Open Access Series of Imaging Studies: Longitudinal MRI
Data in Nondemented and Demented Older Adults
Daniel S. Marcus1, Anthony F. Fotenos1, John G. Csernansky2,
John C. Morris1, and Randy L. Buckner3,4,5,6
Abstrait
■ The Open Access Series of Imaging Studies is a series of
neuroimaging data sets that are publicly available for study and
analyse. The present MRI data set consists of a longitudinal collec-
tion of 150 subjects aged 60 à 96 years all acquired on the same
scanner using identical sequences. Each subject was scanned
on two or more visits, separated by at least 1 year for a total of
373 imaging sessions. Subjects were characterized using the Clin-
ical Dementia Rating (CDR) as either nondemented or with very
mild to mild Alzheimerʼs disease. Seventy-two of the subjects were
characterized as nondemented throughout the study. Sixty-four
of the included subjects were characterized as demented at the
time of their initial visits and remained so for subsequent scans,
y compris 51 individuals with CDR 0.5 similar level of impairment
to individuals elsewhere considered to have “mild cognitive
impairment.” Another 14 subjects were characterized as non-
demented at the time of their initial visit (CDR 0) and were subse-
quently characterized as demented at a later visit (CDR > 0). Le
subjects were all right-handed and include both men (n = 62) et
femmes (n = 88). For each scanning session, three or four indi-
vidual T1-weighted MRI scans were obtained. Multiple within-
session acquisitions provide extremely high contrast to noise,
making the data amenable to a wide range of analytic approaches
including automated computational analysis. Automated calcula-
tion of whole-brain volume is presented to demonstrate use of
the data for measuring differences associated with normal aging
and Alzheimerʼs disease. ■
INTRODUCTION
The Open Access Series of Imaging Studies (OASIS) is a
project aimed at making neuroimaging data sets of the
brain freely available to the scientific community. By compil-
ing and freely distributing neuroimaging data sets, we hope
to facilitate future discoveries in basic and clinical neuro-
science similar to other initiatives such as the Alzheimerʼs
Disease Neuroimaging Initiative. The initial OASIS set of
cross-sectional MRI data included over 400 demented and
nondemented individuals across the adult lifespan (Marcus,
Wang, et coll., 2007). Here we describe a longitudinal sample of
MRI data from older adults, with and without Alzheimerʼs dis-
ease (AD). The preparation and release of the data set follows
the rigor established with the initial release: careful quality
control, detailed documentation, example of postprocessed
images, full anonymization, multiple access methods, sur-
going support, and liberal data usage requirements (Marcus,
Wang, et coll., 2007).
The data set includes longitudinal MRI data from 150 dans-
dividuals age 60 à 96 années, y compris 64 individuals with
very mild to moderate AD as diagnosed clinically and char-
acterized using the Clinical Dementia Rating (CDR) scale
(Morris et al., 2001; Morris, 1993) at their initial visit. Another
1Washington University School of Medicine, 2Northwestern Uni-
versity School of Medicine, 3Université Harvard, 4Harvard Médical
École, 5Hôpital général du Massachusetts, 6Howard Hughes Medi-
cal Institute
14 of the individuals were characterized as nondemented
at the time of one or more scans and then clinically deter-
mined to have AD at the time of a subsequent scan. All
data were acquired on the same scanner using identical
procedures. Subjects were screened to eliminate indi-
viduals with psychiatric and neurological conditions that
might contribute to dementia but, where possible, variation
typical of advanced aging was included. Ainsi, many of the
older adults had age-related increases in blood pressure
and a small percentage treated diabetes. Sample charac-
teristics were similar between the individuals with and with-
out AD.
Longitudinal brain imaging has proven useful in studying
normal and diseased aging. Whole-brain volume decline
as measured from longitudinally acquired MRI has been
shown to evolve at a near 0.5% per year (in the range −0.37
to −0.88 across seven reports; Fotenos, Snyder, Girton,
Morris, & Buckner, 2005; Jack et al., 2004; Liu et al., 2003;
Resnick, Pham, Kraut, Zonderman, & Davatzikos, 2003;
Thompson et al., 2003; Wang & Doddrell, 2002; Chan
et coll., 2001) in nondemented older adults, somewhat
greater than that observed in younger adults (Raz et al.,
2005; Liu et al., 2003). The volumes of the whole-brain
and structures associated with memory have been shown
to atrophy at a significantly greater rate in mild cognitive im-
pairment and early AD (par exemple., Dickerson et al., 2006; Fotenos
et coll., 2005; Killiany et al., 2000, 2002; Fox & Freeborough,
1997; Jack et al., 1997; Jack, Petersen, OʼBrien, & Tangalos,
© 2010 Massachusetts Institute of Technology
Journal des neurosciences cognitives 22:12, pp. 2677–2684
D
o
w
n
je
o
un
d
e
d
je
je
/
/
/
/
j
t
t
F
/
je
t
.
:
/
/
F
r
o
m
D
h
o
t
w
t
n
p
o
:
un
/
d
/
e
m
d
je
t
F
r
p
o
m
r
c
h
.
s
p
je
je
d
v
je
e
r
e
r
c
c
t
h
.
m
un
je
r
e
.
d
c
toi
o
o
m
c
/
n
j
un
o
r
c
t
je
n
c
/
e
un
–
p
r
d
t
je
2
c
2
je
e
1
2
–
p
2
d
6
F
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
oui
2
0
g
0
toi
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
F
e
m
b
oui
b
e
r
g
toi
2
0
e
2
s
3
t
/
j
t
.
.
F
.
/
o
n
1
8
M.
un
oui
2
0
2
1
1992). Longitudinal analysis of measures derived from
advanced computational methods, including nonlinear
deformations and shape analysis, have also revealed age-
and disease-associated changes in the brain (par exemple., Buckner
et coll., 2005; Thompson et al., 2003; Wang et al., 2003; Scahill,
Schott, Stevens, Rossor, & Fox, 2002). Longitudinal mea-
sures of brain structure are emerging as tools for tracking
progression of disease and as adjunct outcome measures
in clinical trials (par exemple., Jack et al., in press; Borroni, Premi,
Di Luca, & Padovani, 2007; Chong, Lim, & Sahadevan,
2006; Mueller et al., 2005). The OASIS longitudinal data
set is being made openly available to encourage continued
investigation into aging and disease processes and to sup-
port development of improved methods for studying these
processes.
mentia. Each subject was scanned on two or more sep-
arate occasions, with an average delay of 719 jours (range =
183–1707 days) between visits. The final data set includes
150 subjects and 373 imaging sessions.
Portions of the clinical, demographic, and longitudinal
image data obtained from subjects in this release have
been used in previous publications (Dickerson et al., 2008;
Fotenos, Mintun, Snyder, Morris, & Buckner, 2008; Il,
Chen, & Evans, 2008; Salat et al., 2009; Dickerson et al.,
2009; Buckner et al., 2005; Burns et coll., 2005; Fotenos
et coll., 2005; Head, Snyder, Girton, Morris, & Buckner, 2005;
Buckner et al., 2004; Salat et al., 2004). Many of the subjects
were part of the cross-sectional OASIS data set (Marcus,
Olsen, et coll., 2007; Marcus, Wang, et coll., 2007) but have been
assigned new random identifiers.
MÉTHODES
Sujets
Subjects aged 60 à 96 years were selected from a larger
database of individuals who had participated in MRI studies
at Washington University on the basis of the availability of at
least two separate visits in which clinical and MRI data were
obtained, at least three acquired T1-weighted images per
imaging session, and right-hand dominance. Subjects were
obtained from the longitudinal pool of the Washington
University Alzheimer Disease Research Center (ADRC).
The ADRCʼs normal and cognitively impaired subjects were
recruited primarily through media appeals and word of
mouth, avec 80% of subjects initiating contact with the cen-
ter and the remainder being referred by physicians. All
subjects participated in accordance with guidelines of the
Washington University Human Studies Committee. Ap-
proval for public sharing of the anonymized data was also
specifically obtained.
All subjects were screened for inclusion in this release.
Each subject underwent the ADRCʼs full clinical assessment
as described below. Subjects with a primary cause of de-
mentia other than AD (par exemple., vascular dementia, primaire
progressive aphasia), active neurologic or psychiatric ill-
ness (par exemple., major depression), serious head injury, histoire
of clinically meaningful stroke, and use of psychoactive
drugs were excluded, as were subjects with gross anatomi-
cal abnormalities evident in their MRI images (par exemple., grand
lesions, tumors). Cependant, subjects with age-typical brain
changes (par exemple., mild atrophy, leukoaraiosis) were accepted.
MRI acquisitions typically were obtained within 1 year before
or after a subjectʼs clinical assessment (mean = 111 jours,
range = 0–352 days). Twelve subjects with AD were scanned
after a somewhat longer duration (mean = 653 jours, range =
374–924 days) but were included because each had sev-
eral previous clinical assessments with CDR scores greater
que 0. Two subjects without dementia were scanned some-
what longer than 1 year before a clinical assessment (392
et 431 jours) but were included because their subsequent
clinical assessments continued to indicate no signs of de-
Clinical Assessment
Dementia status was established and staged using the CDR
scale. The determination of AD or nondemented control
status is based solely on clinical methods, without refer-
ence to psychometric performance, and any potential alter-
native causes of dementia (known neurological, medical,
or psychiatric disorders) must not contribute to dementia.
The diagnosis of AD is based on clinical information (de-
rived primarily from a collateral source) that the subject
has experienced gradual onset and progression of decline
in memory and other cognitive and functional domains.
Spécifiquement, the CDR is a dementia-staging instrument that
rates subjects for impairment in each of six domains: mem-
ory, orientation, judgment and problem solving, fonction
in community affairs, home and hobbies, and personal
care. On the basis of the collateral source and subject inter-
voir, a global CDR score is derived from individual ratings
in each domain. A global CDR of 0 indicates no dementia
and a CDR of 0.5, 1, 2, et 3 represent very mild, mild, mod-
erate, and severe dementia, respectivement. These methods
allow for the clinical diagnosis of AD in individuals with a
CDR of 0.5 or greater on the basis of standard criteria that
is confirmed by histopathological examination in 93% de
the individuals (Berg et al., 1998), even for those in the
earliest symptomatic stage (CDR 0.5) of AD who else-
where may be considered to represent “mild cognitive
impairment” (Storandt, Grant, Miller, & Morris, 2006).
Image Acquisition
Pour chaque sujet, three to four individual T1-weighted
magnetization prepared rapid gradient-echo (MP-RAGE)
images were acquired on a 1.5-T Vision scanner (Siemens,
Erlangen, Allemagne) in a single imaging session. Head
movement was minimized by cushioning and by a thermo-
plastic face mask. Headphones were provided for commu-
nication. A vitamin E capsule was placed over the left
forehead to provide a reference marker of anatomic side.
Positioning was low in the head coil (toward the feet) à
2678
Journal des neurosciences cognitives
Volume 22, Nombre 12
D
o
w
n
je
o
un
d
e
d
je
je
/
/
/
/
j
t
t
F
/
je
t
.
:
/
/
F
r
o
m
D
h
o
t
w
t
n
p
o
:
un
/
d
/
e
m
d
je
t
F
r
p
o
m
r
c
h
.
s
p
je
je
d
v
je
e
r
e
r
c
c
t
h
.
m
un
je
r
e
.
d
c
toi
o
o
m
c
/
n
j
un
o
r
c
t
je
n
c
/
e
un
–
p
r
d
t
je
2
c
2
je
e
1
2
–
p
2
d
6
F
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
oui
2
0
g
0
toi
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
F
e
m
b
oui
b
e
r
g
toi
2
0
e
2
s
3
t
/
j
F
t
.
.
.
/
o
n
1
8
M.
un
oui
2
0
2
1
optimize imaging of the cerebral cortex. MP-RAGE param-
eters were empirically optimized for gray-white contrast
(Tableau 1). The scanner and the sequences were maintained
across the duration of the study so the present data are not
influenced by hardware upgrades or other instrument
differences.
Postprocessing
Pour chaque sujet, the individual scan files were converted
from Siemens proprietary IMA format into 16-bit NiFTI1
format using a custom conversion program. Header fields
with identifying information (patient ID, experiment date)
were left blank. The images were then corrected for inter-
scan head movement and spatially warped into the atlas
space of Talairach and Tournoux (1988) using a rigid trans-
formation that differs in process from the original piecewise
scaling. The resulting transformation nonetheless places
the brains in the same coordinate system and bounding
box as the original atlas. The template atlas used here con-
sisted of a combined young-and-old target previously gen-
erated from a representative sample of young (n = 12) et
nondemented old (n = 12) adultes. The use of a combined
template has been shown to minimize the potential bias of
an atlas normalization procedure to overexpand atrophied
brains (Buckner et al., 2004). Given the age range of the
present sample, an old-only atlas target could have been
used. We chose to retain the young-and-old target to be com-
parable to our earlier report (Marcus, Wang, et coll., 2007).
For registration, a 12-parameter affine transformation
was computed to minimize the variance between the first
MP-RAGE image and the atlas target. The remaining
MP-RAGE images were registered to the first (in-plane
stretch allowed) and resampled via transform composition
into a 1-mm isotropic image in atlas space. The result was a
single, high-contrast, averaged MP-RAGE image in atlas
espace. Subsequent steps included skull removal by applica-
tion of a loose-fitting atlas mask and correction for intensity
inhomogeneity because of nonuniformity in the magnetic
field. Intensity variation was corrected across contiguous
regions on the basis of a quadratic inhomogeneity model
fitted to data from a phantom.
Estimated Total Intracranial Volume and
Normalized Whole-brain Volume
The procedures used for measuring intracranial and whole-
brain volumes have been described previously (Fotenos
et coll., 2005; Buckner et al., 2004) and are identical to our
earlier OASIS data release (Marcus, Wang, et coll., 2007). Esti-
mated total intracranial volume (eTIV) was computed by
scaling the manually measured intracranial volume of the
atlas by the determinant of the affine transform connecting
each individualʼs brain to the atlas. This method is mini-
mally influenced and proportional to manually measured
total intracranial volume.
Normalized Whole-brain Volume (nWBV) was computed
using the FAST program in the FSL software suite (www.
fmrib.ox.ac.uk/fsl). The image was first segmented to clas-
sify brain tissue as cerebral spinal fluid, gray, or white matter.
The segmentation procedure iteratively assigned voxels to
tissue classes on the basis of maximum likelihood estimates
of a hidden Markov random field model. The model used
spatial proximity to constrain the probability with which
voxels of a given intensity are assigned to each tissue class.
Enfin, nWBV was computed as the proportion of all voxels
within the brain mask classified as tissue (either gray or
white matter). The unit of normalized volume is percent,
which represents the percentage of the total white and
gray matter voxels within the eTIV (Fotenos et al., 2005).
To calculate atrophy rates, we estimated the slope of the
line connecting nWBV measurements within each individ-
double, divided by baseline nWBV, expressed as percent change
per year. Par exemple, in a participant with two scans, atro-
phy rate was computed as nWBV at Scan 2 minus nWBV at
Scan 1, divided by the interval between measurements, di-
vided by nWBV at Scan 1, times 100. ANCOVA was again
used to test for differences in atrophy rate on the basis of
âge, sex, and dementia status.
Tableau 1. MR Image Acquisition Details
Quality Control
D
o
w
n
je
o
un
d
e
d
je
je
/
/
/
/
j
t
t
F
/
je
t
.
:
/
/
F
r
o
m
D
h
o
t
w
t
n
p
o
:
un
/
d
/
e
m
d
je
t
F
r
p
o
m
r
c
h
.
s
p
je
je
d
v
je
e
r
e
r
c
c
t
h
.
m
un
je
r
e
.
d
c
toi
o
o
m
c
/
n
j
un
o
r
c
t
je
n
c
/
e
un
–
p
r
d
t
je
2
c
2
je
e
1
2
–
p
2
d
6
F
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
oui
2
0
g
0
toi
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
F
e
m
b
oui
b
e
r
g
toi
2
0
e
2
s
3
t
/
j
t
.
.
.
/
F
Sequence
TR (msec)
TE (msec)
Flip angle
TI (msec)
TD (msec)
Orientation
Thickness, gap (mm)
Slice number
Resolution
o
n
1
8
M.
un
oui
2
0
2
1
MP-RAGE
9.7
4.0
10°
20
200
Sagittal
1.25, 0
128
256 × 256 (1 × 1 mm)
All images in the data set were carefully screened for arti-
facts, acquisition problems, and processing errors. During
the screening process, each image was viewed on a per-slice
basis along the axis of acquisition. Typical flaws visible in the
images included electronic noise resulting in bright lines
through multiple slices, motion artifacts appearing as hazy
bands across the image, poor head positioning resulting
in wraparound artifacts, distortions from dental work, et
limited image contrast. Images with severe flaws were ex-
cluded from the data set. A number of borderline images
remain in the distribution, providing tool builders and
testers with a realistic range of acquisition quality. In cases
where individual scans were deemed unusable, the single
scan was removed from the data set but the remainder
Marcus et al.
2679
Tableau 2. Age and Diagnosis Characteristics of Subjects at the Time of Their Initial Visit
Nondemented
Demented
Age Group
60s
70s
80s
90s
N
34
71
41
4
Total
150
n
23
35
26
2
86
Mean
Male
Femelle
Convert
65.71
74.91
84.30
92.50
75.82
6
11
9
0
26
17
24
17
2
59
3
4
7
0
14
n
11
36
15
2
64
Mean
Male
Femelle
CDR 0.5/1
65.67
73.97
82.33
93.00
74.95
8
20
7
1
36
3
16
8
1
29
8/3
29/7
13/2
1/1
52/13
The Convert column indicates individuals who were determined to have AD on a subsequent visit. CDR = Clinical Dementia Rating, avec 0, 0.5, et 1
corresponding to nondemented, very mild, and AD, respectivement. CDR 0.5 individuals may be considered to represent those elsewhere labeled as
“mild cognitive impairment” (MCI).
of the subjectʼs scans was included. Dans l'ensemble, 25 imaging
sessions were excluded from the final release because of
poor image quality.
RÉSULTATS
Overview of the Data Set
The current data set consists of 150 sujets (88 femmes)
âgé 60 à 96 années (Tableau 2). At the time of their initial
visit, 86 had a CDR score of 0, indicating no dementia, et
64 had a CDR score greater than 0 (52 sujets, CDR = 0.5;
13 sujets, CDR = 1; 0 sujet, CDR = 2), indicating a
diagnosis of very mild to moderate AD. Of the subjects
who were initially determined to be nondemented, 14 étaient
later determined to be demented (CDR > 0) at the time of a
subsequent imaging visit. Additional demographics and
clinical characteristics of the subjects are shown in Table 3.
Anatomic Characteristics
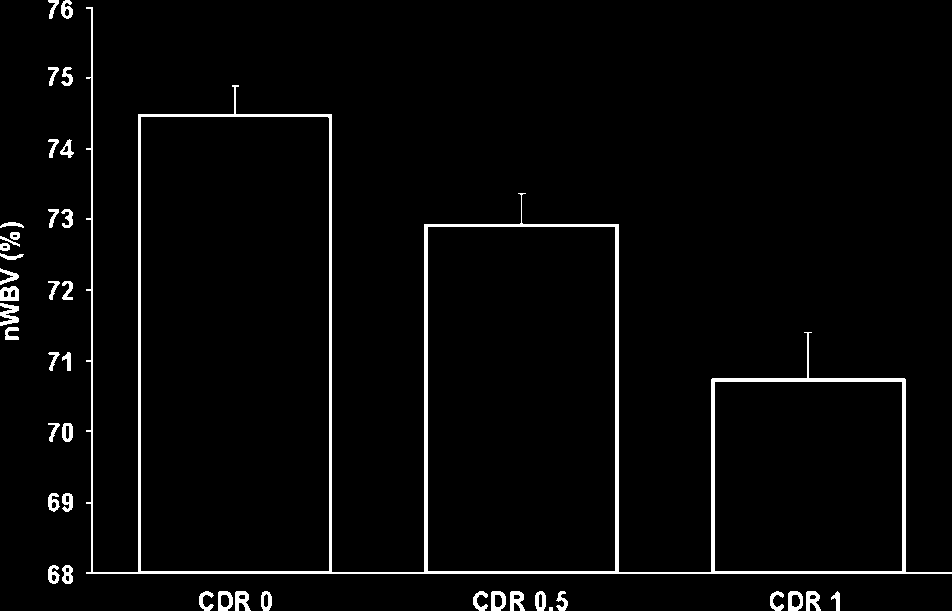
Whole-brain volumes for each of the subjects in the data
set are plotted by age at each visit in Figure 1. Marked de-
creases in nWBV are apparent with age, and nWBV is signifi-
cantly impacted by dementia status (Chiffre 2). Differences
in nWBV between nondemented (CDR 0), very mild de-
mentia (CDR 0.5), and mild dementia (CDR 1) are all sig-
nificant ( p < .01). Whole-brain atrophy rates are shown in
Figure 3 (top). The atrophy rate in nondemented indi-
viduals was −0.49% (SD = 0.56) per year. The atrophy rate
in individuals with DAT was −0.87% (SD = 0.99) per year,
a significant increase compared with nondemented indi-
viduals ( p < .01). For the 14 individuals who declined
from an initial CDR 0 to a CDR 0.5 at the time of their last
scan, the atrophy rate fell between nondemented indi-
viduals and those who entered with AD (−0.69% per year,
SD = 0.62).
Table 3. Sample Characteristics of Subjects
Number
Female/male
Age (years)
Education (years)
MMSE
Prescriptions (n)
Systolic BP (mmHg)
Diastolic BP (mmHg)
Reported HBP (%)
Diabetes (%)
CDR 0
86
60/26
75.8 ± 8.2 (60–93)
15.2 ± 2.7 (8–23)
29.1 ± 0.8 (27–30)
2.9 ± 2.1 (0–9)
135.5 ± 20.3 (98–192)
72.8 ± 10.2 (50–100)
54.6
9.3
CDR 0.5
51
21/30
74.8 ± 6.3 (62–90)
13.6 ± 2.8 (6–20)
26 ± 3.1 (17–30)
3.2 ± 2.4 (0–11)
CDR 1
13
7/6
75.7 ± 8.7 (61–96)
14.0 ± 3.2 (8–20)
23.0 ± 3.3 (19–30)
2.5 ± 2.4 (0–7)
143.5 ± 19.4 (118–188)
143.4 ± 24.9 (90–188)
77.1 ± 10.1 (58–98)
76.9 ± 9.2 (60–88)
46.0
14.0
53.3
13.3
The sample consisted of 150 individuals (72 nondemented, 64 with AD, and 14 who converted over the course of the study). Clinical measures in the
above table were obtained at the clinical assessment closest in date to the initial imaging session, except in 39 cases where these values were not
available until a later visit. Values are presented as mean ± SD. Values in parentheses represent the range. Compared with the nondemented adults,
the older adults with dementia had lower scores on the MMSE ( p < .001) and slightly fewer years of education ( p < .001).
CDR = Clinical Dementia Rating, with 0, 0.5, and 1 corresponding to nondemented, very mild, and mild AD, respectively; MMSE = Mini-Mental State
Examination where scores range from 30 (best) to 0 (worst); HBP = high blood pressure.
2680
Journal of Cognitive Neuroscience
Volume 22, Number 12
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
t
f
r
p
o
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
h
.
m
a
i
r
e
.
d
c
u
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
e
1
2
-
p
2
d
6
f
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
y
2
0
g
0
u
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
f
e
m
b
y
b
e
r
g
u
2
0
e
2
s
3
t
/
j
t
.
.
.
/
f
o
n
1
8
M
a
y
2
0
2
1
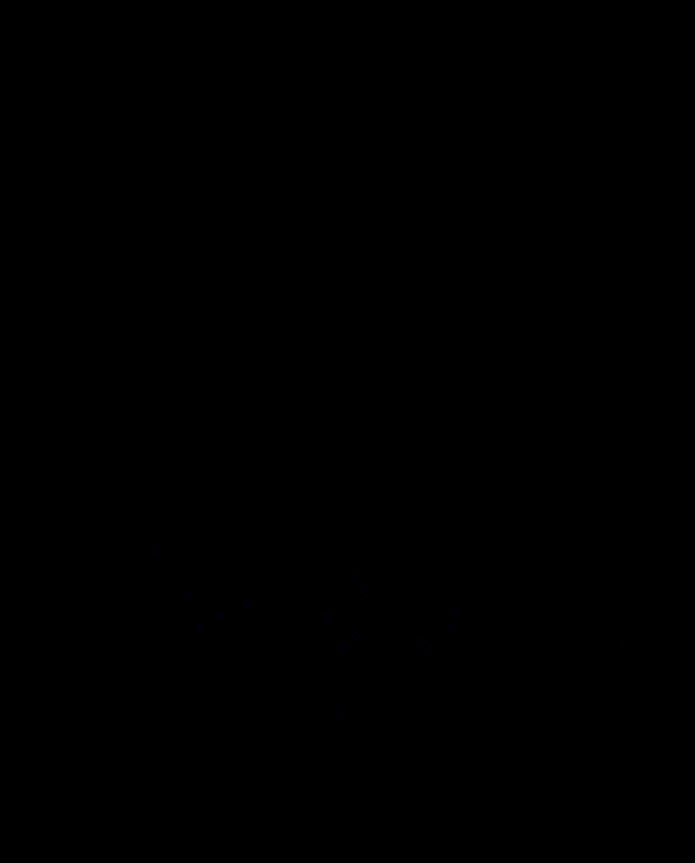
Figure 1. Longitudinal plot of nWBV; lines connect nWBV at
baseline and follow-up scans (or the best fit, for participants with
multiple follow-ups), such that the slope of each line as a proportion
of baseline nWBV represents an individualʼs atrophy rate.
Figure 2. Mean cross-sectional nWBV for all individuals separated
by Clinical Dementia Rating (CDR) (0, 0.5, and 1) at the individualsʼ
initial visit. All differences are significant.
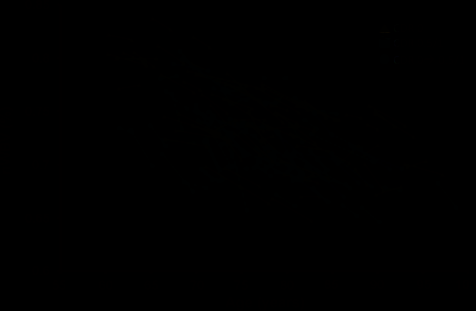
Figure 3. (A) Longitudinal
atrophy rates, expressed in
nWBV loss per year relative
to baseline, are separated by
CDR status at first and last
session. Atrophy rate was
significantly greater for the
group entering the experiment
with very mild dementia
(CDR 0.5 → 0.5/1) than
the group entering without
dementia that remained stable
(CDR 0 → 0), whereas the rate
for the group that manifested
the earliest signs of AD during
the experiment (CDR 0 → 0.5)
fell between those with no
dementia and those who
entered with dementia.
(B) Individual atrophy rates
plotted by age and CDR score.
The trendline is plotted for
CDR 0 → 0.
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
t
f
r
p
o
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
h
.
m
a
i
r
e
.
d
c
u
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
e
1
2
-
p
2
d
6
f
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
y
2
0
g
0
u
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
f
e
m
b
y
b
e
r
g
u
2
0
e
2
s
3
t
/
j
.
.
t
f
.
/
o
n
1
8
M
a
y
2
0
2
1
Marcus et al.
2681
Table 4. Measures Included in the Data Set
Age
Sex
Age at time of image acquisition (years)
Sex (M or F)
Education
Years of education
SES
Socioeconomic status as assessed by the Hollingshead Index of Social Position and classified
into categories from 1 (highest status) to 5 (lowest status) (Hollingshead, 1957)
MMSE
Mini-Mental State Examination score (range is from 0 = worst to 30 = best) (Folstein, Folstein, & McHugh, 1975)
CDR
ASF
eTIV
nWBV
Clinical Dementia Rating (0 = no dementia, 0.5 = very mild AD, 1 = mild AD, 2 = moderate AD) (Morris, 1993)
Atlas scaling factor (unitless). Computed scaling factor that transforms native-space brain and
skull to the atlas target (i.e., the determinant of the transform matrix) (Buckner et al., 2004)
Estimated total intracranial volume (cm3) (Buckner et al., 2004)
Normalized whole-brain volume, expressed as a percent of all voxels in the atlas-masked image that
are labeled as gray or white matter by the automated tissue segmentation process (Fotenos et al., 2005)
Obtaining and Using the Data
OASIS data can be obtained at http://www.oasis-brains.org.
Requests for DVD distributions of the data can be submitted
at the Web site. For convenience, we also provide the data
using the open-source Extensible Neuroimaging Archive
Toolkit (Marcus, Olsen, et al., 2007). It provides tools to
search, to visualize, and to download the data. Before down-
loading and requesting data, users are asked to abide by the
OASIS Data Usage Agreement.
OASIS data are distributed in GNU zip archive files, which
can be uncompressed using freely available software. All
images are distributed in NIFTI1 format (http://nifti.nimh.
nih.gov), which can be visualized and processed using many
common commercial and open source image viewing ap-
plications, including Neurolens, ImageJ, Slicer, and MRIcro.
For each imaging session, the following image files are in-
cluded in the distribution: three to four individual scan
images; an image in which the individual scans have been
aligned and coregistered, an image that has been gain field-
corrected and registered to the Talairach and Tournoux
atlas (T88); a masked T88 image in which the intensity of
all nonbrain voxels has been set to zero; and a segmented
T88 image in which each voxel has been labeled as gray
matter, white matter, or cerebral spinal fluid. Demographic,
clinical, and derived imaging measures (Table 4) are avail-
able in XML and spreadsheet formats. Additional details of
the directory structure, file naming scheme, and image
characteristics can be found at http://www.oasis-brains.
org/longitudinal_facts.html.
DISCUSSION
The present data set includes longitudinally acquired
T1-weighted MRI data from 150 individuals aged 60 to
96 years, including 64 individuals initially determined to
have AD and 14 who were diagnosed with AD at a return
visit. Repeated within-visit acquisitions are included for
each subject allowing extremely high contrast properties
after image averaging. The data have been anonymized,
carefully screened for image quality, and postprocessed
to generate common anatomic measures. The data are
available under a liberal usage policy that allows free access
and unrestricted usage to all interested parties.
The image files included in this OASIS set differ from the
previous OASIS set in two substantive ways meant to im-
prove overall usability. First, the files are in the NiFTI 1 im-
age format, which is now widely supported and preferred
for its more explicit specification of voxel ordering. Second,
the images have not been altered to remove facial features.
This ensures that fiducial markers placed on the left temple
are always present in raw scan images. It also removes hard
edges that may cause difficulty in some segmentation
algorithms.
The specific anatomical measure of nWBV included
here illustrates a common approach to analyzing ana-
tomical characteristics of the brain in MRI images, par-
ticularly in relation to aging. Unsurprisingly, our findings
are in agreement with those described in previous studies
using portions of these data (e.g., Fotenos et al., 2005). In
particular, nWBV was shown to decline significantly with
increasing age and by AD status as previously reported by
Fotenos et al. (2005) and others (Dickerson et al., 2006;
Killiany et al., 2000, 2002; Fox & Freeborough, 1997; Jack
et al., 1992, 1997). Similarly, the rate of nWBV decline was
significantly greater for the AD group than for the non-
demented group.
These findings are representative of the types of analyses
that have been reported in the literature and are not in-
tended to be comprehensive or the final word on how to
approach these data. Such issues as the interplay between
imaging markers, AD, and other diseases (e.g., hyper-
tension, diabetes) remain open avenues for further investi-
gation. Similarly, alternative image processing and statistical
methods may yield additional findings. We hope that the
description and open release of these data will encourage
2682
Journal of Cognitive Neuroscience
Volume 22, Number 12
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
t
f
r
p
o
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
h
.
m
a
i
r
e
.
d
c
u
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
e
1
2
-
p
2
d
6
f
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
y
2
0
g
0
u
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
f
e
m
b
y
b
e
r
g
u
2
0
e
2
s
3
t
/
j
.
.
.
/
t
f
o
n
1
8
M
a
y
2
0
2
1
ongoing exploration of the data, leading to improvements
in the diagnosis and treatment of AD.
Acknowledgments
The authors thank the Washington University ADRC and the
Conte Center for clinical assistance and participant recruitment;
Elizabeth Grant for assistance with data preparation; Susan Larson,
Amy Sanders, Laura Williams, Jamie Parker, and Glenn Foster for
assistance with MRI data collection; Avi Snyder for development of
analytic techniques; and Tim Olsen, Mohana Ramaratnam, Kevin
Archie, and Mikhail Milchenko for development of database and
Web tools. Anders Dale assisted with the original selection of
imaging parameters. The acquisition of this data and the support
for data analysis and management were provided by the National
Institutes of Health grant nos. P50 AG05681, P01 AG03991, R01
AG021910, P20 MH071616, RR14075, RR 16594, and BIRN002;
the Alzheimerʼs Association; the James S. McDonnell Foundation;
the Mental Illness and Neuroscience Discovery Institute; and the
Howard Hughes Medical Institute.
Reprint requests should be sent to Daniel S. Marcus, Department
of Radiology, Campus Box 8225, Washington University School
of Medicine, 4525 Scott Ave., St. Louis, MO 63110, or via e-mail:
dmarcus@wustl.edu.
REFERENCES
Berg, L., McKeel, D. W., Miller, J. P., Storandt, M., Rubin, E. H.,
Morris, J. C., et al. (1998). Clinicopathologic studies in
cognitively healthy aging and Alzheimer disease—Relation
of histologic markers to dementia severity, age, sex, and
apolipoprotein E genotype. Archives of Neurology, 55,
326–335.
Borroni, B., Premi, E., Di Luca, M., & Padovani, A. (2007).
Combined biomarkers for early Alzheimer disease diagnosis.
Current Medicinal Chemistry, 14, 1171–1180.
Buckner, R. L., Head, D., Parker, J., Fotenos, A. F., Marcus, D. S.,
Morris, J. C., et al. (2004). A unified approach for
morphometric and functional data analysis in young, old,
and demented adults using automated atlas-based head
size normalization: Reliability and validation against manual
measurement of total intracranial volume. Neuroimage,
23, 724–738.
Buckner, R. L., Snyder, A. Z., Shannon, B. J., LaRossa, G., Sachs, R.,
Fotenos, A. F., et al. (2005). Molecular, structural, and
functional characterization of Alzheimerʼs disease: Evidence
for a relationship between default activity, amyloid, and
memory. Journal of Neuroscience, 25, 7709–7717.
Burns, J. M., Church, J. A., Johnson, D. K., Xiong, C., Marcus, D.,
Fotenos, A. F., et al. (2005). White matter lesions are
prevalent but differentially related with cognition in
aging and early Alzheimer disease. Archives of Neurology,
62, 1870–1876.
Chan, D., Fox, N. C., Jenkins, R., Scahill, R. I., Crum, W. R., &
Rossor, M. N. (2001). Rates of global and regional cerebral
atrophy in AD and frontotemporal dementia. Neurology,
57, 1759–1763.
Chong, M. S., Lim, W. S., & Sahadevan, S. (2006). Biomarkers
in preclinical Alzheimerʼs disease. Current Opinion in
Investigational Drugs, 7, 600–607.
Dickerson, B. C., Bakkour, A., Salat, D. H., Feczko, E., Pacheco, J.,
Greve, D. N., et al. (2008). The cortical signature of
Alzheimerʼs disease: Regionally-specific cortical thinning
relates to symptom severity in very mild to mild AD
dementia and is detectable in asymptomatic amyloid-positive
individuals. Cerebral Cortex, 19, 497–510.
Dickerson, B. C., Feczko, E., Augustinack, J. C., Pacheco, J.,
Morris, J. C., Fischl, B., et al. (2009). Differential effects
of aging and Alzheimerʼs disease on medial temporal lobe
cortical thickness and surface area. Neurobiology of Aging,
30, 432–440.
Dickerson, B. C., Goncharova, I., Sullivan, M. P., Forchetti, C.,
Wilson, R. S., Bennett, D. A., et al. (2006). Longitudinal
course and neuropathologic outcomes in original vs
revised MCI and in pre-MCI. Neurology, 67, 467–473.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975).
“Mini-mental state”. A practical method for grading the
cognitive state of patients for the clinician. Journal of
Psychiatric Research, 12, 189–198.
Fotenos, A. F., Mintun, M. A., Snyder, A. Z., Morris, M. D.,
& Buckner, R. L. (2008). Brain volume decline in aging:
Evidence for a relation between socioeconomic status,
preclinical Alzheimerʼs disease, and reserve. Archives
of Neurology, 65, 113–120.
Fotenos, A. F., Snyder, A. Z., Girton, L. E., Morris, J. C., &
Buckner, R. L. (2005). Normative estimates of cross-sectional
and longitudinal brain volume decline in aging and AD.
Neurology, 64, 1032–1039.
Fox, N. C., & Freeborough, P. A. (1997). Brain atrophy
progression measured from registered serial MRI:
Validation and application to Alzheimerʼs disease.
Journal of Magnetic Resonance Imaging, 7, 1069–1075.
He, Y., Chen, Z., & Evans, A. (2008). Structural insights into
aberrant topological patterns of large-scale cortical networks
in Alzheimerʼs disease. Journal of Neuroscience, 28,
4756–4766.
Head, D., Snyder, A. Z., Girton, L. E., Morris, J. C., & Buckner, R. L.
(2005). Frontal-hippocampal double dissociation between
normal aging and Alzheimerʼs disease. Cerebral Cortex,
15, 732–739.
Hollingshead, A. (1957). Two factor index of social position.
New Haven, CT: Yale University Press.
Jack, C. R., Jr., Petersen, R. C., OʼBrien, P. C., & Tangalos, E. G.
(1992). MR-based hippocampal volumetry in the diagnosis
of Alzheimerʼs disease. Neurology, 62, 183–188.
Jack, C. R., Jr., Petersen, R. C., Grundman, M., Jin, S., Gamst, A.,
Ward, C. P., Sencakova, D., Doody, R. S., Thal, L. J., & Members
of the Alzheimerʼs Cooperative Study. (2008). Longitudinal
MRI findings from the vitamin E and donepezil treatment study
for MCI. Neurobiology of Aging, 29, 1285–1295.
Jack, C. R., Jr., Petersen, R. C., Xu, Y. C., Waring, S. C., OʼBrien, P. C.,
Tangalos, E. G., et al. (1997). Medial temporal atrophy on
MRI in normal aging and very mild Alzheimerʼs disease.
Neurology, 49, 786–794.
Jack, C. R., Jr., Shiung, M. M., Gunter, J. L., OʼBrien, P. C.,
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
t
f
r
p
o
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
h
.
m
a
i
r
e
.
d
c
u
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
e
1
2
-
p
2
d
6
f
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
y
2
0
g
0
u
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
f
e
m
b
y
b
e
r
g
u
2
0
e
2
s
3
t
/
j
/
.
.
.
t
f
o
n
1
8
M
a
y
2
0
2
1
Weigand, S. D., Knopman, D. S., et al. (2004). Comparison
of different MRI brain atrophy rate measures with clinical
disease progression in AD. Neurology, 62, 591–600.
Killiany, R. J., Gomez-Isla, T., Moss, M., Kikinis, R., Sandor, T.,
Jolesz, F., et al. (2000). Use of structural magnetic resonance
imaging to predict who will get Alzheimerʼs disease.
Annals of Neurology, 47, 430–439.
Killiany, R. J., Hyman, B. T., Gomez-Isla, T., Moss, M. B., Kikinis, R.,
Jolesz, F., et al. (2002). MRI measures of entorhinal cortex vs
hippocampus in preclinical AD. Neurology, 58, 1188–1196.
Liu, R., Lemieux, L., Bell, G. S., Sisodiya, S. M., Shorvon, S. D.,
Sander, J. W., et al. (2003). A longitudinal study of brain
morphometrics using quantitative magnetic resonance
imaging and difference image analysis. Neuroimage, 20,
22–33.
Marcus, D. S., Olsen, T. R., Ramaratnam, M., & Buckner, R. L.
(2007). The Extensible Neuroimaging Archive Toolkit:
Marcus et al.
2683
An informatics platform for managing, exploring, and
sharing neuroimaging data. Neuroinformatics, 5, 11–34.
Marcus, D. S., Wang, T. H., Parker, J., Csernansky, J. G., Morris, J. C.,
& Buckner, R. L. (2007). Open Access Series of Imaging
Studies (OASIS): Cross-sectional MRI data in young,
middle aged, nondemented, and demented older adults.
Journal of Cognitive Neuroscience, 19, 1498–1507.
Morris, J. C. (1993). The Clinical Dementia Rating (CDR):
Current version and scoring rules. Neurology, 43, 2412–2414.
Morris, J. C., Storandt, M., Miller, J. P., McKeel, D. W., Price, J. L.,
Rubin, E. H., et al. (2001). Mild cognitive impairment
represents early-stage Alzheimer disease. Archives of
Neurology, 58, 397–405.
Mueller, S. G., Weiner, M. W., Thal, L. J., Petersen, R. C., Jack, C. R.,
Jagust, W., et al. (2005). Ways toward an early diagnosis in
Alzheimerʼs disease: The Alzheimerʼs Disease Neuroimaging
Initiative (ADNI). Alzheimerʼs & Dementia, 1, 55–60.
Raz, N., Lindenberger, U., Rodrigue, K. M., Kennedy, K. M.,
Head, D., Williamson, A., et al. (2005). Regional brain
changes in aging healthy adults: General trends, individual
differences and modifiers. Cerebral Cortex, 15, 1676–1689.
Resnick, S. M., Pham, D. L., Kraut, M. A., Zonderman, A. B., &
Davatzikos, C. (2003). Longitudinal magnetic resonance
imaging studies of older adults: A shrinking brain.
Journal of Neuroscience, 23, 3295–3301.
Salat, D. H., Buckner, R. L., Snyder, A. Z., Greve, D. N.,
Desikan, R. S. R., Busa, E., et al. (2004). Thinning of the
cerebral cortex in aging. Cerebral Cortex, 14, 721–730.
Salat, D. H., Greve, D. N., Pacheco, J. L., Quinn, B. T., Helmer, K. G.,
Buckner, R. L., et al. (2009). Regional white matter volume
differences in nondemented aging and Alzheimerʼs disease.
Neuroimage, 15, 1247–1258.
Scahill, R. I., Schott, J. M., Stevens, J. M., Rossor, M. N., & Fox, N. C.
(2002). Mapping the evolution of regional atrophy in
Alzheimerʼs disease: Unbiased analysis of fluid-registered
serial MRI. Proceedings of the National Academy of
Sciences, U.S.A., 99, 4703–4707.
Storandt, M., Grant, E. A., Miller, J. P., & Morris, J. C. (2006).
Longitudinal course and neuropathologic outcomes
in original vs revised MCI and in pre-MCI. Neurology,
67, 467–473.
Talairach, J., & Tournoux, P. (1988). Co-planar stereotaxic
atlas of the human brain: An approach to medical cerebral
imaging. New York: Thieme.
Thompson, P. M., Hayashi, K. M., de Zubicaray, G., Janke, A. L.,
Rose, S. E., Semple, J., et al. (2003). Dynamics of gray matter
loss in Alzheimerʼs disease. Journal of Neuroscience, 23,
994–1005.
Wang, D. M., & Doddrell, D. M. (2002). MR image-based
measurement of rates of change in volumes of brain
structures. Part 1: Method and validation. Magnetic
Resonance Imaging, 20, 27–40.
Wang, L., Swank, J. S., Glick, I. E., Gado, M. H., Miller, M. I.,
Morris, J. C., et al. (2003). Changes in hippocampal volume
and shape across time distinguish dementia of then Alzheimer
type from healthy aging. Neuroimage, 20, 667–682.
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
t
f
r
p
o
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
h
.
m
a
i
r
e
.
d
c
u
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
e
1
2
-
p
2
d
6
f
7
/
7
2
1
2
9
/
4
1
0
2
1
/
7
2
2
6
o
7
c
7
n
/
2
1
0
7
0
7
9
0
8
2
4
1
4
8
0
/
7
j
o
p
c
d
n
.
b
y
2
0
g
0
u
9
e
.
s
t
2
o
1
n
4
0
0
7
8
.
S
p
e
d
p
f
e
m
b
y
b
e
r
g
u
2
0
e
2
s
3
t
/
j
f
.
.
t
.
/
o
n
1
8
M
a
y
2
0
2
1
2684
Journal of Cognitive Neuroscience
Volume 22, Number 12