I had believed, as did
otros, that everything possible was being done. While there was no debate about the imme-
diate imperatives of managing the existing infections and preventing further infections with
whatever means possible, public health leaders understood that an approach based entirely on
behavioral change and basic treatment would not, in the long run, end the epidemic or be sus-
tainable. It was apparent to all working in the field that a preventive vaccine was the best long-
term tool to blunt and ultimately end the epidemic. Public awareness and concern over the epi-
demic was rapidly growing and the economic environment for private sector vaccine R&D
innovaciones / invierno 2006
53
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023
INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 54
Seth Berkley
seemed promising—so what was the matter? Early work suggested that the economic incen-
tives should be adequate: a 1990 report by Shearson Lehman had estimated the global market
for an HIV/AIDS vaccine to be worth as much as $1.6 billion—a respectable number even when compared to the costs of developing and marketing a new vaccine or drug, then estimat- ed at $500 million or more.
To jump-start research and find more definitive answers, the Rockefeller Foundation con-
vened a series of meetings culminating in a gathering in Bellagio, Italia, in March 1994 with two
dozen AIDS researchers, vaccinol-
ogists, public health officials, y
representatives from philanthrop-
ic organizations. Their consensus
was that despite scientific clues
that the development of a preven-
tive AIDS vaccine appeared possi-
ble, it was unlikely that a vaccine
for use throughout the world
would be developed in an accept-
able time frame without a con-
certed effort from both the public
and private sectors.
[I]n March 1994,…two dozen AIDS
investigadores, vaccinologists, público
health officials, and representatives
from philanthropic organizations
[met in Bellagio, Italia]. Su
consensus was that… it was unlikely
that a vaccine for use throughout
the world would be developed and
made in an acceptable time frame
without a concerted effort involving
both the public and private sectors.
The Bellagio participants out-
lined three major impediments to
the development of an AIDS vac-
cine: ciencia, economics and poli-
tics.1 The scientific challenges of
vaccine research and development
have never been easy, and HIV has
particularly complex characteris-
tics. Most nonfatal pathogens
leave the human body immune. Not so for HIV; no one has ever recovered from the infection
and gained protective immunity. Compared with other viral infections, HIV provides few clues
to researchers regarding its vulnerabilities. Because it is a retrovirus, it inserts its genome into
that of the host, conferring persistent infection, and its high mutation rate during the replica-
tive cycle results in enormous variability. Early vaccine candidates were successful at produc-
ing neutralizing antibodies against laboratory-adapted strains of HIV, not against the wild-
tipo, circulating virus.2 Some HIV-infected subjects do produce broadly neutralizing antibod-
ies against wild-type HIV, but translating this knowledge to the lab and vaccine design contin-
ues to be an uphill scientific battle.
Basic economics raised a second set of obstacles. We found that the 1990 report by
Shearson Lehman exaggerated the market for AIDS vaccine in the developed world. Since HIV
was stigmatized and controversial, it was not clear if the vaccine would become mandated for
use in these high-profit markets—often a requirement for quick adoption of a vaccine. En
addition, careful consideration of the size of the population at highest risk of contracting
HIV/AIDS in resource-poor countries resulted in an estimate of the size of the early adapter
54
innovaciones / invierno 2006
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023
INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 55
Ending an Epidemic
market that was one-seventh of that estimated earlier.3 HIV/AIDS was disproportionately
afflicting people in the world’s poorest places; where the demand would be greatest, el
resources would be the most deficient.
Además, as a rule vaccines have been great for public health but not as great for business.
A treatment for a disease is administered repeatedly—sometimes for a lifetime—but a vaccine
is generally administered in one or a few doses. Por lo tanto, overall vaccine sales account for
solo 2-3% of pharmaceutical firms’ overall revenue. Vaccines are often purchased in bulk by
public entities, so the “market
price” of a vaccine is subject to
negotiations that take place only
after successful vaccine develop-
mento. Private companies engaged
in seeking a vaccine for global ill-
nesses take the risk that, if success-
lleno, they will be under enormous
pressure to make the vaccine avail-
able below cost to developing coun-
tries that are unwilling or unable to
offer compensating subsidies.
The Bellagio meeting participants
recommended a new global
initiative with the mandate to
ensure the development of safe,
effective, preventive HIV vaccines
for use throughout the world and,
En particular, for use in those
regions most affected by HIV and
AIDS. This became the basis for
IAVI’s mission statement.
Political obstacles also threat-
ened progress toward an AIDS vac-
cine. HIV/AIDS is deadly but con-
troversial.
In May 1994, muchos
countries were denying that their
citizens were at risk and considered
HIV as someone else’s problem.
Success
un
HIV/AIDS vaccine might earn acclaim for a private company, but the perception in 1994 era
that the firm could just as easily end up earning notoriety. Then a successful company would
be faced with an unenviable choice: to succumb to inevitable and intense public pressure to
make the vaccine available below cost in regions most severely affected by the epidemic or to
resist such demands and risk vilification. In a tragic irony…increasing public awareness and
activism regarding the epidemic was, at least along one dimension, blunting private efforts to
seek its permanent end.
developing
en
The Bellagio meeting participants recommended a new global initiative with the mandate
to ensure the development of safe, effective, preventive HIV vaccines for use throughout the
world and, En particular, for use in those regions most affected by HIV and AIDS. This became
the basis for IAVI’s mission statement.
A second group of scientists met in October 1994 to assess the prospects for the develop-
ment of a vaccine and the impediments to progress. All pertinent questions were on the table,
including whether the incentives problems could be overcome and whether the scientific chal-
lenge was fundamentally intractable. This group of leading scientists judged an AIDS vaccine
to be possible and they had strong ideas on how such an effort should be managed and
resourced to maximize success in the shortest time frame. They recommended that the initia-
innovaciones / invierno 2006
55
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023
INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 56
Seth Berkley
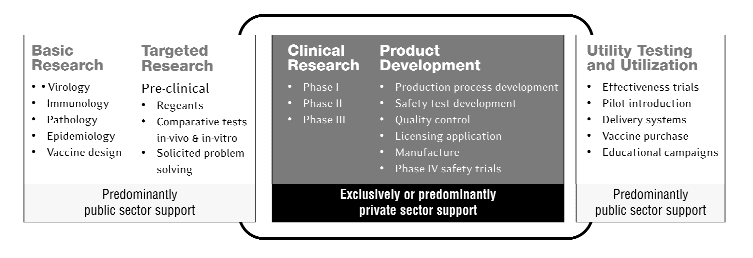
Cifra 1. Who pays for vaccine development and utilization?
Fuente: IAVI, “AIDS Vaccines for the World: Preparing Now to Assure Access.” July 9, 2000.
tive complement existing efforts by exploring previously neglected approaches; develop candi-
date vaccines from subtypes found in those areas most severely affected (an obvious starting
point that had not been attempted), and act to ensure that the appropriate incentives were in
place for industrial participation, and rapidly move products under consideration into clinical
ensayos. en agosto 1995, participants at a third Rockefeller-sponsored meeting in New York set
forth specifics for the creation of the IAVI. The new entity was incorporated in January 1996
as a non profit organization, based in New York but operating globally.
HOW IAVI OPERATES
In December 2004, Science magazine in its “Breakthrough of the Year feature” acknowledged
IAVI’s role as a leading pioneer in the public-private partnership movement. The magazine
characterized such partnerships as a revolution in public health that is fundamentally shifting
how medicines are developed and delivered to the world’s poorest people. This section discuss-
es the challenges facing public-private partnerships and how IAVI has sought to overcome
them and to serve as a truly international organization.
A New Kind of Public-Private Partnership
Over the past 30 years no new vaccines have been discovered and licensed without the active
involvement of private industry. The pharmaceutical testing and manufacturing process are so
complex that it is no longer feasible for academic scientists working outside of industry to cre-
ate a product, conduct toxicology tests, manage the manufacturing processes, set up and run
clinical trials, and move candidates through the regulatory process in a timely fashion. Todavía
industry did not have the incentives to develop an AIDS vaccine, so the responsibility for pub-
lic health and a significant share of the resources for action—including the academic basic
research critical to initiating the process—had to come from the public sector. So IAVI’ s first
challenge was to answer the questions: How do you bridge public and private? How do you
bring them together? How do you finance such an effort? Early experiments in the contracep-
tion area suggested how such public-private partnerships might be organized and formed the
basis of much of the early discussion.
56
innovaciones / invierno 2006
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023
INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 57
Ending an Epidemic
Hoy, public-private partnerships of various types are proliferating. By one count there
are currently 92 in the healthcare field alone.4 These include R&D partnerships like IAVI, columna-
laborations dedicated to the donation and distribution of existing products, ventures to
enhance community outreach or strengthen infrastructure for delivering treatment and pre-
vention. IAVI was the first biomedical product development public-private partnership
(PDPPP). More than a dozen other PDPPPs have since formed to tackle drugs and vaccines for
the other major infectious diseases of poverty.
Product development partnerships contend not only with the schism between public and
private institutions but also with the specific incentive, financiación, and management gaps that
separate investments in basic science from investments in development of viable, safe, y
effective products. Cifra 1 muestra
the normal process of vaccine
development and the roles of pub-
lic and private sectors, which must
be bridged effectively. The R&D
involved is always high-risk and
high-cost.5
IAVI was the first biomedical
product development public-
private partnership (PDPPP). Más
than a dozen other PDPPPs have
formed since to tackle drugs and
vaccines for the other major
infectious diseases of poverty.
Some fundamentals of IAVI’s
structure were general, and have
been shared by later PDPPPs.
Driven by a defined goal and man-
fecha, IAVI was established as an
independent legal body outside of
existing international and philan-
thropic entities. In all its develop-
ment activities IAVI would follow a
vaccine industry product management model: To start with a desired outcome and direct all
effort toward solving every problem that comes up in seeking to achieve that outcome (see text
box). Good investigator-led research means asking “what if ” questions that may lead to entire-
ly new lines of inquiry; the industry model does not permit this luxury. En cambio, multidiscipli-
nary project teams are held accountable for each vaccine project, keeping the teams focused on
the mission. Hoy, más que 75% of IAVI’s R&D staff have a private industry background.
IAVI also developed a portfolio approach to vaccine development; it reduce overall risk by hav-
ing different types of products in different stages of development.
We also made an early commitment to be an international organization. Based in New
York and led by an outspoken CEO from the U.S., we were aware that if our first government
funding came from the U.S. government we might be perceived as an “American organization.”
Therefore we built a broad and diverse financial and political base, and hired globally. The first
government to support us was that of the U.K.. Los países bajos, Irlanda, Canada, and finally
Estados Unidos. soon followed, and since then five more governments have joined. With these coun-
tries’ support and the generous support of private foundations, companies, and international
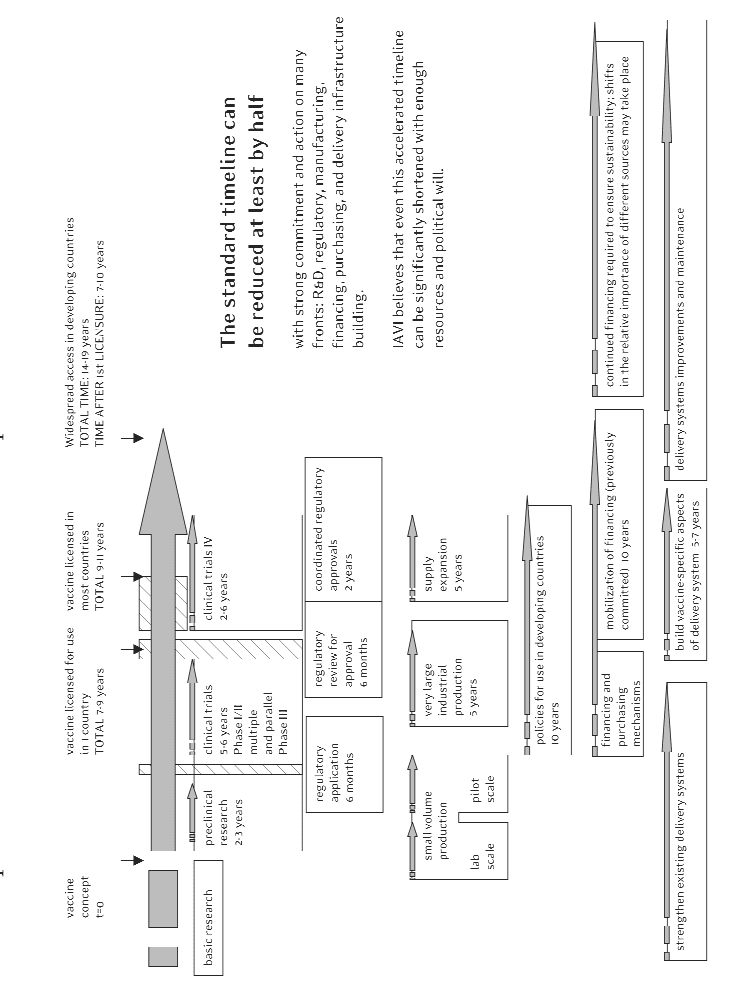
institutions, IAVI has raised more than $470M in new funds since its inception. Our global focus and geographically unrestricted funding has allowed us to search the world for the best technologies (Por ejemplo, we are now the largest funder of HIV vaccines in innovations / invierno 2006 57 Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023 INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 58 Seth Berkley Figure 2. Proposed timeline for AIDS vaccine development and access. Adapted from information in AIDS vaccines for the world: Preparing now to assure access (International AIDS Vaccine Initiative, 2000); and Scientific Blueprint 2000: Accelerating glob- al efforts in AIDS vaccine development (International AIDS Vaccine Initiative, 2000). 58 innovaciones / invierno 2006 Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023 INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 59 Ending an Epidemic Europe), partner with experts in different companies and academic institutions in different worldwide, and conduct studies where HIV/AIDS is spreading fastest. Comparative assess- ments also become an important function; we can test different products against each other as well as consider combining technologies that otherwise might not be brought together. As an international organization, IAVI can also focus on “vaccine preparedness” in the most affected developing countries: building clinical and political capabilities as well as assur- ing adequate skills in the media, civil society, and special interest groups. These are often coun- tries where the market may not create access, and this requires that we face the related chal- lenges of science and politics. This poses an organizational challenge as we bring together a not-for-profit capacity-building culture with an industrial product-development culture; sin embargo, it is our belief that the tensions lead to healthy innovations in how we work. IAVI has also stressed the importance of nurturing research capabilities within developing countries. While our basic approach has remained constant, the scope of our activities has changed considerably as we have come to better under- stand the field and the needs of our constituen- cíes, including those in the developing world. Initially, IAVI focused on advocacy for HIV vac- cines and on convincing the world that a not- for-profit PDPPP had a critical role to play in the biomedical advancement. We later moved into product development, but assumed that we would act as a “biotech incubator” that would accelerate only early development of products, which would then be quickly adopted by indus- intentar. We then shifted to become a fully integrated vaccine development effort with in-house expertise across the entire vaccine development chain (see figure 2). Más recientemente, through the development of consortium-style directed applied research, we have begun to tackle some of the fundamental challenges that still impede the vaccine development effort. We are currently establishing an industrial-style R&D laboratory to undertake early candidate process develop- mento, assay creation, and systematic studies and comparisons of candidates, delivery systems, and adjuvants6—activities that occur routinely in large vaccine companies but are not normal- ly available in the academic world. Addressing Needs and Building Capabilities in Resource-poor Countries In 1993, most of the work on AIDS vaccines was limited to battling AIDS in industrialized economies—where the market (in dollar terms), major scientific institutions, and companies were located. IAVI took the lead in addressing the full range of challenges in redirecting efforts to better reflect the global distribution of the disease—guiding the effort to serve the largest number of people afflicted and those at highest risk. Amazingly, given the geographical distribution of the disease, not a single candidate vac- cine had been made from the sub-type of viruses circulating in Africa. All of the focus had been on candidates made from the sub-types of HIV viruses in the U.S. and Europe. It remains unclear whether it is necessary to develop distinct HIV vaccines for different sub-types of the virus, but having mismatched viruses during testing adds an additional significant dimension to the puzzle. If a candidate is not effective in a given population, it is virtually impossible to innovations / invierno 2006 59 Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023 INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 60 Seth Berkley determine if the failure is attributable to the mismatch of viruses or to a basic inefficacy of the candidate vaccine. Idealmente, candidates are tested in both matched and mismatched settings, allowing testing of the candidate and its applicability in different settings. IAVI was the first organization to work with candidates that were matched to the strains of HIV present in var- ious parts of the world. Hoy, a majority of the candidate vaccines under development, including almost all of the newer candidates, are focused on the developing world. IAVI has also stressed the importance of nurturing research capabilities within developing countries. Until recently, the standard approach in vaccine development was to conduct Phase I and Phase II trials close to the industrial sponsor.7 We decided to help a number of develop- ing countries with a high incidence of HIV/AIDS develop the capability to conduct Phase I tri- als and thus impart clinical know-how and important national ownership of the process. In partnership with many global stakeholders in HIV vaccine development, IAVI established a network of field laboratories for on-site evaluation of immune responses to candidate HIV vaccines. Today trials that conform to international good Clinical and Laboratory Practice (gCLP) standards are underway in places as diverse as Kenya, Uganda, Rwanda, South Africa, and India. To coordinate field lab work and provide comprehensive, ongoing training to all field lab- oratory staff involved in IAVI-sponsored trials, IAVI established a state-of-the-art Human Core Immunology Laboratory (the Core Lab) at the Imperial College in London. The accred- ited gCLP Core Lab serves as IAVI’s main quality control and quality assurance monitoring center and links to other HIV vaccine human immunology laboratories, so that results from IAVI sites anywhere in the world can be compared to results anywhere else within the IAVI net- work as well as to those from other labs that are gCLP certified. This innovative approach to move early testing to high-incidence countries has worked. The quality of the laboratory work and the speed of enrollment often exceed those of our Northern institutional partners. Conducting trials in high-incidence countries has led to increased political support and to the strengthening of the regulatory systems. Our current view is that completely novel technologies should be tested first in industrialized countries with fully-fledged regulatory review systems. En el futuro, especially as countries build capac- ity and gain experience in regulatory work, it will be possible to move novel candidates quick- ly through the legal and regulatory pipelines without first conducting trials in industrialized countries. The clinical trial IAVI and its partners recently launched in Chennai, India is a prime example. Addressing the Dual and Related Challenges of Science and Politics The challenge of developing a preventive vaccine for HIV/AIDS is hardly just a scientific one; en efecto, política, advocacy, and science are integrally connected. Advocacy without science lacks substance. But science without appropriate advocacy may be derailed by political agendas and fail to lead to the appropriate public health results. India provides a good example. For historical reasons, the public in India has come to view the activities of western pharmaceutical companies and researchers with some suspicion; political views have reflected that public concern. Therefore IAVI initiated its program in India by spending three years working with political entities, media, and NGOs at the local, estado, and national levels. Vaccine literacy tool kits and publications were created and disseminated 60 innovaciones / invierno 2006 Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023 INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 61 Ending an Epidemic What does it mean to have an «integrado» y «industrial» acercarse? (cid:121) All R&D activities come together under unified planning and management. (cid:121) Critical disciplines required for vaccine development are represented on a multidiscipli- nary integrated product development team. (cid:121) All product development is managed by experienced industrial project managers using industry’s project management tools. (cid:121) Various candidates in different stages of development and move in parallel, not sequen- inicialmente, under a portfolio approach. (cid:121) Products move quickly without unnecessary delay from discovery to product design and then from manufacturing to clinical trials. (cid:121) Laboratories are internally validated, externally standardized and accredited to support vaccine discovery and clinical trials. (cid:121) Intellectual Property provisions and regulatory actions are tightly linked to product development and trials; access terms are always included. (cid:121) Unpromising products are terminated quickly so funds are used efficiently. in local languages; consultations, discusiones, and advocacy events were undertaken. After a time the development of a preventive HIV/AIDS vaccine was declared a national goal, with a mission-like focus articulated by Dr. A.P.J. Abdul Kalam, President of the Republic of India: This broad governmental commitment has survived a change of political leadership; by the time India actually initiated its first AIDS vaccine trial in 2005, the effort had widespread sup- puerto. India and other southern nations that participated only marginally in vaccine advocacy, investigación, and development five years ago are beginning to lead the field. In June 2003, India, Brasil, and South Africa, with technical assistance from IAVI, created the India-Brazil-South Africa (IBSA) Dialogue Forum to promote trilateral cooperation in HIV/AIDS vaccine research, product development, and clinical capacity-building. India is currently examining how it can harness its powerful scientific, biotech, and manufacturing base to help solve some of the fundamental scientific challenges plaguing the AIDS vaccine field. These middle-income nations, with strong scientific and manufacturing capabilities and political will, could be dom- inant players in vaccine R&D, producción, and distribution in coming years. Beating the Path to Commercialization Many companies have innovative and interesting technologies that they would not normally advance for HIV vaccines. We attempt to identify the best private-sector breakthroughs and then propose that IAVI work with the company to accelerate the development of its technolo- gy as an HIV vaccine product. Given our finances, focus on speed, technical expertise, and clin- ical trials network, as well as the expedited regulatory reviews that are possible with HIV, these promising candidates can move rapidly into the clinic. The company gets its platform technol- ogy validated, which increases its value, and they retain rights for the technology for all non- HIV uses. If the development effort for HIV is successful, IAVI will co-develop the technology with the company, which will have to abide by our access provisions for the developing world. innovaciones / invierno 2006 61 Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023 INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 62 Seth Berkley For example, we worked withTargeted Genetics, a small firm, to move its adeno-associated virus (AAV) vector into the clinic as a prophylactic vaccine. Initially, it was suspected that the vector might integrate into the host chromosome, which would have posed major regulatory challenges, but careful studies and extensive toxicology demonstrated that this was not the case, clearing the way for clinical tests that showed that the vaccine was well tolerated. This led to enormous benefits for the company; IAVI financing of this project helped support some of the company’s researchers, and investor confidence and the stock price rose with each major milestone reached, allowing the company to raise further financing. This is not only possible with smaller companies; we recently concluded a partnership with GlaxoSmithKline to move a chimpanzee adenovirus vaccine to clinical development. IAVI’s Comparative Advantage IAVI is driven by three fundamental principles: velocidad, flexibilidad, and the ability to take informed risk. Although there is a limit to how fast the vaccine development effort can move, given the need for regulatory approvals and adequate time for toxicology and clinical studies, IAVI focuses on minimizing unnecessary delays in vaccine development. When there is a trade-off between speed and finance we tend to emphasize speed—for example, by doing tri- als in parallel rather than sequentially. Cifra 2 shows the ways that candidate development and testing can be accelerated. Because IAVI is a private organization and enjoys unrestricted, flexible support from its donors, it can change directions very rapidly. If a new and promising product appears, we can often commit to moving it forward within weeks. As importantly, if new data demonstrate that a product is less promising, we can stop work immediately and move to more viable vaccine candidates. Finalmente, we are risk takers. Our role is to develop prod- ucts that have potential but may be too risky for private industry. The ability to act quickly has an additional benefit. Because we are nimble and aggressive,we have created some healthy pressure for other HIV vaccine efforts. This healthy competition means that the whole field moves more swiftly. IAVI’s Approach to Intellectual Property—Industry’s Lifeblood Since access to vaccines for the poor is one of the cornerstones of our program, management of intellectual property has been a critical issue for IAVI from its inception. The companies we work with agree to provide vaccines to the public sector in developing countries in reasonable quantities, and within adequate timelines and cost parameters. If companies do not live up to these agreements, then we have “march-in” rights for the technology as well as background and enabling technology.8 The actual implementation of this principle has remained pragmatic and flexible. Approaches include agreements specifying in detail the profit permitted for devel- oping country supply, stipulations that we may seek competitive bids for manufacturing, and partial or full ownership or licensing of the intellectual property on our part. IAVI’S ROLE IN ACCELERATING THE BASIC SCIENCE Although IAVI originally targeted its activities on product development, clinical studies have suggested that the quality of the products needs to improve substantially. Para hacer esto, a series of applied research challenges must be overcome, including understanding how to develop vac- 62 innovaciones / invierno 2006 Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023 INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 63 Ending an Epidemic cines that elicit broadly neutralizing antibodies against globally diverse and circulating strains of HIV, achieving the protection obtained in non-human primate models through experimen- tal use of live-attenuated vaccines, and investigating how mucosal immunity might provide supplemental benefit to systemic immunity. Although these advances will be based on the basic science done by many individual investigators, IAVI concluded that a consortium of sci- entists who shared reagents, viral panels, datos, and employed industrial project management could together advance the field beyond that done by individual investigators. IAVI’s Neutralizing Antibody Consortium (NAC), established in 2002, brought together researchers from academia, government and private companies with a shared and focused mis- sión. In an unusual but critical advancement, the NAC has agreed to intellectual property pro- visions that will guarantee access to any resultant HIV vaccine products to developing coun- intentos, ensuring not only that the individual inventor receives adequate rights and is rewarded for their discovery but also that all members benefit from any discover —thus encouraging group work. Since its inception the NAC has significantly advanced the search for vaccine designs capable of eliciting broadly neutralizing antibodies by solving the crystal structures of the few neutralizing antibodies identified from HIV+ subjects in association with the virus’s outer membrane protein, which is the principal target for neutralization. Reaching these mile- stones has validated the Consortium model for accelerating applied vaccine research, and has led IAVI and others to establish additional consortia focused on solving the correlates of pro- tection (p.ej., IAVI Live Attenuated Consortium) and addressing challenges associated with designing candidate HIV vaccines that elicit mucosal immunity (e.g.CanVac, a consortium of Canadian vaccine researchers). TAPPING THE MARKET IAVI believes that to ensure the development of a vaccine we must fully engage the industrial sector. IAVI has considered a range of incentives that could be used to encourage industrial engagement—not only by reducing the risk through IAVI’s work to advance the science but also by making the market more attractive. Tax credits for the research done to accelerate vac- cines for AIDS, malaria, and tuberculosis have been created in the U.K. and are under consid- eration in the U.S.. Liability protection in the U.S. market has been used for other vaccines and regulatory prioritization has been implemented. Another concept has been to create an advance market commitment (AMC). This initiative received a boost at the G-8 summit at Gleneagles in summer 2005, where leaders endorsed the concept for AMCs for AIDS vaccines and other urgently needed medical innovations. The AMCs would create an artificial market by requiring donors contract to provide subsidies to purchase vaccines for developing coun- tries with specified characteristics once they are developed.9 AMCs seem to be gaining momen- tum and are also supported by current U.S. draft legislation. The G-7 finance ministers fol- lowed suit last fall with their plan to develop a pilot AMC in 2006. Although such pull mech- anisms alone will not solve the AIDS vaccine development problem, along with direct funding for private-sector research they could stimulate an increase in R&D activities, and encourage manufacturers to scale up their production to cover developing markets. innovaciones / invierno 2006 63 Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023 INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 64 Seth Berkley Some IAVI Innovations (cid:121) First biomedical product development public-private partnership (cid:121) First AIDS vaccine candidate designed specifically for Africa (cid:121) First AIDS vaccine trials in Germany, India, Kenya, and Rwanda (cid:121) First HIV vaccine immunological lab in the world to be accredited to the new good clin- ical practices (GCLP) standards; the Ugandan UVRI vaccine research lab was the first lab- oratory in sub-Saharan Africa (other than South Africa) to receive GCLP accreditation (cid:121) Creation of new country model of AIDS vaccine work—»vaccine preparedness»—which fully integrates all levels of engagement across all critical stakeholders (cid:121) First AIDS vaccine policy and integrated policy-advocacy program (cid:121) Seven novel candidates into clinical testing in six years (cid:121) Novel intellectual property agreements with academia, biotech, pharmaceutical and gov- ernment provide product access for the developing world (cid:121) Establishment of applied vaccine research consortia with shared effort and intellectual property (p.ej., Neutralizing Antibody Consortium) OUTCOMES As discussed at the beginning of this case study, when I founded IAVI ten years ago, many were skeptical that a not-for-profit (PDPPP) would yield any result. Although we currently have no AIDS vaccine in hand there have been many important interim accomplishments. In April 2003, an extensive independent evaluation commissioned by the World Bank was conducted of IAVI. The evaluation panel’s findings reflect IAVI’s multiple strategies toward advancing its mission: “IAVI has helped to spur research and development on AIDS vaccines. It has focused the attention of the world on the viral strains circulating in those countries most severely affected by HIV. It has pursued extensive pre-clinical research, helped expand the pipeline of novel candidate vaccines, and has eight vaccine candidates in development. IAVI has helped to raise the political profile of HIV/AIDS. It has increased the attention of policy makers to the need for an AIDS vaccine that would meet the needs of developing countries and that would be available simultaneously throughout the world.” The panel further noted that IAVI has “created a ‘competition’ among researchers that has catalyzed research on AIDS vac- cines,” and become “the world leader in providing information on AIDS vaccines.”10 While many of the innovations developed by IAVI might have occurred in the organiza- tion’s absence, the team concluded that these innovations would have occurred more slowly— and in the search for a lifesaving tool, this is important. As a small NGO operating on a glob- al scale, IAVI has pioneered a significant number of “firsts” (see text box) and has influenced the field of PDPPPs.11 Perhaps the most important effects of IAVI’s work, sin embargo, have been the positive changes in the HIV vaccine field. The G-8 has directly noted the importance of AIDS vaccine research in communiqués from six different summits, and finance for AIDS vac- cine research has increased from an estimated $160M per year in 1993 to more than $500M a decade later (and soon to be over $700M).12 Governments such as the U.S. and India have
declared HIV vaccines to be a national goal. And the number of agencies working toward a
64
innovaciones / invierno 2006
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023
INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 65
Ending an Epidemic
vaccine has increased as well. Four pharmaceutical companies have vaccine candidates in tri-
como, up from two in 2000. The long-standing programs of the NIH have grown and they have
been joined by the European Vaccine Effort Against HIV/AIDS, the Canadian Network for
Vaccines and Immunotherapeutics, the South African AIDS Vaccine Initiative, y el
Australian-Thai HIV Vaccine Consortium, among others. Recently the Bill and Melinda Gates
Foundation brought the different HIV vaccine players together to work in a more collabora-
tive Global HIV Vaccine
Enterprise and dramatically
increased its funding to the field.
IAVI is working closely with this
esfuerzo, serving on the coordinat-
ing committee and on each of the
scientific working groups.
Ten years ago the search for an AIDS
vaccine was at a standstill, el
scientific, political, and economic
obstacles considered insurmountable.
Hoy, there is new momentum and a
conducive environment for vaccine
R&D, with a plethora of new players
all set on one goal.
The science of HIV/AIDS
remains daunting but progress
has been made. The first efficacy
trial of an AIDS vaccine was
completed in 2004. Aunque el
results unfortunately did not
show efficacy, the trial was con-
ducted with excellent compliance
and little ethical controversy.
One more efficacy trial is under-
way and a third candidate vaccine is in critical proof-of-concept studies. Más que 30 candi-
dates are in development, and a renewed effort to solve some of the fundamental scientific
challenges in the past five years will soon bear fruit. We can build on these findings with ade-
quate resources and political commitment, and by matching the best in academic science with
the best in industry in a goal-driven process.
Yet AIDS continues to outpace the global response. Estimates at the end of 2005 sugerir
that despite all of our advances in prevention and treatment, this year had a record number of
new infetions.13 If the epidemic continues another decade on its current trajectory, más que
100 million people will have been infected and will ultimately die of this disease—more than
all that died during the wars of the twentieth century combined. Prevention efforts are lower-
ing HIV prevalence in a handful of countries but current strategies are only partially
effective,and offer women inadequate power or control. Significant strides have been made
over the past decade in treatment options but still only 12 percent of those with HIV/AIDS
have access to AIDS medicines. Despite a global commitment to do better—the G-8 at their
Gleneagles committed to access to AIDS treatment for those in need by 2010—drug toxicity
and viral resistance are spreading around the world. And even countries that have demonstrat-
ed leadership in providing treatment to all their citizens, such as Brazil, face an enormous chal-
lenge, including spending a substantial and growing proportion of their treatment resources
on patients who have developed multi-resistant strains.
Only an AIDS vaccine holds the possibility of ending the epidemic, making it a global pub-
lic good of the highest priority. Ten years ago the search for an AIDS vaccine was at a stand-
innovaciones / invierno 2006
65
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023
INNOV0101FINAL.qxd 2/23/2006 11:49 Página AM 66
Seth Berkley
still, the scientific, political, and economic obstacles considered insurmountable. Today there
is new momentum and a conducive environment for vaccine R&D, with a plethora of new
players all set on one goal. The IAVI model (and now the PDPPP model) creates a laser-
focused effort by joining the best of the public and private sectors—and the lessons learned —
have relevance not only for HIV vaccines, but for other health and non-health technologies. En
the future many global public-health problems will not be solved by either government or
industry alone; to make progress alternative institutional approaches such as those undertak-
en by IAVI will be required. But this will not be easy; for IAVI perhaps the greatest challenge
will be to sustain its long-term effort given the difficulty of the science and the short-term
attention span of most policy makers and institutions.
We invite reader comments. Please send an email to
1. Reports from the Bellagio consultation as well as the other two Rockefeller consultations: the Val de Grace meet-
ing in Paris and the Structure and Financing meeting are available on the IAVI website www.iavi.org.
2. The recently completed VaxGen Phase III efficacy trial of this prototype antibody-based approach thus failed to
confer protection.
3. Previous estimates had looked at those at risk rather than those able to pay or likely to be included in early pub-
lic-sector programs.
4. For a discussion of the various public-private partnerships, ver
5. Craig Wheeler and Seth Berkley, 2001. “Initial lessons from public-private partnerships in drug and vaccine
development.” Bulletin of the World Health Organization 79(8), pag. 29 and references cited therein.
6. The expertise for systematic development of tools to test and enhance a vaccine is uniquely found in industry.
As this is not an “excess capacity,” it is not available to PDPPPs nor academic investigators. This includes adjuvants
(which are additions to the vaccine to enhance their immune responses), as well as specific assays used in their test-
ing and licensure.
7. A Phase I trial tests safety and immune response in a small number of healthy subjects (usually <50). Phase II
trials further test safety and immunogenicity as well as determine proper dosage and dose intervals. It is done with
those populations who will be used for the trial (in this case, high risk) and includes a larger number of subjects
(usually 100’s). A Phase III trial determines if the vaccine has efficacy and will be used to argue for licensure. The
trial is conducted in those at risk for the disease, and although the sample size depends on many factors, it is usu-
ally in the 1000’s.
8. As intellectual property is so critical to companies, particularly small ones, we have often allowed them to keep
their IP. For us to do this, we need to have legally binding agreements that say that if they do not live up to their
commitments we can have the option to take over the product and the enabling technology necessary to use it.
9. More details on these mechanisms can be found on the Center for Global Development website
10. Richard Skolnik, , et. Alabama. Independent evaluation of IAVI, Abril 2003. Available on
11. For a review of the whole field of PDPPPs from the perspective of a major donor, the Rockefeller Foundation,
see “Partnering to develop new products for diseases of poverty—one donor’s perspective,” Rockefeller
Foundation Monograph, Noviembre 2004. Available on
12. For detailed information on funding, see “Tracking Funding for Preventive HIV Vaccine Research &
Desarrollo: Estimates of Annual Investments and Expenditures 2000 to 2005” at
13. For more information on the global HIV/AIDS epidemic, ver
innovaciones / invierno 2006
66
Descargado de http://direct.mit.edu/itgg/article-pdf/1/1/52/704064/itgg.2006.1.1.52.pdf by guest on 08 Septiembre 2023