Parahippocampal and Entorhinal Resection Extent
Predicts Verbal Memory Decline in an
Epilepsy Surgery Cohort
Anli Liu, Thomas Thesen, William Barr, Chris Morrison, Patricia Dugan,
Xiuyuan Wang, Michael Meager, Werner Doyle, Ruben Kuzniecky,
Orrin Devinsky, and Karen Blackmon
D
o
w
n
je
o
un
d
e
d
F
r
o
m
Abstrait
■ The differential contribution of medial-temporal lobe regions
to verbal declarative memory is debated within the neuroscience,
neuropsychology, and cognitive psychology communities. Nous
evaluate whether the extent of surgical resection within medial-
temporal regions predicts longitudinal verbal learning and mem-
ory outcomes. This single-center retrospective observational
study involved patients with refractory temporal lobe epilepsy
undergoing unilateral anterior temporal lobe resection from
2007 à 2015. Thirty-two participants with Engel Class 1 et
2 outcomes were included (14 gauche, 18 droite) and followed for
a mean of 2.3 years after surgery (±1.5 years). Participants had
baseline and postsurgical neuropsychological testing and high-
resolution T1-weighted MRI scans. Postsurgical lesions were
manually traced and coregistered to presurgical scans to pre-
cisely quantify resection extent of medial-temporal regions.
Verbal learning and memory change scores were regressed
on hippocampal, entorhinal, and parahippocampal resection
volume after accounting for baseline performance. Dans l'ensemble,
there were no significant differences in learning and memory
change between patients who received left and right anterior
temporal lobe resection. After controlling for baseline perfor-
mance, the extent of left parahippocampal resection accounted
pour 27% ( p = .021) of the variance in verbal short delay free
recall. The extent of left entorhinal resection accounted for
37% ( p = .004) of the variance in verbal short delay free
recall. Our findings highlight the critical role that the left para-
hippocampal and entorhinal regions play in recall for verbal
matériel. ■
INTRODUCTION
The differential role of medial-temporal lobe regions in
verbal declarative learning and memory is the subject
of ongoing debate. Declarative memory refers to the con-
scious learning of facts and events (Squire & Zola, 1996;
Squire, 1992). It has been clear since the early days of
anteromesial temporal lobe epilepsy surgery in humans
that the hippocampus is critical for initial formation of
declarative memories (Scoville & Milner, 1957). Primate
studies reveal that lesions involving the hippocampal,
parahippocampal, and perirhinal cortex produce worse
memory impairment than lesions involving the hippo-
campal formation alone (Zola-Morgan, Squire, Clower,
& Rempel, 1993; Zola-Morgan, Squire, Amaral, & Suzuki,
1989). De même, larger medial-temporal lesions, y compris
entorhinal and parahippocampal cortex, more consis-
tently lead to impairment in delayed nonmatching to
sample tasks compared with hippocampal-only lesions
(Malkova & Mishkin, 2003; Gaffan, 1994; Murray, Gaffan,
& Mishkin, 1993; Zola-Morgan et al., 1993).
New York University School of Medicine
© 2017 Massachusetts Institute of Technology
Patients undergoing epilepsy surgery provide a means
to investigate the mnemonic contributions of different
medial-temporal subregions, as these regions may be sur-
gically removed to a varying degree if implicated in the
seizure network. For patients with medication-refractory
épilepsie, the best option for achieving seizure freedom is
surgical resection, with 30–80% of patients attaining this
outcome (Tellez-Zenteno, Dhar, & Wiebe, 2005). Pour
patients with temporal lobe epilepsy, rates of seizure
freedom following unilateral anteromesial temporal lobe
résection (ATLR) are higher, entre 66% et 70%
(Spencer & Huh, 2008). In a recent meta-analysis, sei-
zure outcomes following standard ATLR are superior to
selective amygdalohippocampectomy ( Josephson et al.,
2013).
Cependant, negative consequences such as memory im-
pairment are also common (Sherman et al., 2011). Mémoire
subtypes appear highly lateralized, as impairment across
a variety of episodic memory tasks has been demon-
strated with left ATLR, but not right ATLR (Barr, Goldberg,
Wasserstein, & Novelly, 1990). Entre 22% et 63% de
individuals who undergo unilateral left ATLR experience
decline in verbal memory (Sherman et al., 2011), cependant
Journal des neurosciences cognitives 29:5, pp. 869–880
est ce que je:10.1162/jocn_a_01089
je
je
/
/
/
/
j
t
t
F
/
je
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
je
n
t
o
p
un
r
d
c
e
.
d
s
F
je
r
o
je
m
v
e
h
r
c
p
h
un
d
je
je
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
toi
c
n
o
/
c
un
n
r
un
t
r
je
t
je
c
c
je
e
e
–
p
–
d
p
d
2
F
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
un
/
_
j
0
o
1
c
0
n
8
9
_
un
p
_
d
0
1
b
0
oui
8
g
9
toi
.
e
p
s
t
d
o
F
n
b
0
oui
8
S
M.
e
je
p
T
e
m
L
je
b
b
e
r
r
un
2
r
0
je
2
3
e
s
/
j
/
.
t
F
toi
s
e
r
o
n
1
7
M.
un
oui
2
0
2
1
there is a considerable amount of variability in degree of
verbal memory change (Hermann, Seidenberg, Haltiner,
& Wyler, 1995).
Patients who undergo larger unilateral temporal lobe
resections perform worse on an verbal associative learn-
ing and recall tasks than patients who had smaller surger-
ies (Helmstaedter, Petzold, & Bien, 2011; Helmstaedter,
Roeske, Kaaden, Élan, & Schramm, 2011), suggérant
that medial-temporal regions other than the hippocam-
pus support verbal declarative memory formation. Là
is a strong correlation between 18F-fluorodeoxyglucose
uptake in the left perirhinal cortex and learning of arbi-
trary word pairs in patients with left temporal lobe epi-
lépreuse (Weintrob, Saling, Berković, Berlangieri, & Reutens,
2002). De la même manière, the structural integrity of the left perirhinal
region, as measured by MRI T2 relaxation time, is asso-
ciated with learning of arbitrary relational verbal material,
whereas consolidation of the material is related to hippo-
campal integrity (Lillywhite et al., 2007). En outre, concernant-
gional blood flow measured by PET [15Ô]H2O during a
task involving unrelated verbal word pairs implicates a
predominantly left-sided network including dorsolateral
pFC, fusiform, parahippocampal, perirhinal cortices, et
posterior cingulate structures (Weintrob, 2004). Saling has
proposed a two-part model for verbal memory involving
the left temporal lobe: (1) a mesial protosemantic com-
ponent responsible for arbitrary paired associated learn-
ing and (2) a lateral semantic component when semantic
meaning is required (par exemple., during related paired associ-
ates or passage learning; Saling, 2009). En outre,
Fernández and Tendolkar (2006) propose that rhinal
cortex acts as a “gatekeeper” to the hippocampal forma-
tion, with the semantic status of the incoming information
determining probability of transfer to the hippocampus
(Fernández & Tendolkar, 2006).
Variance in neurosurgical practice and cognitive out-
comes in the epilepsy surgical population provides a
unique opportunity to understand the respective contri-
butions of the entorhinal and parahippocampal regions
to the formation and retention of new verbal memory
traces in humans. Ici, we introduce a novel approach
for measuring the extent of entorhinal and parahippo-
campal resection in a case series of patients who under-
went ATLR. We segment the medial-temporal neocortical
architecture of each individual participant on his or her
high-resolution presurgical MRI scan and then coregister
his or her postsurgical lesion mask to this native neuro-
anatomical map. This method allows for precise quan-
tification of resection extent in medial-temporal lobe
subregions and investigation of their particular contribu-
tions to longitudinal verbal declarative memory outcomes.
MÉTHODES
This was a retrospective observational study conducted at
New York University (NYU) Comprehensive Epilepsy
Center at the NYU School of Medicine using data collected
depuis 2007 à 2015. This study was approved by the NYU
School of Medicine institutional review board. All patients
consented to participate in research MRI scanning and
neuropsychological testing and to have their clinical re-
cords reviewed. All patients were adults diagnosed with
medication-refractory focal epilepsy (defined as failure of
at least two appropriately chosen and dosed antiepileptic
medications) and were considered appropriate candidates
for temporal lobe resection.
Clinical Variables
Participants’ clinical data such as seizure type and fre-
quency, age of seizure onset, duration of epilepsy, esti-
mated lifetime number complex partial and secondarily
generalized tonic-clonic seizures, and number of current
antiepileptic medications were extracted from clinical re-
cords. The presence or absence of mesial temporal scle-
rosis was diagnosed using MRI criteria (c'est à dire., hippocampal
volume loss and increased T2 signal on T2-weighted im-
aging) and histopathological evaluation of resected surgi-
cal tissue. The intracarotid sodium amobarbital procedure
(also known as the “Wada test”) variables included lan-
guage lateralization (left/right/ bilateral) and memory
scores for the right and left hemisphere (discrimination
de 12 target objects and pictures from 24 foils). Patients
were followed clinically for at least 1 year to assess post-
surgical clinical outcomes. Seizure type and frequency were
used to determine their Engel class outcome (Ange 1 =
seizure free, Ange 2 = rare disabling seizures, Ange 3 =
worthwhile reduction in seizure frequency, Ange 4 = no
worthwhile improvement; 1992 Palm Desert Conference
on Epilepsy Surgery).
Participant Population
Il y avait 34 participants initially enrolled in this study,
y compris 15 who underwent a left ATLR and 19 OMS
underwent a right ATLR. Two participants were excluded
from analyses because of poor postsurgical seizure out-
comes (Engel class 3–4). The remaining group of 32
participants had a mean age of 35.5 années (range =
16–63 years) at time of surgery and mean postoperative
follow-up of 2.41 années (SD = 1.45 années; Tableau 1). Mean
age of seizure onset was 15.1 années (range = 1–47 years),
with a mean duration of seizures of 18.9 années (SD = 14.2).
About 41% of the cohort had mesial temporal sclerosis
identified by pathology. Mean educational level was
15.0 années (SD = 2.8). At presurgical baseline testing, par-
ticipants had an average IQ of 99.0 (SD = 13.8). As a group,
patients had low depression (mean BDI = 9.3, SD = 5.7)
and anxiety (mean = 11.3, SD = 11.4) scores. Il y avait
no differences in baseline or postsurgical demographic,
clinical, or neuropsychological characteristics of patients
who underwent a left- or right-sided ATLR (Tableau 1), sauf
that patients who received a left ATLR showed a trend
toward a lower left-sided Wada memory score at baseline
870
Journal des neurosciences cognitives
Volume 29, Nombre 5
D
o
w
n
je
o
un
d
e
d
F
r
o
m
je
je
/
/
/
/
j
F
/
t
t
je
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
je
n
t
o
p
un
r
d
c
e
.
d
s
F
je
r
o
je
m
v
e
h
r
c
p
h
un
d
je
je
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
toi
c
n
o
/
c
un
n
r
un
t
r
je
t
je
c
c
je
e
e
–
p
–
d
p
d
2
F
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
un
/
_
j
0
o
1
c
0
n
8
9
_
un
p
_
d
0
1
b
0
oui
8
g
9
toi
.
e
p
s
t
d
o
F
n
b
0
oui
8
S
M.
e
je
p
T
e
m
L
je
b
b
e
r
r
un
2
r
0
je
2
3
e
s
/
j
/
t
.
F
toi
s
e
r
o
n
1
7
M.
un
oui
2
0
2
1
Tableau 1. Demographic and Baseline Clinical Characteristics of Participants (Engel Classes 1 et 2 Only, N = 32, Mean ± SD)
All Participants
Left ATLR
Right ATLR
p
Demographic and Clinical Characteristics
Number of participants
Age at surgery (années, range)
Sex (male/female)
Éducation (années)
N = 32
35.53 (16–63)
17/15
N = 14
N = 18
36.57 ± 9.35
34.72 ± 13.54
8/6
9/9
15.0 ± 2.77
15.00 ± 2.08
15.00 ± 3.12
Ethnicity
Blanc
Noir
Hispanic
Asian
Handedness
(right/left/ambidextrous)
23 (71.9%)
4 (12.5%)
4 (12.5%)
1 (3.1%)
23/8/1
10
2
2
0
13
2
2
1
10/4/0
13/4/1
Age at seizure onset (années)
15.06 (1–47)
15.71 ± 10.36
14.56 ± 11.24
Duration of seizures (années)
18.88 ± 14.18
18.93 ± 13.34
18.83 ± 15.18
Years of follow-up after
surgery (années)
2.41 ± 1.45
2.51 ± 1.46
2.34 ± 1.50
Mesial temporal sclerosis
13/17 (40.6%/53.1%)
Engel class outcome
Class 1
Class 2
27 (84.4%)
5 (15.6%)
4/9
11
3
9/8
16
2
Baseline Neuropsychological Testing
FSIQ
99.04 ± 13.76
98.83 ± 13.99
99.19 ± 14.05
Verbal Comprehension Index
100.5 ± 19.82
94.36 ± 18.98
105.28 ± 19.64
Perceptual Reasoning Index
98.84 ± 15.39
101.14 ± 17.77
97.06 ± 13.51
Working Memory Index
Processing Speed Index
Verbal Learning
Verbal SDFR
Verbal LDFR
Visual Confrontation
Naming (BNT)
Visual Memory
(RCFT delay trial)
BDI
BAI
Left Wada memory score
Right Wada memory score
Wada language
(left/right/bilateral)
93.78 ± 18.64
93.72 ± 19.71
46.81 ± 12.89
8.85 ± 3.53
9.42 ± 3.67
99.50 ± 10.06
89.50 ± 22.49
97.75 ± 10.91
90.88 ± 24.02
45.14 ± 14.69
46.33 ± 9.94
8.21 ± 3.42
8.71 ± 3.47
8.58 ± 3.58
9.58 ± 3.42
50.20 ± 7.30
48.93 ± 6.96
51.31 ± 7.64
12.90 ± 6.48
14.00 ± 7.47
12.17 ± 5.84
9.26 ± 5.73
9.15 ± 5.90
9.36 ± 5.79
11.32 ± 11.35
12.07 ± 12.69
10.57 ± 10.26
9.03 ± 3.52
7.32 ± 3.32
30/0/1
7.64 ± 3.97
8.29 ± 2.64
13/0/1
10.18± 2.72
6.47 ± 3.70
17/0/0
.666
.688
1.00
.735
(Fisher’s exact)
.636
.767
.985
.763
.283
.631
.948
.124
.465
.164
.365
.404
.190
.346
.382
.458
.929
.734
.055
.138
.452
(Fisher’s exact)
Liu et al.
871
D
o
w
n
je
o
un
d
e
d
F
r
o
m
je
je
/
/
/
/
j
F
/
t
t
je
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
je
n
t
o
p
un
r
d
c
e
.
d
s
F
je
r
o
je
m
v
e
h
r
c
p
h
un
d
je
je
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
toi
c
n
o
/
c
un
n
r
un
t
r
je
t
je
c
c
je
e
e
–
p
–
d
p
d
2
F
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
un
/
_
j
0
o
1
c
0
n
8
9
_
un
p
_
d
0
1
b
0
oui
8
g
9
toi
.
e
p
s
t
d
o
F
n
b
0
oui
8
S
M.
e
je
p
T
e
m
L
je
b
b
e
r
r
un
2
r
0
je
2
3
e
s
/
j
.
F
t
/
toi
s
e
r
o
n
1
7
M.
un
oui
2
0
2
1
Tableau 1. (a continué )
Postsurgical Neuropsychological Testing
All Participants
Left ATLR
Right ATLR
FSIQ
99.61 ± 14.61
99.25 ± 11.35
99.88 ± 17.02
Verbal Comprehension Index
103.93 ± 15.02
101.00 ± 9.83
106.00 ± 17.82
Perceptual Reasoning Index
99.45 ± 13.58
101.33 ± 11.74
98.12 ± 14.95
Working Memory Index
100.56 ± 14.76
103.45 ± 13.78
98.56 ± 15.50
Processing Speed Index
97.18 ± 14.01
96.42 ± 14.79
97.75 ± 13.87
Verbal Learning
Verbal SDFR
Verbal LDFR
42.56 ± 10.81
39.08 ± 10.77
46.33 ± 9.94
6.92 ± 3.67
7.60 ±4.26
5.38 ± 3.15
5.77 ± 4.30
8.58 ± 3.58
9.58 ± 3.34
Visual Confrontation Naming
48.30 ± 8.81
44.36 ± 9.52
52.54 ± 5.70
(BNT)
Visual Memory
(RCFT delay trial)
BDI
BAI
10.97 ± 5.17
12.69 ± 5.66
9.56 ± 4.43
8.13 ± 7.32
6.84 ± 6.40
9.36 ± 8.23
8.29 ± 7.97
7.12 ± 6.56
5.64 ± 4.67
Independent samples t test comparison performed with p values listed.
*Significant after correction for multiple comparisons.
p
.913
.387
.540
.408
.809
.094
.026
.022
.012
.106
.406
.260
(7.6 vs. 10.2, p = .055), as well as lower postsurgical verbal
memory and naming scores, compared with patients who
received a right-sided resection.
Neuropsychological Testing
Presurgical comprehensive neuropsychological testing
was conducted as part of routine clinical practice. Post-
surgical neuropsychological testing was acquired for
recherche (at least 6 months following surgery) and included
the same test battery administered presurgically. Le
neuropsychological test battery adhered to the National
Institute of Neurological Disorders and Stroke common
data elements protocol for epilepsy (Loring et al., 2011),
with the exception of the California Verbal Learning Test-
2nd Edition (CVLT-II), which was administered to patients
before 2011. The Wechsler Adult Intelligence Scale-Third
or Fourth Edition (WAIS-III or WAIS-IV) was administered
to obtain the Full-Scale Intellectual Quotient (FSIQ). Par-
ticipants completed standard questionnaires of mood
functioning, including the Beck Anxiety Inventory (BAI;
Beck & Steer, 1993) and Beck Depression Inventory-II
(BDI-II; Beck, Steer, & Brun, 1996 ). Measurements of
global cognitive functioning (FSIQ) and mood (BAI, BDI-II)
were used to determine whether changes in these vari-
ables contributed to memory decline between pre- et
postsurgical time points.
Verbal declarative memory was assessed with serial
word list-learning tasks (Rey Auditory Verbal Learning Test
or the CVLT-II; Taylor, 1959). On both of these list-learning
tasks, examinees are asked to learn a list of words (List A)
across a series of five learning trials, given a second dis-
traction word list (List B), and then they are asked to freely
recall words from List A. Free recall of the List A words are
tested after a brief (2 min) and long (20 min) delay. Le
total score across all five learning trials was used as a
measure of verbal learning; the short delay free recall
(SDFR) score represents verbal free recall after 2 min and
the long delay free recall (LDFR) score represents verbal
free recall after 20 min (Taylor, 1959). Raw scores across
these two list-learning tasks are highly correlated in patients
with closed head injuries whereas normalized scores differ
(Stallings, Boake, & Sherer, 1995); donc, raw scores
were utilized for this study. Within an individual, the same
list-learning task was administered pre- and postsurgically.
Longitudinal change in verbal declarative learning and
memory performance was assessed by subtracting the post-
surgical test score from the presurgical test score. Negative
scores indicate decline in performance, and positive scores
indicate improvement. The following dependent variables
were used in subsequent analyses of longitudinal change
in neuropsychological performance: Change in Verbal
Apprentissage, Verbal SDFR (SDFR-change), and Verbal LDFR
(LDFR-change).
To test the specificity of findings to verbal declarative
mémoire, we calculated change scores for the Boston
Naming Test (BNT), a measure of visual confrontation
naming, and the Rey Complex Figure Test (RCFT)-Delayed
Recall Trial, a measure of memory for visual material.
Enfin, we calculated change scores for the BAI and BDI
872
Journal des neurosciences cognitives
Volume 29, Nombre 5
D
o
w
n
je
o
un
d
e
d
F
r
o
m
je
je
/
/
/
/
j
F
/
t
t
je
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
je
n
t
o
p
un
r
d
c
e
.
d
s
F
je
r
o
je
m
v
e
h
r
c
p
h
un
d
je
je
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
toi
c
n
o
/
c
un
n
r
un
t
r
je
t
je
c
c
je
e
e
–
p
–
d
p
d
2
F
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
un
/
_
j
0
o
1
c
0
n
8
9
_
un
p
_
d
0
1
b
0
oui
8
g
9
toi
.
e
p
s
t
d
o
F
n
b
0
oui
8
S
M.
e
je
p
T
e
m
L
je
b
b
e
r
r
un
2
r
0
je
2
3
e
s
/
j
t
.
F
/
toi
s
e
r
o
n
1
7
M.
un
oui
2
0
2
1
to ensure that changes in verbal declarative memory were
not associated with changes in mood or anxiety.
MRI Scanning Protocol
Before resective epilepsy surgery, all patients completed
a high-resolution T1-weighted MPRAGE (echo time =
3.25 msec, repetition time = 2530 msec, inversion time =
1100 msec, flip angle = 7°, field of view = 256 mm,
matrix = 2566256, voxel size = 1 × 1 × 1.3 mm) sur
a Siemens (Erlangen, Allemagne) Allegra 3T research-
dedicated MR scanner. Immediately following resective
surgery (c'est à dire., within 24 hr), a clinical MRI scanning pro-
tocol was acquired at the NYU Department of Radiology
on 1.5-T and 3-T Siemens scanners. In many patients, un
additional postsurgical MRI scan was acquired at a sec-
ond time point more remote to surgery (c'est à dire., plus que
6 months to 1 year after surgery); cependant, in these re-
mote MRI scans there was evidence of brain shift, lequel
tended to increase error in the coregistration of post-
surgical to presurgical MRI scans. Error associated with
brain shift over time was greater than error associated
with immediate postsurgical brain swelling; donc,
in all cases the MRI scan that was acquired proximal
to surgery was utilized. Postsurgical image acquisitions
were used for manual tracing of the surgical lesion and
included a high-resolution T1-weighted volume (MPRAGE)
and a T2-weighted FLAIR volume, which was used to im-
prove visualization of postsurgical lesion extent.
IRM, (3) rigid body coregistration of the postsurgical MRI
lesion mask to the native presurgical MRI scan, et (4)
quantification of the percentage of each labeled subregion
that was surgically resected. By coregistering the postsurgical
lesion mask to an individual’s presurgical MRI rather than
a standard neuroanatomical atlas, this procedure pre-
serves native architectural features and allows for precise
delineation of subregion lesion extent. These steps are
outlined in more detail below.
Neuroanatomical Labeling of Subcortical
Structures and Cortical Regions on
Presurgical Scans
Subcortical Segmentation and Labeling
Presurgical images were processed with FreeSurfer 5.1
software package (surfer.nmr.mgh.harvard.edu). Segmen-
tation and labeling of subcortical structures (voir la figure 1)
was performed by rigid body alignment of the partici-
pant’s brain to a probabilistic atlas, followed by nonlinear
morphing to the atlas. Labels were generated based on
the prior probability of a given tissue class occurring at
a specific atlas location, the likelihood of the image inten-
sity given that tissue class, and the probability of the local
spatial configuration of labels given the tissue class (Fischl
et coll., 2002). Labels were manually inspected and, in rare
cases, corrected if necessary. ROIs for the current study in-
clude the hippocampus, entorhinal, and parahippocampal
régions.
Quantifying Surgical Lesion Extent
Surgical lesion extent for specific temporal lobe subregions
was quantified by (1) anatomical labeling of the high-
resolution presurgical MRI scan (see below), (2) slice-by-
slice manual tracing of lesion extent on the postsurgical
Cortical Surface Reconstruction, Segmentation,
and Labeling
Freesurfer 5.1 was used to reconstruct, segment, and label
the cortical sheet. These procedures are described in detail
in prior publications (Fischl, Séréno, & Dale, 1999; Fischl
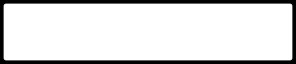
Chiffre 1. Methods for precise
delineation and quantification
of surgical resection extent.
(UN) Presurgical T1-weighted
scan is (B) segmented with
FreeSurfer software for
labeling of individual
subcortical and cortical
anatomy. (C) Post-surgical T1
is coregistered to presurgical
T1 MPRAGE. (D) Resection
mask is drawn with respect
to presurgical boundaries.
(E) Resection mask is overlaid
on presurgical scan with
subcortical and cortical
labeling. (F) Percentage of
tissue resected for each
labeled structure/region.
D
o
w
n
je
o
un
d
e
d
F
r
o
m
je
je
/
/
/
/
j
t
t
F
/
je
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
je
n
t
o
p
un
r
d
c
e
.
d
s
F
je
r
o
je
m
v
e
h
r
c
p
h
un
d
je
je
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
toi
c
n
o
/
c
un
n
r
un
t
r
je
t
je
c
c
je
e
e
–
p
–
d
p
d
2
F
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
un
/
_
j
0
o
1
c
0
n
8
9
_
un
p
_
d
0
1
b
0
oui
8
g
9
toi
.
e
p
s
t
d
o
F
n
b
0
oui
8
S
M.
e
je
p
T
e
m
L
je
b
b
e
r
r
un
2
r
0
je
2
3
e
s
/
j
.
/
F
t
toi
s
e
r
o
n
1
7
M.
un
oui
2
0
2
1
Liu et al.
873
et coll., 2002; Dale, Fischl, & Séréno, 1999). In brief, processus-
ing steps included segmentation of gray matter and white
matter, inflation and flattening of the cortical surface, et
automatic correction of topological defects. D'abord, intensity
variations due to magnetic field inhomogeneities are cor-
rected; a normalized intensity image is created; et le
skull is removed from the high-resolution, T1-weighted,
anatomical MR image. The cortical gray matter ribbon is
segmented, and the resulting surface is covered with a po-
lygonal tessellation and smoothed to reduce metric
distortions. After constructing the initial surface model, un
refinement procedure delineates the gray/white interface.
This surface is subsequently deformed outwards to obtain
an explicit representation of the pial surface. Alors, un
automated method for subdividing the human cerebral
cortex into standard gyral-based neuroanatomical regions
is applied (Desikan et al., 2006). This method results in
the neuroanatomic labeling of 34 cortical regions (voir
Figure 1B) and corresponding white matter regions. Le
following ROIs were analyzed given that they are typically
included (to varying degrees) in a standard ATLR: entorhi-
nal, fusiform gray matter, parahippocampal, inferior
temporal lobe, middle temporal lobe, superior temporal
lobe, temporal pole.
Manual Lesion Tracing and Estimation of
Resection Percentages
Before lesion tracing, the postoperative T1-weighted and
FLAIR images were coregistered to the preoperative T1-
weighted image using rigid body linear transformation
algorithms. Surgical lesion masks were manually traced on
the postsurgical T1-weighted scan, with the T2-weighted
FLAIR image used to verify lesion boundaries (see Fig-
ure 1C–D). Lesion masks were crosschecked across the
coronal, axial, and sagittal planes of the T1-weighted image.
Each postoperative slice was visually reviewed against the
presurgical segmentations, and if there was evidence of
brain shift, then the masks were manually adjusted accord-
franchement. These resection masks were then overlaid onto the
neuroanatomical division maps of the individual patient to
calculate the percentage of the subcortical and cortical re-
gions that were removed (see Figure 1E–F). Total resection
extent was calculated as a percentage of the total supra-
tentorial brain volume. The hippocampus and amygdala
resection extent was quantified as a percentage of total
preoperative hippocampus and amygdala volume removed
for each patient. Resection extent for entorhinal, para-
hippocampal, fusiform, temporal pole, superior temporal,
middle temporal, and inferior temporal gray and white
matter regions was quantified as a percentage of total pre-
operative area removed for each patient.
Statistical Analysis
Statistical analysis was performed with SPSS Version 22.0
(SPSS, Inc., Chicago, IL). Descriptive statistics, y compris
frequencies, moyens, and standard deviations, were calcu-
en retard. An independent samples t test with a p value of .05
was used to determine differences for all continuous var-
iables such as clinical, demographic, and baseline neuro-
psychological testing by side of surgery. For comparison
between categorical variables such as Engel class outcome
and side of surgery, a Fisher’s exact test was used. Pour
analysis of longitudinal neuropsychological outcomes,
only Engel Classes 1 et 2 outcomes were included to
avoid confounding poor seizure control or impact of med-
ication changes with cognitive performance. A repeated-
measures ANOVA with Lesion group (right/left) as the
between-subject factor and Time point (pre/post) as the
within-subject factor was conducted, with performance
on verbal memory tests as the dependent variables.
Regression analyses were performed to examine the rela-
tionship between resection extent of the medial-temporal
subregions (hippocampus, entorhinal cortex, and para-
hippocampal regions) and change in verbal learning
and memory scores, after accounting for baseline per-
formance. Given the strong established relationship be-
tween verbal memory decline and left-sided resection
described in the literature, we performed separate re-
gression analyses in the left and right ATLR groups. À
account for multiple comparisons, Benjamini–Hochberg
correction for false discovery rate was applied.
RÉSULTATS
Surgical Resection
The extent of surgical resection was quantified for total
resection volume, percentage of total brain volume re-
sected, as well as for each temporal lobe substructure,
and described in more detail in Table 2. There was a sig-
nificant difference in the total resection volume and the
percentage of total brain volume resected between
patients who received left ATLR versus right ATLR ( p <
.001). There was a wide degree of variance of medial-
temporal structures resected (see Table 2). Patients
who underwent a left ATLR had significantly decreased
extent of inferior, mid, and superior temporal neocortical
and subcortical tissue resected compared with right ATLR
( p < .001). Patients who underwent a right ATLR had
slightly less hippocampus resected (left 0.84, SD = 0.07
vs. right 0.91, SD = 0.09; p = .014). Other resection extent
percentages were statistically similar.
Cognitive Outcomes
Among participants who had an Engel Class 1 or Engel
Class 2 outcome (n = 32), there was an average decrease
in all measures of verbal memory (Figure 2; Table 3). After
correction for multiple comparisons, there were no sig-
nificant differences in memory performance change by
side of resection, although there was a trend toward
874
Journal of Cognitive Neuroscience
Volume 29, Number 5
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
a
/
_
j
0
o
1
c
0
n
8
9
_
a
p
_
d
0
1
b
0
y
8
g
9
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
t
/
f
.
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
Table 2. Surgical Resection Extent by Side of Resection (Engel Classes 1 and 2 Only, n = 32)
Region
Total resection volume (mm3)
Percentage of total brain volume resected
Hippocampal (gray matter)
Entorhinal (gray and white matter)
Parahippocampal (gray and white matter)
Fusiform (gray and white matter)
Temporal pole (gray and white matter)
Inferior temporal (gray and white matter)
Mid temporal (gray and white matter)
Superior temporal (gray and white matter)
Range
17319–66955
Left ATLR
(n = 14)a
Right ATLR
(n = 18)a
29139 ± 9103
46165 ± 11938
0.02–0.07
0.64–1.00
0.32–0.97
0–0.97
0.08–0.46
0.49–1.00
0.08–0.67
0.04–0.61
0.02–0.79
0.03 ± 0.01
0.84 ± 0.07
0.84 ± 0.20
0.62 ± 0.28
0.19 ± 0.06
0.89 ± 0.13
0.20 ± 0.11
0.14 ± 0.10
0.08 ± 0.07
0.04 ± 0.01
0.91 ± 0.09
0.89 ± 0.10
0.64 ± 0.24
0.27 ± 0.09
0.94 ± 0.06
0.40 ± 0.13
0.35 ± 0.15
0.37 ± 0.15
pb
<.001*
<.001*
.014*
.394
.507
.009*
.166
<.001*
<.001*
<.001*
aMeans and SD percentage resection of each temporal lobe substructure given for left and right ATLR.
bIndependent samples t test comparison performed with p values listed.
*Significant after correction for multiple comparisons.
differing BNT and BDI changes, with patients receiving
a left ATLR exhibiting a greater decline in naming and
patients receiving a right ATLR reporting less depression
after surgery.
Predictors of Verbal Declarative Memory Outcomes
Clinical characteristics including age of seizure onset,
duration of seizures before surgery, educational level,
verbal IQ, and ipsilateral Wada memory score were not
correlated with change in verbal learning or memory
(Table 4); however, there was a positive correlation be-
tween baseline verbal learning and verbal learning change
(r = .54, p = .006) and baseline SDFR and SDFR-change
(r = .44, p = .026). There was no correlation between
baseline LDFR and LDFR change (r = .286, p = .17).
Neither total resection volume or percentage of total
brain volume resected was significantly correlated with
change in verbal learning or memory.
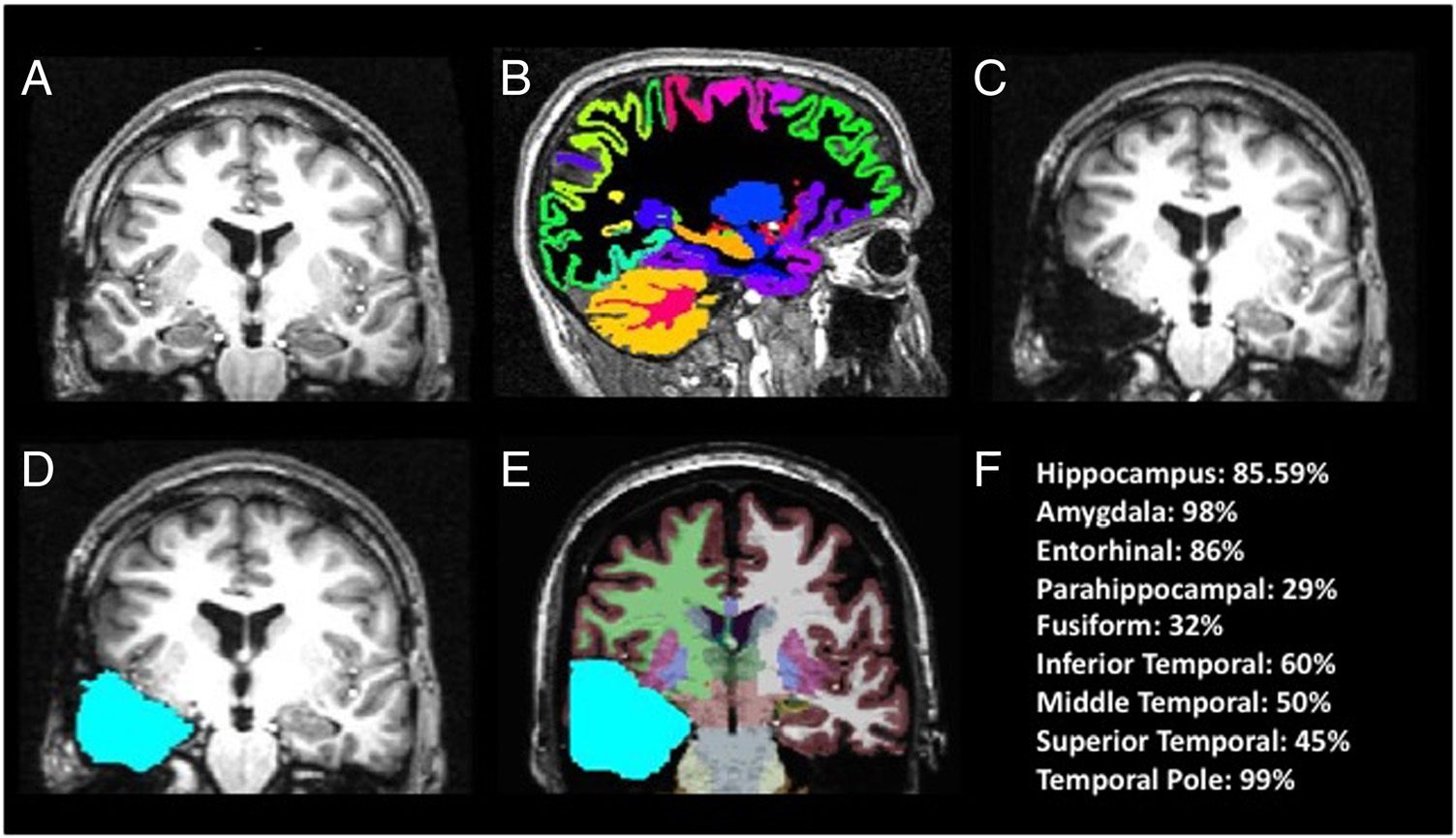
Figure 2. Percent change
in neuropsychological
outcomes by side of
resection, for Engels
1 and 2 only (N = 32).
Patients with a left ATLR
(red) are compared with
patients who received a
right ATLR (blue) percent
change across each
neuropsychological measure
after surgery. Bars represent
SEMs. There is a statistically
significant difference
between patients who
received a left-sided
versus a right-sided ATLR
in performance in the BNT
and the BDI; otherwise,
there were no differences
between left and right
ATLR groups. Patients who
received a left ATLR had a
trend toward more decline
in verbal learning and
recall scores.
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
a
/
_
j
0
o
1
c
0
n
8
9
_
a
p
_
d
0
1
b
0
y
8
g
9
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
.
f
t
/
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
Liu et al.
875
Table 3. Change in Neuropsychological Outcomes (Raw Scores, for Engel Classes 1 and 2 Only, n = 32)
Neuropsychological Test
All Participants
Verbal Learning (L = 14, R = 13)c
−5.60 ± 10.56
Verbal SDFR (L = 14, R = 13)c
Verbal LDFR (L = 14, R = 13)c
RCFT (L = 11, R = 16)
Visual Confrontation Naming
(BNT) (L = 14, R = 13)
BDI (L = 13, R 13)
BAI (L = 14, R = 13)
−2.00 ± 3.38
−1.92 ± 3.57
−2.30 ± 5.67
−1.62 ± 7.10
−2.85 ± 7.54
−5.11 ± 11.32
pa
.014*
.007*
.011*
.045*
.244
.066
.027*
Left ATLR
Right ATLR
−8.31 ± 11.50
−2.92 ± 3.55
−3.07 ± 3.55
−0.73 ± 6.76
−4.43 ± 8.40
−2.67 ± 8.39
−1.00 ± 3.01
−0.67 ± 3.08
−3.38 ± 4.72
1.53 ± 3.71
0.08 ± 6.78
−5.77 ± 7.34
−3.79 ± 11.84
−6.54 ± 10.95
pb
.188
.159
.084
.241
.022
.045
.524
aGroup level differences were calculated with a paired t test (post–pre), with mean raw scores and SD given for all participants.
b Independent samples t test comparing change in neuropsychological test scores. After correction for multiple comparisons, there were no
differences in the change in neuropyschological test outcomes for left- versus right-sided resections.
cCalculated for all participants with same memory test given pre- and postsurgery (CVLT and Rey Auditory Verbal Learning Test) for Engel Classes 1 and
2 only (n = 25).
*Significant change from presurgical to postsurgical testing.
Among participants who received a left ATLR, we found
that baseline verbal learning performance accounted for
37% of the variance in verbal learning decline (Table 5).
After accounting for baseline performance, the extent of
parahippocampal resection (gray and white matter) con-
tributed an additional 27% of the variance in verbal learning
decline, although this did not reach statistical signifi-
cance after correction for multiple comparisons ( p = .02;
Table 5A). Baseline verbal SDFR performance accounted
for 37% of the variance in verbal SDFR-change. The extent
of entorhinal region (gray and white matter) resection
accounted for an additional 37% of the variance ( p =
.004), after controlling for the contribution of baseline
SDFR performance. In a separate model, the extent of para-
hippocampal resection accounted for 27% of the variance
in verbal SDFR-change, after controlling for baseline per-
formance ( p = .021; Table 5B). For LDFR-change, none
of the regional resection extent values predicted perfor-
mance decline (Table 5C). In summary, after correction
for multiple comparisons, resection extent in parahippo-
campal and entorhinal regions remained significant pre-
dictors of decline in verbal SDFR.
Discriminant Validity of Left Parahippocampal and
Entorhinal Findings
To determine whether decline in verbal SDFR-change
was being driven by resection extent in left entorhinal
and parahippocampal regions and not other left temporal
lobe subregions, we entered the remaining left temporal
lobe subregions (i.e., fusiform, temporal pole, inferior
temporal, middle temporal, and superior temporal gray
and white matter) as predictors of verbal SDFR-change
in separate regression models. There was no relationship
between resection extent in any of these left temporal
subregions and verbal SDFR-change. Furthermore, we
examined the relationship between verbal SDFR-change
Table 4. Participant Characteristics Predicting Verbal Memory Decline After Surgery (for Engel Classes 1 and 2 Only, n = 32)
Verbal Learningb
Verbal SDFR b
Verbal LDFR b
Participant Characteristics
Age of seizure onset
Duration of seizures before surgery
Education
Verbal IQ
Ipsilateral WADA Memory Score
R
.067a
−.045
.246
.079
−.167
p
.750
.830
.236
.720
.436
R
.085
<.001
.073
−.011
−.198
p
.687
1.000
.729
.961
.354
R
.063
.029
.292
.189
−.295
p
.763
.892
.157
.387
.162
aValues provided are Pearson correlations (bivariate), with two-tailed p values.
bFor verbal change scores, only participants who took the same memory test pre and post were included (n = 25).
876
Journal of Cognitive Neuroscience
Volume 29, Number 5
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
a
/
_
j
0
o
1
c
0
n
8
9
_
a
p
_
d
0
1
b
0
y
8
g
9
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
t
f
.
/
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
Table 5. Verbal Learning, SDFR, and LDFR Change
A. Linear Regression with Verbal Learning Change as the Dependent Variable, for Left ATLR, Engel Classes 1–2 Only (n = 13)
Baseline VL R2
R2-Change
Total R 2
Standardized β
t
p
Total volume resected
Hippocampus
Entorhinal region
(GM + WM)
Parahippocampal region
(GM + WM)
.37
.41
.37
0.37
.05
.09
.06
.41
.50
.43
0.27
0.64
−0.21
−0.32
−0.25
−0.52
−0.862
.409
−1.30
−1.03
−2.76
.23
.33
.02
B. Linear Regression with SDFR Change as the Dependent Variable, for Left ATLR and Engel Classes 1–2 Only (n = 13)
Total volume resected
Hippocampus
Entorhinal region
(GM + WM)
Parahippocampal region
(GM + WM)
Baseline
SDFR R2
.37
.63
.37
.37
R2-Change
Total R2
Standardized β
.02
.05
.37
.27
.39
.68
.74
.637
−0.14
−0.22
−0.614
−0.520
t
−0.56
−1.14
−3.72
p
.590
.29
.004*
−2.73
.021*
C. Linear Regression with LDFR Change as the Dependent Variable, for Left ATLR, Engel Classes 1–2 Only (n = 13)
Total volume resected
Hippocampus
Entorhinal Region
(GM + WM) (n = 13)
Parahippocampal region
(GM + WM)
Total R2
Standardized β
t
.037
.188
.275
.144
−0.192
−0.433
−0.524
−0.649
−1.521
−2.042
−0.338
−1.192
p
.530
.159
.066
.258
*Significant after correction for multiple comparisons ( p < .05).
and resection extent in all of the right temporal lobe sub-
regions of patients who underwent right ATLR, and there
were no significant findings. To establish the specificity of
findings to verbal declarative memory, we examined the
relationship between resection extent in left entorhinal
regions and BNT-change ( p = .252), RCFT-change ( p =
.262), BDI-change ( p = .296), and BAI change ( p =
.857), and there were no significant findings. Likewise,
there was no significant correlation between left para-
hippocampal resection extent and BNT-change ( p =
.368), RCFT change ( p = .692), BDI-change ( p = .688),
or BAI change ( p = .851). In addition, there was no rela-
tionship between change in verbal SDFR and improve-
ment in depression ( p = .514) or anxiety ( p = .821)
symptoms. Taken together, these results demonstrate
that greater resection extent of left entorhinal and para-
hippocampal regions predicts decline in verbal declarative
memory specifically and not neuropsychological functions
in general.
DISCUSSION
In this retrospective longitudinal study, we demonstrate
that the degree of left parahippocampal and entorhinal
resection predicted decline in verbal declarative memory
performance, after correction for multiple comparisons.
This finding was present after accounting for the contri-
bution of baseline verbal memory performance, which
has been reported as a critical variable in prior literature
(Dulay & Busch, 2012; Baxendale, Thompson, Harkness,
& Duncan, 2006). It is important to note that the total
resection volume and resection extent of other left
and right temporal subregions were not related to
verbal memory outcomes, suggesting that the extent of
Liu et al.
877
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
a
/
_
j
0
o
1
c
0
n
8
9
_
a
p
_
d
0
1
b
0
y
8
g
9
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
t
.
/
f
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
resection of left parahippocampal and entorhinal regions
made a specific contribution to verbal memory decline.
However, we cannot draw conclusions about the contri-
bution of hippocampal resection, as this structure was
nearly completely resected in most cases (0.84 ± 0.07).
Declines in verbal memory after left temporal lobectomy
have been described in other retrospective neurosurgical
series (Helmstaedter, Petzold, et al., 2011; Helmstaedter,
Roeske, et al., 2011; Helmstaedter, Grunwald, Lehnertz,
Gleissner, & Elger, 1997) and selective amygdalo-
hippocampectomy (Wendling et al., 2013; Morino et al.,
2006). However, there are mixed findings in verbal mem-
ory outcomes between the more selective mesial temporal
and complete temporal lobe resection (Kuang, Yang, Gu,
Kong, & Cheng, 2014; Wendling et al., 2013; Helmstaedter
et al., 2008; Morino et al., 2006). Our findings extend pre-
vious reports by identifying key temporal lobe subregions
that appear to drive verbal memory decline. These find-
ings are consistent with a small case series of patients
who had hippocampal-sparing temporal lobe resections;
only patients who had perirhinal and entorhinal cortex
resections had an immediate and lasting effect on asso-
ciative learning of unrelated word pairs (Weintrob, Saling,
Berkovic, & Reutens, 2007).
Our findings highlight the critical role that the perfor-
ant pathway plays in encoding and STM for verbal mate-
rial. The entorhinal cortex plays a privileged role because
it receives input from the perirhinal cortex and para-
hippocampal cortex and communicates directly to
the dentate gyrus and CA1–C3 hippocampal subfields
(Eichenbaum, Sauvage, Fortin, Komorowski, & Lipton,
2012). Entorhinal cortex serves as a critical gateway
facilitating transfer and convergence of unimodal and
polymodal sensory input from the dorsal and ventral
streams to the hippocampus (Eichenbaum et al., 2012).
In particular, entorhinal cortex may be particularly acti-
vated by novel information, increasing the probability of
transfer to the hippocampus for encoding (Fernández &
Tendolkar, 2006). Communication between entorhinal
cortex and hippocampus is facilitated by phase-coupled
theta and gamma frequency activity (Fell, Klaver, Elger,
& Fernandez, 2002). MRI volumetric studies of patients
with intractable temporal lobe epilepsy show hippo-
campal and entorhinal atrophy ipsilateral to the seizure
focus compared with healthy controls, suggesting on-
going cell loss from disruption of a critical hippocampal–
entorhinal connection (Bernasconi et al., 2003).
Direct electrical stimulation studies also support the
critical role of entorhinal cortex in encoding. In rodents,
stimulation of the perforant pathway results in long-term
potentiation, including the resetting of the theta phase,
which has been associated with improved memory out-
comes ( Vertes, 2005; Williams & Givens, 2003; Ehret
et al., 2001; Bliss & Gardner-Medwin, 1973; Bliss & Lomo,
1973). In epilepsy patients undergoing surgical evalua-
tion, stimulation applied to the EC, but not the hippo-
campus, enhanced learning on a spatial navigation task
(Suthana et al., 2012). Likewise, previous fMRI studies
also support the importance of the parahippocampal
structures to verbal associative learning (word–word or
word–face), demonstrating increased activation during
these tasks ( Vilberg & Davachi, 2013; Kirwan & Stark,
2004; Weintrob et al., 2002; Bernard, Desgranges, Platel,
Baron, & Eustache, 2001).
To our knowledge, this is the first study to separately
measure resection extent in the parahippocampal and
entorhinal regions in human participants after epilepsy
surgery and examine their respective contributions to
verbal declarative memory decline. The strengths of this
study include the use of an MRI volumetric tracing method
that precisely quantifies the extent of resection in each
of these medial-temporal subregions. Since memory stabi-
lizes approximately 2 years after surgery (Andersson-
Roswall, Engman, Samuelsson, & Malmgren, 2010; Alpherts
et al., 2006), our length of follow-up has likely captured
patients’ new cognitive baseline.
A limitation of our method for determining resection
extent was that brain shift from pre- to postoperative
images was evident in some participants. This necessi-
tated visual review and manual correction of lesion
masks, which increased the processing time demands.
We utilized MRI scans acquired proximal to surgery to
minimize such error. Thus, it is important to point out that
the lesion masks reflect the extent of tissue resected but
not additional damage that might occur from Wallerian
degeneration (Winston, Stretton, Sidhu, Symms, & Duncan,
2014; Liu, Gross, Wheatley, Concha, & Beaulieu, 2013;
McDonald et al., 2010). Postsurgical white matter changes,
including both degeneration and reorganization, might
impact postsurgical neuropsychological performance
( Yogarajah et al., 2010). However, more sensitive mea-
sures of tissue microstructure, such as diffusion tensor
imaging, are needed to assess this. In summary, although
ongoing postsurgical changes in brain microstructure
might also play an important role in postsurgical memory
performance, our study is limited to assessing the role of
surgical resection extent. In addition, we chose a cortical
parcellation method (Desikan et al., 2006) that achieves
regional specificity while minimizing the multiple com-
parison problem and the impact of coregistration error.
Finer-grained parcellations improve spatial specificity;
however, costs include a higher number of statistical tests
and potentially increased risk of coregistration error in
smaller regions. Future prospective studies would ben-
efit from higher-resolution pre- and postsurgical imag-
ing of the mesial temporal region and finer grained
parcellation of the entorhinal region into perirhinal,
medial, and lateral subregions. Although we did not find
a relationship between hippocampal resection extent
and learning and memory outcomes, this may have
been due to the near complete resection of the hippo-
campus in most patients and the limited range of hippo-
campal resection extent values. A final limitation of our
study is the limited number of patients included, although
878
Journal of Cognitive Neuroscience
Volume 29, Number 5
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
a
/
_
j
0
o
1
c
0
n
8
9
_
a
p
_
d
0
1
b
0
y
8
g
9
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
t
.
f
/
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
our numbers fall within the range of published studies on
surgical cohorts.
These findings may ultimately inform neurosurgical
approaches to reduce cognitive morbidity after epilepsy
surgery. At the very least, these numbers may be helpful
in presurgical counseling to advise patients as to the de-
gree of memory impairment to be expected after surgery.
Our investigation suggests that there is a measurable
decline, on the order of 10–20% decline on a verbal list
learning task, in the majority of patients who undergo a
left temporal lobe resection. Ideally, a larger, multicenter
sample with different surgical approaches could confirm
or refute our findings. In particular, larger participant
numbers are needed to determine if the presence of
mesial temporal sclerosis influences the relationship be-
tween resection extent and memory outcomes. Finally, our
findings support further investigation of stimulation of
perforant pathways to potentially remediate memory
dysfunction.
In summary, we use a precise method of quantifying
surgical resection volumes to discover that degree of left
parahippocampal and entorhinal resection was strongly
correlated with decline in recall or verbal material. These
findings support the growing body of lesion literature in
animals and humans that highlights the critical role of the
perforant structures in declarative memory function.
Acknowledgments
This work was supported by NYU Finding a Cure for Epilepsy
and Seizures (FACES) and the Morris and Alma Schapiro Fund.
Reprint requests should be sent to Anli Liu, NYU Comprehen-
sive Epilepsy Center, New York University School of Medicine,
223 East 34th Street, New York, NY 10016-6402, or via e-mail:
anli.liu@nyumc.org.
REFERENCES
Alpherts, W. C., Vermeulen, J., van Rijen, P. C., da Silva, F. H.,
van Veelen, C. W., & Dutch Collaborative Epilepsy Surgery
Program (2006). Verbal memory decline after temporal
epilepsy surgery? A 6-year multiple assessments follow-up
study. Neurology, 67, 626–631.
Andersson-Roswall, L., Engman, E., Samuelsson, H., &
Malmgren, K. (2010). Cognitive outcome 10 years after
temporal lobe epilepsy surgery: A prospective controlled
study. Neurology, 74, 1977–1985.
Barr, W. B., Goldberg, E., Wasserstein, J., & Novelly, R. A.
(1990). Retrograde amnesia following unilateral temporal
lobectomy. Neuropsychologia, 28, 243–255.
Baxendale, S., Thompson, P., Harkness, W., & Duncan, J.
(2006). Predicting memory decline following epilepsy
surgery: A multivariate approach. Epilepsia, 47, 1887–1894.
Beck, A. T., & Steer, R. A. (1993). Beck Anxiety Inventory
Manual. San Antonio, TX: Psychological Corporation.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck
Depression Inventory-II. San Antonio, TX: Psychological
Corporation.
Bernard, F., Desgranges, B., Platel, H., Baron, J. C., & Eustache,
F. (2001). Contributions of frontal and medial temporal
regions to verbal episodic memory: A PET study.
NeuroReport, 12, 1737–1741.
Bernasconi, N., Bernasconi, A., Caramanos, Z., Antel, S. B.,
Andermann, F., & Arnold, D. L. (2003). Mesial temporal
damage in temporal lobe epilepsy: A volumetric MRI study of
the hippocampus, amygdala and parahippocampal region.
Brain, 126, 462–469.
Bliss, T. V., & Gardner-Medwin, A. R. (1973). Long-lasting
potentiation of synaptic transmission in the dentate area of
the unanaestetized rabbit following stimulation of the
perforant path. Journal of Physiology, 232, 357–374.
Bliss, T. V., & Lomo, T. (1973). Long-lasting potentiation of
synaptic transmission in the dentate area of the anaesthetized
rabbit following stimulation of the perforant path. Journal of
Physiology, 232, 331–356.
Dale, A. M., Fischl, B., & Sereno, M. I. (1999). Cortical surface-
based analysis. I. Segmentation and surface reconstruction.
Neuroimage, 9, 179–194.
Desikan, R. S., Ségonne, F., Fischl, B., Quinn, B. T., Dickerson,
B. C., Blacker, D., et al. (2006). An automated labeling system
for subdividing the human cerebral cortex on MRI scans into
gyral based regions of interest. Neuroimage, 31, 968–980.
Dulay, M. F., & Busch, R. M. (2012). Prediction of
neuropsychological outcome after resection of temporal
and extratemporal seizure foci. Neurosurgical Focus,
32, E4.
Ehret, A., Haaf, A., Jeltsch, H., Heimrich, B., Feuerstein, T. J.,
& Jackisch, R. (2001). Modulation of electrically evoked
acetylcholine release in cultured rat septal neurones.
Journal of Neurochemistry, 76, 555–564.
Eichenbaum, H., Sauvage, M., Fortin, N., Komorowski, R., &
Lipton, P. (2012). Towards a functional organization of
episodic memory in the medial temporal lobe. Neuroscience
and Biobehavioral Reviews, 36, 1597–1608.
Fell, J., Klaver, P., Elger, C. E., & Fernandez, G. (2002). The
interaction of rhinal cortex and hippocampus in human
declarative memory formation. Reviews in the
Neurosciences, 13, 299–312.
Fernández, G., & Tendolkar, I. (2006). The rhinal cortex:
‘Gatekeeper’ of the declarative memory system. Trends in
Cognitive Sciences, 10, 358–362.
Fischl, B., Salat, D. H., Busa, E., Albert, M., Dieterich, M.,
Haselgrove, C., et al. (2002). Whole brain segmentation:
Automated labeling of neuroanatomical structures in the
human brain. Neuron, 33, 341–355.
Fischl, B., Sereno, M. I., & Dale, A. M. (1999). Cortical surface-
based analysis. II: Inflation, flattening, and a surface-based
coordinate system. Neuroimage, 9, 195–207.
Gaffan, D. (1994). Dissociated effects of perirhinal cortex
ablation, fornix transection and amygdalectomy: Evidence for
multiple memory systems in the primate temporal lobe.
Experimental Brain Research, 99, 411–422.
Helmstaedter, C., Grunwald, T., Lehnertz, K., Gleissner, U.,
& Elger, C. E. (1997). Differential involvement of left
temporolateral and temporomesial structures in verbal
declarative learning and memory: Evidence from temporal
lobe epilepsy. Brain and Cognition, 35, 110–131.
Helmstaedter, C., Petzold, I., & Bien, C. G. (2011). The
cognitive consequence of resecting nonlesional tissues in
epilepsy surgery—Results from MRI- and histopathology-
negative patients with temporal lobe epilepsy. Epilepsia, 52,
1402–1408.
Helmstaedter, C., Richter, S., Roske, S., Oltmanns, F., Schramm,
J., & Lehmann, T. N. (2008). Differential effects of temporal
pole resection with amygdalohippocampectomy versus
selective amygdalohippocampectomy on material-specific
memory in patients with mesial temporal lobe epilepsy.
Epilepsia, 49, 88–97.
Liu et al.
879
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
a
/
_
j
0
o
1
c
0
n
8
9
_
a
p
_
d
0
1
b
0
y
8
g
9
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
t
/
.
f
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1
Helmstaedter, C., Roeske, S., Kaaden, S., Elger, C. E., &
Schramm, J. (2011). Hippocampal resection length and
memory outcome in selective epilepsy surgery. Journal of
Neurology, Neurosurgery and Psychiatry, 82, 1375–1381.
Hermann, B. P., Seidenberg, M., Haltiner, A., & Wyler, A. R.
(1995). Relationship of age at onset, chronologic age, and
adequacy of preoperative performance to verbal memory
change after anterior temporal lobectomy. Epilepsia, 36,
137–145.
Josephson, C. B., Dykeman, J., Fiest, K. M., Liu, X., Sadler, R. M.,
Jette, N., et al. (2013). Systematic review and meta-analysis
of standard vs selective temporal lobe epilepsy surgery.
Neurology, 80, 1669–1676.
Kirwan, C. B., & Stark, C. E. (2004). Medial temporal lobe
activation during encoding and retrieval of novel face-name
pairs. Hippocampus, 14, 919–930.
Kuang, Y., Yang, T., Gu, J., Kong, B., & Cheng, L. (2014).
Comparison of therapeutic effects between selective
amygdalohippocampectomy and anterior temporal
lobectomy for the treatment of temporal lobe epilepsy: A
meta-analysis. British Journal of Neurosurgery, 28, 374–377.
Lillywhite, L. M., Saling, M. M., Briellmann, R. S., Weintrob, D. L.,
Pell, G. S., & Jackson, G. D. (2007). Differential contributions
of the hippocampus and rhinal cortices to verbal memory
in epilepsy. Epilepsy & Behavior, 10, 553–559.
Liu, M., Gross, D. W., Wheatley, B. M., Concha, L., & Beaulieu,
C. (2013). The acute phase of Wallerian degeneration:
Longitudinal diffusion tensor imaging of the fornix following
temporal lobe surgery. Neuroimage, 74, 128–139.
Loring, D. W., Lowenstein, D. H., Barbaro, N. M., Fureman,
B. E., Odenkirchen, J., Jacobs, M. P., et al. (2011). Common
data elements in epilepsy research: Development and
implementation of the NINDS epilepsy CDE project. Epilepsia,
52, 1186–1191.
Malkova, L., & Mishkin, M. (2003). One-trial memory for object-
place associations after separate lesions of hippocampus
and posterior parahippocampal region in the monkey.
Journal of Neuroscience, 23, 1956–1965.
McDonald, C. R., Hagler, D. J., Jr., Girard, H. M., Pung, C.,
Ahmadi, M. E., Holland, D., et al. (2010). Changes in fiber
tract integrity and visual fields after anterior temporal
lobectomy. Neurology, 75, 1631–1638.
Morino, M., Uda, T., Naito, K., Yoshimura, M., Ishibashi, K.,
Goto, T., et al. (2006). Comparison of neuropsychological
outcomes after selective amygdalohippocampectomy
versus anterior temporal lobectomy. Epilepsy & Behavior,
9, 95–100.
Murray, E. A., Gaffan, D., & Mishkin, M. (1993). Neural
substrates of visual stimulus-stimulus association in rhesus
monkeys. Journal of Neuroscience, 13, 4549–4561.
Saling, M. M. (2009). Verbal memory in mesial temporal lobe
epilepsy: Beyond material specificity. Brain, 132, 570–582.
Scoville, W. B., & Milner, B. (1957). Loss of recent memory
after bilateral hippocampal lesions. Journal of Neurology,
Neurosurgery and Psychiatry, 20, 11–21.
Sherman, E. M., Wiebe, S., Fay-McClymont, T. B., Tellez-Zenteno,
J., Metcalfe, A., Hernandez-Ronquillo, L., et al. (2011).
Neuropsychological outcomes after epilepsy surgery:
Systematic review and pooled estimates. Epilepsia, 52,
857–869.
Spencer, S., & Huh, L. (2008). Outcomes of epilepsy surgery
in adults and children. Lancet Neurology, 7, 525–537.
Squire, L. R. (1992). Memory and the hippocampus: A synthesis
from findings with rats, monkeys, and humans. Psychological
Review, 99, 195–231.
Squire, L. R., & Zola, S. M. (1996). Structure and function
of declarative and nondeclarative memory systems.
Proceedings of the National Academy of Sciences, U.S.A.,
93, 13515–13522.
Stallings, G., Boake, C., & Sherer, M. (1995). Comparison of the
California Verbal Learning Test and the Rey Auditory Verbal
Learning Test in head-injured patients. Journal of Clinical
and Experimental Neuropsychology, 17, 706–712.
Suthana, N., Haneef, Z., Stern, J., Mukamel, R., Behnke, E.,
Knowlton, B., et al. (2012). Memory enhancement and deep-
brain stimulation of the entorhinal area. The New England
Journal of Medicine, 366, 502–510.
Taylor, E. M. (1959). Psychological appraisal of children
with cerebral defects. Cambridge, MA: Harvard University
Press.
Tellez-Zenteno, J. F., Dhar, R., & Wiebe, S. (2005). Long-term
seizure outcomes following epilepsy surgery: A systematic
review and meta-analysis. Brain, 128, 1188–1198.
Vertes, R. P. (2005). Hippocampal theta rhythm: A tag for
short-term memory. Hippocampus, 15, 923–935.
Vilberg, K. L., & Davachi, L. (2013). Perirhinal-hippocampal
connectivity during reactivation is a marker for object-based
memory consolidation. Neuron, 79, 1232–1242.
Weintrob, D. L. (2004). The neural correlates of memory
impairment in left temporal lobe epilepsy. Unpublished
PhD Thesis. The University of Melbourne.
Weintrob, D. L., Saling, M. M., Berkovic, S. F., Berlangieri, S. U.,
& Reutens, D. C. (2002). Verbal memory in left temporal lobe
epilepsy: Evidence for task-related localization. Annals of
Neurology, 51, 442–447.
Weintrob, D. L., Saling, M. M., Berkovic, S. F., & Reutens, D. C.
(2007). Impaired verbal associative learning after resection of
left perirhinal cortex. Brain, 130, 1423–1431.
Wendling, A. S., Hirsch, E., Wisniewski, I., Davanture, C.,
Ofer, I., Zentner, J., et al. (2013). Selective
amygdalohippocampectomy versus standard temporal
lobectomy in patients with mesial temporal lobe epilepsy
and unilateral hippocampal sclerosis. Epilepsy Research,
104, 94–104.
Williams, J. M., & Givens, B. (2003). Stimulation-induced
reset of hippocampal theta in the freely performing rat.
Hippocampus, 13, 109–116.
Winston, G. P., Stretton, J., Sidhu, M. K., Symms, M. R., &
Duncan, J. S. (2014). Progressive white matter changes
following anterior temporal lobe resection for epilepsy.
NeuroImage. Clinical, 4, 190–200.
Yogarajah, M., Focke, N. K., Bonelli, S. B., Thompson, P.,
Vollmar, C., McEvoy, A. W., et al. (2010). The structural
plasticity of white matter networks following anterior
temporal lobe resection. Brain, 133, 2348–2364.
Zola-Morgan, S., Squire, L. R., Amaral, D. G., & Suzuki, W. A.
(1989). Lesions of perirhinal and parahippocampal cortex
that spare the amygdala and hippocampal formation produce
severe memory impairment. Journal of Neuroscience, 9,
4355–4370.
Zola-Morgan, S., Squire, L. R., Clower, R. P., & Rempel, N. L.
(1993). Damage to the perirhinal cortex exacerbates memory
impairment following lesions to the hippocampal formation.
Journal of Neuroscience, 13, 251–265.
880
Journal of Cognitive Neuroscience
Volume 29, Number 5
D
o
w
n
l
o
a
d
e
d
f
r
o
m
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
h
t
t
p
:
/
D
/
o
m
w
i
n
t
o
p
a
r
d
c
e
.
d
s
f
i
r
o
l
m
v
e
h
r
c
p
h
a
d
i
i
r
r
e
.
c
c
t
.
o
m
m
/
j
e
d
o
u
c
n
o
/
c
a
n
r
a
t
r
i
t
i
c
c
l
e
e
-
p
-
d
p
d
2
f
9
/
5
2
9
8
/
6
5
9
/
1
8
9
6
5
9
2
/
4
1
7
7
7
8
o
6
c
0
n
3
_
1
a
/
_
j
0
o
1
c
0
n
8
9
_
a
p
_
d
0
1
b
0
y
8
g
9
u
.
e
p
s
t
d
o
f
n
b
0
y
8
S
M
e
I
p
T
e
m
L
i
b
b
e
r
r
a
2
r
0
i
2
3
e
s
/
j
t
.
f
/
u
s
e
r
o
n
1
7
M
a
y
2
0
2
1