Marc J. Epstein and Eric G. Bing
Delivering Health Care to the Global Poor:
Solving the Accessibility Problem
Chaque année, environ 8.1 million children around the world die before they can
celebrate their fifth birthday.1 A child in a developing country is 33 times as likely
to die before age five as a child in the industrialized world, and up to 60 percent of
these deaths could be prevented through basic health education, des produits, et
services, including low-cost treatments that are readily available in developed
countries.2 Adults are also dying of illnesses that have largely been eradicated in
developed countries and could be prevented using low-cost interventions that are
often available within the country, but are not accessible to those who need them,
and not in sufficient amounts.3
In comparisons of industrialized and developing countries, the lack of finan-
cial resources partially accounts for the differential mortality rates. Cependant, many
prevention and treatment strategies for easily treatable conditions have been made
available to developing countries by local and international governmental and
non-governmental organizations (NGOs). Dans 2007 alone, these entities provided
Marc J. Epstein is Distinguished Research Professor of Management at Jones Graduate
School of Business at Rice University in Houston, Texas, and an expert on sustainabil-
ville, gouvernance, performance measurement, and accountability in both corporations
and nonprofit organizations. He is working in developing countries in Africa, Asia,
and South America on microfinance, entrepreneurship, and education, and on com-
mercializing and disseminating low-cost health technologies. All the students in his
MBA course travel with him to Rwanda or Liberia to work on commercializing health
technologies for the poor.
Eric G. Bing is the Director of Global Health at the George W. Bush Institute in Dallas,
Texas, and Endowed Professor of Global Health at the Charles Drew University of
Medicine and Science in Los Angeles. He has developed and implemented disease sur-
veillance, prevention, care, treatment, and research programs in Africa, le
Caribbean, and Central America. In his current position he partners with others to
turn innovative ideas into practical health-care solutions that can be tested, imple-
mented, and scaled, and focuses on social entrepreneurship and women’s and family
health issues in developing countries.
© 2011 Marc J. Epstein and Eric G. Bing
nouveautés / volume 6, number 2
117
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
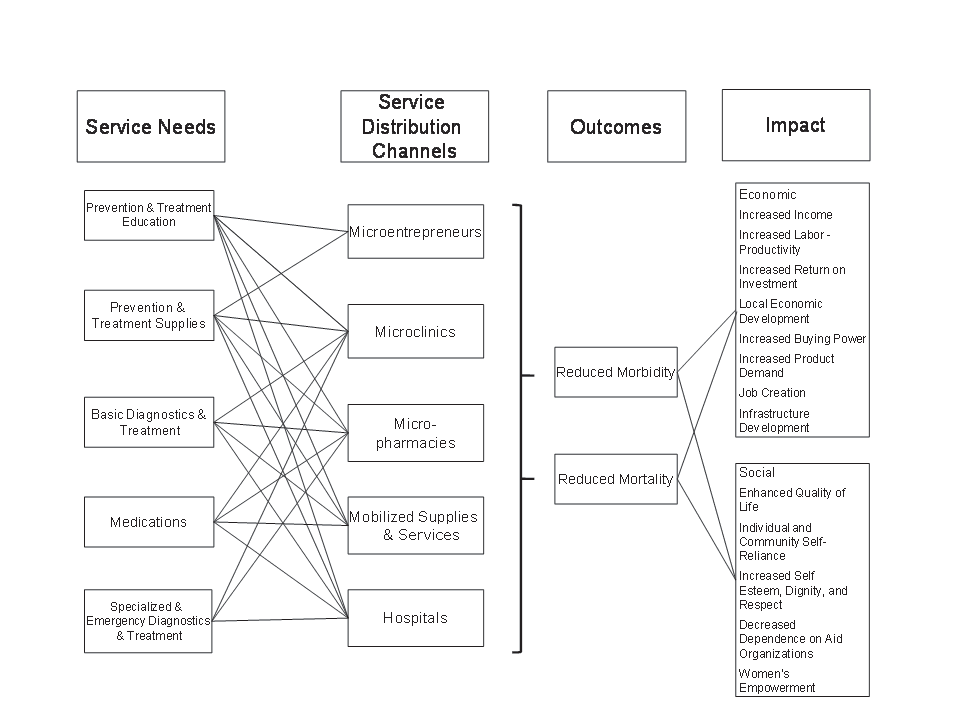
$21.1 billion for health-related projects in developing countries4—but interven- tions frequently do not reach the poorest and most vulnerable. Developing coun- tries lack delivery systems that can give their populations access to health informa- tion, health technologies, and services, and to high-quality and affordable medica- tion. In developing countries, health care often relies on both the public and private sectors. Malheureusement, these sectors are often poorly coordinated, regulated, and supported, resulting in gaps in services, lost opportunities, and unsustainable sys- thèmes. Souvent, the public health sector has inadequate resources and must address a host of public health issues, including disease surveillance and prevention, devel- opment of evidence-based policies, oversight of health providers, and enforcement of public health regulations. En outre, it must staff and oversee an array of hos- pitals, clinics, laboratories, and pharmacies throughout the country. In many developing countries, the private sector is robust and a critical part- ner in providing care. A recent report noted that the private sector funds 60 par- cent of all health care in sub-Saharan Africa.5 Moreover, 50 percent of all health- care expenditures in that region go to the private sector.6 The private sector’s sup- port for and involvement in providing health care to developing nations has been controversial because of concerns that increased privatization may divert resources away from the public sector and that quality controls for private care are not in place.7 While there are many examples of low-quality and even hazardous servic- es within both the public and private sectors,8 the private sector has helped improve care overall in developing countries, including helping reduce the health disparities that result from differences in income levels and geographic settings.9 Like their wealthier counterparts, developing countries will benefit from strong public and private sectors that have adequate resources, and are integrated and regulated so that health-care programs are cost-effective, scalable, financially sustainable, safe, and trusted. Dans ce document, we describe innovative private pro- grams in distribution channels that have the potential to help bridge the gap in care. We then propose a model that integrates the public and private sectors. THE DISTRIBUTION CHANNELS Improving access to essential health information, des produits, and services requires multiple and complementary distribution channels to reach consumers in low- income settings. Chiffre 1 shows five distribution channels: microentrepreneurs, microclinics, micropharmacies, mobile distribution of supplies and services, and hospitals. The products and services we describe within these channels are already being used in many low-resource settings. They complement governmental and nongovernmental programs and enhance access to health-care products and serv- ices. Cependant, they are often isolated components and not integrated into a com- prehensive health-care system. Even where they are integrated, they have not been taken to scale in order to maximize cost efficiency, financial sustainability, and reach. 118 nouveautés / Meaningful Markets Downloaded from http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Delivering Health Care to the Global Poor Figure 1. Health Distribution Model Microentrepreneurs Low-cost interventions that can prevent acute and chronic medical conditions and death are quite cheap when compared to the wages, skills, and other resources that individuals and communities lose when people are ill or die. Health projects are often inexpensive to produce and require little training to disseminate. Microentrepreneurs can often distribute basic health supplies effectively because they understand the needs and financial restrictions of the local community10 and have become advocates of disease prevention and health care in their communi- liens. Microentrepreneurs have financial incentives to serve as both health educators and distributors: they earn the trust of customers, build demand for products, and earn income. Aligning the incentives for microentrepreneurial success with the goal of increasing access can help bring the first point of disease prevention and health-care services closer to those in need in low-resource settings. Microclinics Unlike microentrepreneurs, who generally have no medical background, micro- clinics are often franchises that provide basic medical care for a short list of com- mon and preventable diseases. They tend to be staffed by providers, such as com- munity health nurses, who have received formal training to provide appropriate innovations / volume 6, number 2 119 Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Marc J. Epstein and Eric G. Bing care that is consistent and of high quality. Some microclinics also contain micropharmacies and distribute medication. Efforts to align clinicians’ profits with the goal of improved delivery have helped microclinics discover efficient ways to bring diagnosis and treatment closer to those in rural areas. Micropharmacies When medications are prescribed appropriately, they can maintain or restore health. Cependant, if they are improperly prescribed and administered, rates of ill- ness and death can rise, antibiotic-resistant strains of infectious diseases can spread, and community trust in the health-care delivery system can diminish. For this reason, an emphasis has been placed on having trained clinicians or pharma- cists prescribe and distribute medications. Aligning financial incentives with improving access to basic medications to the poor will strengthen the overall health-care delivery system. Mobile Distribution of Supplies and Services Poor infrastructure can place great strains on the supply chains for health-care providers in developing countries. When the poor, particularly those in rural and remote settings, try to access health care, providers cannot always serve them because they do not always have the necessary supplies. Delivering supplies to patients, providers, or distributors—using small cars, vans, trucks, motorcycles, or even bikes—is an important bridge in supply chains; drivers can even deliver prod- ucts directly to consumers when needed. Vehicles can also bring trained health- care providers to remote and rural areas that would otherwise be unable to attract or retain them. Hospitals For more advanced treatment and emergency care, people in low-resource settings need access to hospitals. By shifting some of the burden for basic and routine pre- vention and care to franchised and other clinics and pharmacies, hospitals could focus their attention on the most complex cases. Doing so would relieve stress on the commonly overcrowded and understaffed public hospitals in developing coun- tries. EXAMPLES OF INNOVATIVE IMPLEMENTATION In this section we provide examples of these five kinds of distribution channels. Microentrepreneurs and Health Workers Microentrepreneurs, the owners of small businesses in low-resource settings, are particularly well positioned to deliver health products and services to rural com- munities. In some developing countries, such businesses employ more than half of the workforce.11 They already operate in remote areas, understand the cultural intricacies needed to market products, and have personal connections with their 120 nouveautés / Meaningful Markets Downloaded from http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Delivering Health Care to the Global Poor customers. In addition, over 100 million of these businesses receive loans from microfinance institutions (MFIs) every year, which can help them increase their businesses.12 Given the estimated $87.7 billion market for health products and
services in developing countries, there is great potential for health products to pro-
vide both income to microentrepreneurs and a service to communities.13
Private nonprofit and for-profit organizations that supply financial services to
the rural poor have recognized the potential, in both financial and social benefits,
for their clients to sell health products in the poor communities at the bottom of
the pyramid.14 Many have supplied their clients with items to sell to community
members: health kits consisting of rudimentary first aid supplies, insecticide-treat-
ed mosquito nets (to prevent malaria), and oral rehydration therapy (to treat diar-
rhea). Entrepreneurs need little training to sell many of these basic health prod-
ucts, except skills as sales representatives; with such training, they can promote and
market these products more effectively.
Freedom from Hunger (FFH) is an NGO with programs in 16 countries that
has reached over one million women. It supplies entrepreneurs in Ghana with an
assortment of products to sell in their communities, most notably in their Micro
Business for Health program. Women in this program operate as microfrancisees,
also called healthkeepers, who sell health products door to door. FFH trains its
members to teach customers how to hang bed nets to prevent malaria, to use con-
traceptives, and to recognize if a child is dehydrated. The women earn commis-
sions on the products they sell and pay fees to FFH. For those already selling prod-
ucts, this program has already proven profitable. They have served over 16,000
people in rural Ghana, with a goal of reaching 80% of Ghana’s rural population by
2012.15
VisionSpring is an NGO performing similar work, but its focus is on eye care.
Because sight affects people’s efficiency in performing even the most basic tasks,
those who need glasses can see a 27-fold return on their investment when they buy
a pair of non-prescription reading glasses. Because it is such a cost-effective pur-
chase for both consumers and business people, VisionSpring can sell its product
profitably in developing countries. The NGO has given entrepreneurs the oppor-
tunity to establish a business and earn an income by selling glasses and providing
basic eye care. In a three-day training program, the microentrepreneurs learn the
basics of eye care; they also learn how to sell their services door to door in their
communautés. VisionSpring provides the business supplies on consignment to its
members; in return they pay a set price for the glasses they sell. VisionSpring owns
inexpensive branded glasses in seven countries across three continents. Dans le passé
decade it has sold over 230,000 pairs of glasses through 863 entrepreneurs.16
Living Goods, another NGO operating in Uganda, offers microentrepreneurs
the option to become franchisees. Microentrepreneurs receive a health kit at a cost
ranging between $100 et $250. The kit contains products for preventing sexual-
ly transmitted infections (STIs) and malaria and other products for maintaining
basic hygiene, including soap and shampoo. The microfranchisees sell these prod-
ucts for a small profit in their communities and meanwhile help to prevent and
nouveautés / volume 6, number 2
121
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
treat some serious infections, including diarrhea and intestinal parasites. Because
some cannot afford the startup costs for this business, BRAC (Bangladesh Rural
Advancement Committee), one of the world’s largest microfinance institutions,
has partnered with Living Goods to offer its clients loans to enter the business.17
Soluciones Comunitarias (SolCom) is a Guatemalan microenterprise that uses
the microconsignment model. It identifies, trains, and supports rural entrepre-
neurs who sell a variety of basic products, including eyeglasses, water filters, light
bulbs, and seeds. In this model, entrepreneurs only pay for the products they sell,
and return the rest—which removes much of the financial risk. This setup allows
them to experiment more freely with a variety of products and diversify their
product portfolio, which also lowers their risk.18
Hindustan Unilever Limited (HUL) is one of India’s largest companies. Its
microfranchising program, Project Shakti, provides a business model for more
que 40,000 female microentrepreneurs in India, most of them poor and illiterate.
HUL has helped double the income of many of its participants. The additional $12 per month that these women earn can make a tremendous difference in their lives. As in the programs run by Living Goods and FFH, women earn profits on their sales. Unlike the other programs, cependant, HUL is a for-profit company, and it operates this program under its corporate social responsibility (CSR) program. Project Shakti may bring the company significant profits; it is expected to contin- ue to contribute between $27 et $45 million to HUL’s bottom line.19 While many organizations, including Partners in Health (PIH), have promot- ed the use of community health workers (CHWs) to deliver basic health products, CHWs are often paid by the NGOs or governments or represent community vol- unteers. While these services are important, the programs require substantial ongoing governmental or NGO investments in training, management, supervi- sion, and logistics.20 Nonprofit organizations that provide free health services (similar to CHW programs) have developed an important model for delivering health care in low- resource settings. Providing basic health supplies for free, cependant, fails to meet the test of long-term financial sustainability. En outre, these programs may inadver- tently foster dependence, and programs may fail to scale up their efforts and reach larger populations. Microentrepreneurship can provide a more robust and sustain- able model for delivering basic health-care products, éducation, and services to consumers in developing countries. Encouraging microentrepreneurs to deliver these basic interventions can be cost effective because they often require little training and can recycle the money they make from their enterprises back into ordering more health supplies for their communities. FFH, Vision Spring, Living Goods, SolCom, and HUL have shown that by aligning the incentives of the entre- preneur with the goal of improved health-care distribution, businesses and organ- izations can better serve both their customers and their communities. These pro- grams have also proven to be scalable and sustainable. Surtout, they have suc- cessfully merged commerce with community service and found replicable success in bringing health care to the poor. Microentrepreneurs are typically not health 122 nouveautés / Meaningful Markets Downloaded from http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Delivering Health Care to the Global Poor professionals, but they can serve an important role in preventing and treating basic diseases. Microclinics The HealthStore Foundation operates CFW (Child and Family Wellness) shops, which are franchised clinics managed by nurses. They focus primarily on distrib- uting treatments for the medical conditions that cause 70 percent to 90 percent of child morbidity and mortality in developing countries; the nurses can provide additional primary care services if needed. These microclinics have proven highly successful and now account for 48 of the 65 CFW shops in Kenya, providing over $1,000 per month in income for the nurses who operate them.21
MicroClinic, a similar franchising organization operating in West Africa, uses
microfinance lending practices to provide community health-care workers, nurs-
es, and doctors the opportunity to start clinics in suburban and rural areas.
MicroClinic operates on a hub-and-spokes model: clinics are connected to a main
hospital or distribution center to receive goods, but they operate independently.
The franchisors strictly monitor the quality of services and the performance of
franchisees. MicroClinics, like CFW shops, focus specifically on treating the most
ravaging diseases in their communities, including HIV/AIDS, malaria, tuberculo-
sis, and perinatal conditions. Franchisees supply the community with general
health-care items and help to maintain the health of all community members.
Depending on their training, franchisees may perform minor surgery. MicroClinic
supports the franchisees through training, certification for health practices, et
loans to start and expand their clinics.22
An Indian NGO, Janani, has also franchised clinics to doctors in two rural
states of India. It has trained over 800 doctors to offer reproductive surgeries and
clinical services, and currently has 172 active franchisees. This program has
emerged through partnerships between the Indian government and Janani, et
has become a cost-efficient service delivery system. Each franchisee pays a yearly
franchise fee to use the Janani brand and receive logistical support; à son tour, clients
are drawn to their high quality and low prices. Since 1996, by increasing their out-
reach in two of India’s poorest provinces, Janani-trained doctors have performed
close to 500,000 procedures, and provided family products and services to over
12.5 million couples.23
New providers are emerging across the developing world to help bring more
affordable, sustainable care to rural populations through clinics and health-care
centres. One Indian company, Electronic Health Point (EHP), has launched a pro-
gram in Punjab that provides comprehensive health services to rural villages.
EHP’s products and services include pharmaceuticals, advanced diagnostics,
telemedical consultations with doctors in urban areas, and clean water. Because
EHP provides clean drinking water, it has daily contact with many of its customers
and can play a key role in raising awareness about health issues in its communities.
Three EHP clinics are currently in operation, and plans are to scale-up rapidly.
nouveautés / volume 6, number 2
123
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
Micropharmacies
Micropharmacies help to extend access to pharmaceuticals and ensure that high-
quality medicines are delivered to communities that would otherwise get few or no
such supplies. Many of the treatments that can alleviate common diseases in devel-
oping countries need not be provided by doctors; trained pharmacists can often
distribute medicines at lower cost. Many companies franchise pharmacies in devel-
oping countries, allowing pharmacists to sell the treatments for diseases that have
long been the scourges of their communities. These medical entrepreneurs require
training and must meet certain quality standards. Because medications can sicken
and even kill people if not properly administered, it is crucial to ensure that these
products are of high quality and are distributed appropriately.
Customers at pharmacies in developing countries must trust their pharmacists
because the regulatory framework to protect drug quality does not always exist in
low-resource settings. As counterfeiting is a significant concern in developing
des pays, consumers need to know that the medications they are receiving are of
high quality. In Nigeria, for example, almost half of all medicines did not meet
WHO quality standards in 2004. While there have been significant successes in
increasing drug quality in Nigeria, the poor will not seek care if they do not trust
it to serve their needs.24
Successful pharmacies can provide essential medications to treat or cure dis-
eases in early stages and thus decrease morbidity and the need for more expensive
clinical care. Two organizations, CareShop Ghana and the HealthStore
Fondation, have developed distribution systems that make drugs accessible and
provide a brand that customers can trust. These two organizations have successful-
ly franchised these pharmacies to entrepreneurs who serve their communities.
Dans 2002, the nonprofit Ghana Social Marketing Foundation founded CareShop
Ghana as a wholly owned for-profit subsidiary. CareShop franchises pharmacies
that are already in operation. Rather than try to assist entrepreneurs in starting up
pharmacies, CareShop converts existing drug retailers within Ghana to CareShops;
this helps support brand identity and ensure product quality. CareShop supports
the franchisee through training programs specialized to fit the needs of the com-
munity by providing information on essential medications and treatments. Ce
approach has become an effective part of the business model. With more knowl-
bord, franchisees can strengthen their businesses. In its seven-year history,
CareShop Ghana has franchised 276 independent outlets. While it has relied on
loans and grants to fill funding gaps, it has succeeded in avoiding supply chain dis-
ruptions and has reduced the costs of operating pharmacies. Since its founding, it
has distributed more than 60,000 units of malarial medications and more than
800,000 condoms.25
HealthStore Foundation has also proven successful using similar methods
through its Child and Family Wellness (CFW) Shops, a micropharmacy program
in Kenya and Rwanda that lends money to entrepreneurs to help them start CFW
franchises. It operates this program in addition to the microclinic program men-
124
nouveautés / Meaningful Markets
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Delivering Health Care to the Global Poor
tioned above. HealthStore Foundation mandates quality control and a rigorous
training program, but also negotiates drug prices and keeps detailed medical
records for franchisees, helping them to drastically reduce costs. This business
model has contributed to the approximately $600 à $800 monthly incomes of the
community health worker franchisees. While its franchising entity in Rwanda
remains an NGO, this organization is currently restructuring to make the fran-
chisor in Kenya a for-profit subsidiary of HealthStore. HealthStore hopes that this
approach will make it more sustainable and scalable. The foundation has 87 CFW
shops and is growing rapidly.26
As in the other microfranchising programs, pharmacy franchisees own their
businesses and earn sustainable income for their families. The franchisor lowers
the prices that patients pay for pharmaceuticals by purchasing for all of its fran-
chisees and exploiting its larger buying power. Both of these organizations demon-
strate the potential of merging commercial and nonprofit models of health-care
delivery, and their methods should serve as a guide for those looking to scale-up
quality drug distribution in developing countries.
Franchisees require prior training on the basic treatment of common illnesses,
the pharmacology of commonly sold medications, and details of medication
dosage and use. The pharmacist, cependant, does not need the same experience or
training in diagnosing advanced diseases or illnesses as a primary care provider.
Pharmacies typically only provide basic information on diseases, mostly pertain-
ing to patients’ medications. Although they require less training, they are also lim-
ited in the services they can provide. Even for primary health care, patients often
must see a doctor or nurse.
Microclinics and micropharmacies may not necessarily be close to patients’
residences. Plus que 80 percent of Africa’s populated areas are over 100 kilome-
ters from a body of water or navigable river,27 and governments often cannot afford
to maintain or expand road systems. By using local personnel, including microen-
trepreneurs, pharmacists, and clinicians, health systems can reach many of the
poorest.
Mobilized Delivery of Supplies and Treatment
Motorized vehicles must be used, cependant, to bridge the gaps in supply chains that
plague many communities in developing countries. Trucks and motorcycles can
ensure that providers have consistent access to supply distributors; this becomes
especially crucial in addressing illnesses like tuberculosis or HIV/AIDS. Patients
with these infections need consistent access to care and treatment to avoid antibi-
otic and antiretroviral resistance. If motor vehicles can be used to keep supply
chains operating, they may also help to slow both the progression and spread of
maladie, and drug resistance in the developing world.
It would be expensive to place highly-trained health-care workers in every
small community across the developing world. Mobilization has been used to
bring more advanced points of care to the rural poor. Clinicians and doctors have
nouveautés / volume 6, number 2
125
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
donned backpacks and satchels filled with tools to diagnose and treat diseases in
rural areas that are not accessible by car. Some NGOs have tried to move more
advanced points of care to the rural poor by using motorcycles and other modes
of rapid transportation. In Zimbabwe, one such program, Riders for Health, a
reached five times as many patients using motorcycles as it has on foot.28 Riders for
Health uses motorized vehicles to bridge links in strained supply chains in devel-
oping countries, allowing health providers to visit more patients, move further
into rural regions, and respond more rapidly to medical emergencies.29 It charges
government health ministries and other NGOs a small fee to train their health-care
workers in motorcycle maintenance and to perform regular, scheduled mainte-
nance. This model can significantly reduce repair costs and help ensure that
health-care workers can consistently reach their patients.30 The African Infectious
Disease Village Clinics (AIDVC) is an NGO that uses the mobile support systems
of Riders for Health from a central building in Kenya to provide health care to
plus que 90,000 patients. It also uses Riders for Health transportation to train
community members to deliver health-care treatments to more patients using a
relatively small number of staff.31
Mobilization has greatly facilitated the distribution of health-care supplies and
allowed health-care workers to serve larger communities. Cependant, distributing
health supplies and care is often inefficient. Systems trying to serve large numbers
of patients from a central location may not leverage resources effectively without
intervening support structures. En outre, unless they operate at scale, they may
never become financially sustainable. These projects have succeeded in bringing
improved health care to the rural poor. To stretch scarce resources further, mobile
treatment must be further integrated into the overall health-care system, and be
used in conjunction with existing infrastructure (par exemple., CFW shops, microclinics,
CareShops). Par exemple, franchise pharmacists and clinicians or their staff could
drive trucks to help deliver treatments to their patients. Because these workers
often serve and earn their livelihoods by serving these smaller communities, ils
can provide health-care services more effectively.
Hospitals
Hospitals are large care centers that must be responsible for advanced and complex
treatment, but not necessarily for providing less expensive, basic medical supplies
to patients. Much of the burden for hospitals in developing countries could be alle-
viated through more effective distribution systems for products and services, as we
have described. Hospitals must be integrated into the larger distribution system
and able to refer patients to microclinics, micropharmacies, and entrepreneurs in
patients’ communities if they are to make effective use of their highly trained
employees and their limited space. They must also shift the burden of care to oth-
ers as much as possible, to make the best use of their expensive and skilled facili-
ties and personnel. The integrated system we suggest offers many outlets for such
shifts. Par exemple, patients can see clinicians, pharmacists, or even microentre-
126
nouveautés / Meaningful Markets
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Delivering Health Care to the Global Poor
preneurs for most of their needs; only for the most complex and unusual cases do
they need a hospital. Making sure the poor have other available resources to receive
primary health care is an important step toward integrating hospitals into a com-
prehensive distribution system.
One way to expand access to hospital care in the developing world is to reduce
costs and improve efficiency. The Aravind Eye Care System, a group of hospitals
that has revolutionized cataract surgery in India, is one example of how efficiency
gains can drive improved health outcomes in hospitals and significantly improve
dissemination. Nine million Indians are blind, and many more have eye impair-
ments that can be treated with surgery. At Aravind hospitals, each staff physician
performs an average of 2,600 cataract surgeries per year—more than six times the
average for hospitals in India. This drives down costs significantly: while a cataract
surgery may cost between $2,600 et $3,000 in the United States, Aravind can per-
form the procedure for between $50 et $100. En outre, it does over 60% de
procedures at no cost for poor patients. These factors allow the five Aravind hos-
pitals in Tamil Nadu province to perform nearly 200,000 cataract surgeries every
year.32
Despite the low costs and number of free surgeries that Aravind doctors per-
formulaire, the business still operates at a profit. It manufactures many of its own surgi-
cal supplies and materials, thereby often lowering costs to 5% of the price of com-
parable imports. Aravind also exports some of the lenses it manufactures. Its prof-
itability can also be attributed to the high demand for its services. Many consider
it to be one of the top eye-care centers in the world because its doctors and nurses
have gained so much technical experience through the remarkable volume of pro-
cedures they perform. Aravind offers a wide range of options to make stays in its
hospitals more comfortable for those who can pay, including air-conditioned sin-
gle rooms. Profits from these services help subsidize the poor patients who also
have their sight restored at Aravind hospitals. Aravind also reaches out to villagers
through government-sponsored eye camps that help bring those in need of treat-
ment to their hospitals.
Aravind integrates commercial principles and models into health-care delivery
and dramatically improves both the quality and availability of health care. By spe-
cializing in eye care, it can routinize procedures and reduce costs through scale.
Other hospitals, especially those specializing in one area of treatment, can follow
Aravind’s example, using more creative pricing schemes to subsidize the care of
those who cannot afford treatment.33
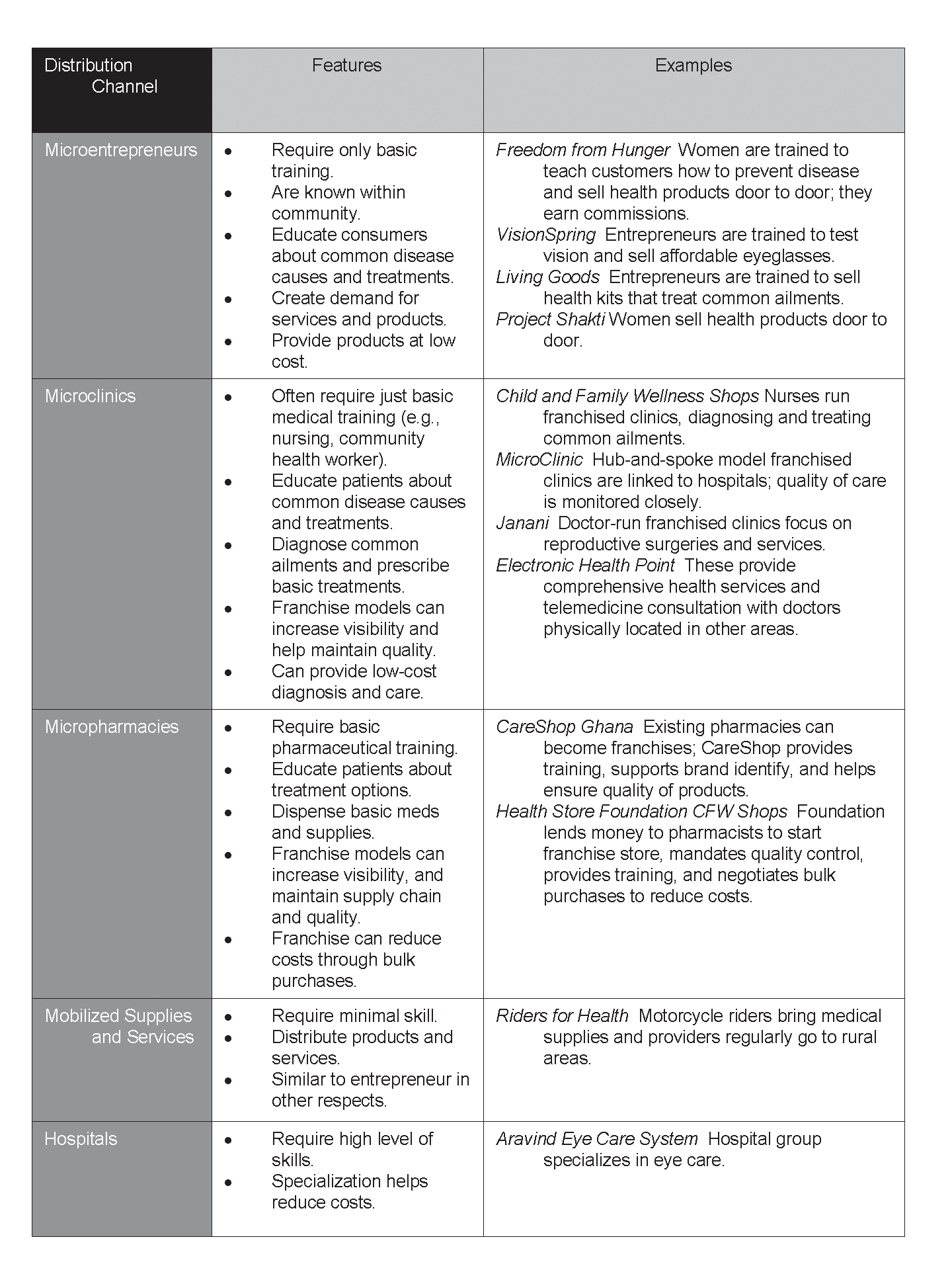
Tableau 1 (following page) summarizes these distribution channels. It offers sig-
nificant current examples of successful implementations that can bring health
products and services to the rural poor in developing countries. Integrating these
programs into a more holistic system can dramatically improve both access and
quality of health care for the poor around the world.
nouveautés / volume 6, number 2
127
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
Tableau 1. Distribution Channels
A HEALTH DISTRIBUTION MODEL
More effective distribution systems help save lives by making disease prevention
and medical care more available and accessible to those in need. Because challenges
in global health occur on such a large scale, improved systems need to be cost effec-
128
nouveautés / Meaningful Markets
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Delivering Health Care to the Global Poor
tive, scalable, and financially sustainable. Chiffre 1 portrays such an integrated
approche.
To solve the challenge of availability and accessibility, these distribution sys-
tems must rely heavily on a sustainable model that integrates and complements
governmental and NGO support and facilitates the coordination of products and
services. With this approach, increased scale improves cost efficiency, access to
products and services, financial sustainability, and societal health and well-being.
To both treat and prevent the spread of diseases, distribution channels must
provide education and supplies for prevention and treatment, along with basic,
advanced, and emergency diagnostics and treatment and medications. Éducation
can inform people about many aspects of disease: how they are transmitted and
can be prevented, how health-care supplies can help them stay healthy, and how to
recognize symptoms, and when to seek more intensive diagnosis and treatment.
Health supplies—including condoms, sterile delivery kits, soaps, and insecticide-
treated bed nets—can help prevent the spread of diseases. Diagnostics can help cli-
nicians determine if treatment is necessary, and if so, what type to provide.
Clinicians trained in basic diagnosis and treatment can provide the most care and
treatment. Trained providers can safely prescribe basic medications. Each level of
the health system provides multiple products and services to address different dis-
eases.
Distribution Matrix: A Summary of Opportunities for Health-Care Delivery
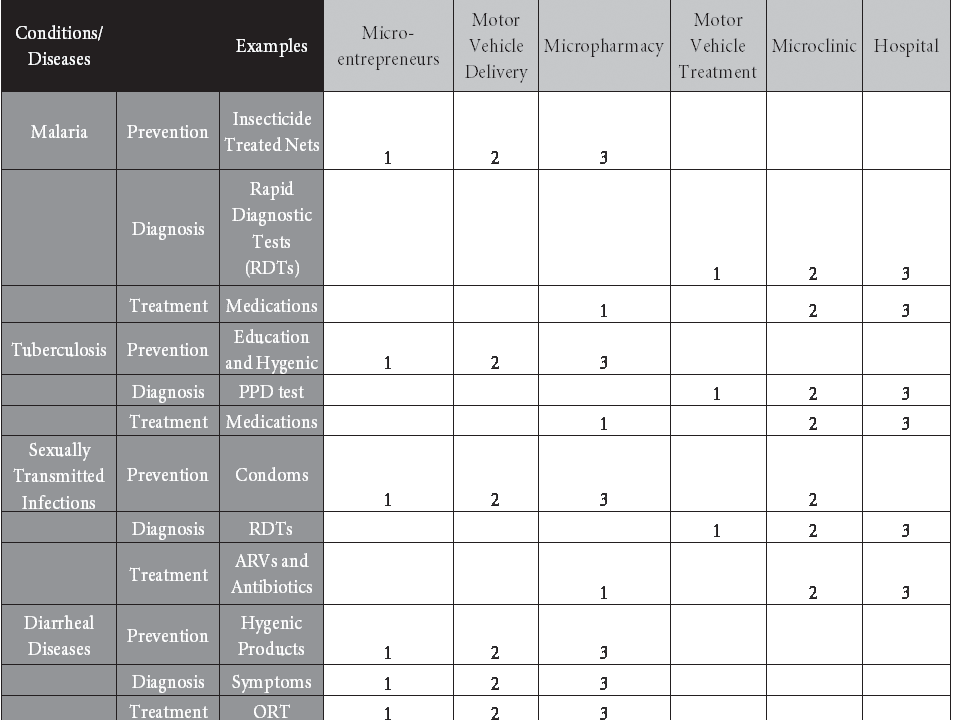
Tableau 2 (following page) shows a health-care delivery matrix. The columns repre-
sent different methods of health-care delivery, while the rows represent different
types of products and services that a health-care system in a resource-constrained
setting could provide. For each product or service type, three different distribution
channels are potential providers and are noted by the numbers in the correspon-
ding boxes in each row showing product and service type. Each provider, which is
responsible for providing a given intervention, has been ranked, balancing con-
cerns for accessibility, safety, efficacité, and efficiency. Par exemple, the matrix
indicates that, balancing these concerns, microentrepreneurs could provide malar-
ia prevention (insecticide-treated nets) to consumers. This is shown by the 1 dans le
box corresponding to microentrepreneurs in the malaria prevention row. In areas
where microentrepreneurs could not deliver bed nets, motor vehicles would prove
an effective distribution mechanism. This is shown by the 2 in the box correspon-
ding to motor vehicle delivery in the malaria prevention row. If either of these
delivery mechanisms were absent in certain areas, then micropharmacies could
distribute bed nets. This is indicated by the 3 in the corresponding box.
Notice that in every product-service row in the figure, the numbers ascend
from the left to the right. This is because the providers are typically ascending in
levels of training and operating expense. In such a matrix, the provider rankings
must ascend from left to right to meet the condition of cost effectiveness. Le
provider that is ranked as the most effective delivery mechanism is largely deter-
nouveautés / volume 6, number 2
129
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
Tableau 2. Health Distribution Matrix.
Note: The Numbers 1, 2, et 3 represent a ranking of the primary providers
based on accessibility, safety, efficacité, and efficiency.
mined by safety concerns. Microentrepreneurs could deliver malaria treatment, pour
example, even though the box corresponding to micropharmacies in this row is
marked with a 1. The matrix ranking reflects the safety concerns and regulatory
environment often associated with delivering prescription anti-malarial medi-
cines. En fait, in some regulatory settings, it may be appropriate to have microen-
trepreneurs deliver anti-malarials. The figure is meant to serve as a guide. It is not
context-specific, and should not be considered as a universal prescriptive tool.
Aussi, some overlapping services will vary by region. Plutôt, the figure should serve
as a starting point in efforts to examine how delivery systems can best address
issues of cost effectiveness, consistency, and sustainability by leveraging synergies
and differences between different providers. It must be adapted to different regions
based on regulatory regimes, local needs, the availability of products and services,
and capacity.
Applying the Model: An Example of Malaria Care Delivery
Malaria was responsible for approximately 863,000 deaths worldwide during 2008,
avec 89% of those cases in Africa.34 It is caused by a blood-borne parasite that is
spread by mosquitoes. It can be prevented by ensuring that still water, where mos-
130
nouveautés / Meaningful Markets
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Delivering Health Care to the Global Poor
quitoes breed, is cleaned up, and by using insecticide-treated bed nets that cost $5 and require a small amount of training to install. It can be diagnosed by noting clinical symptoms such as high fever, sweating, headaches, chills, and fatigue; by examining a stained blood smear under a microscope; or by using malaria rapid diagnostic tests. Et, it can be treated by using anti-malarial pills that cost 50 cents a dose.35 Malaria can be addressed by each of the distribution channels, indicated by the lines connecting malaria to their corresponding boxes. Each of these distribution channels can provide needed interventions to alle- viate the symptoms and prevent the spread of malaria. Microentrepreneurs can educate consumers about the signs and symptoms of malaria, supply them with insecticide-treated nets, and train them on their proper use. The products and services offered by different providers overlap significantly. Par exemple, to deliver malaria care, every provider can effectively provide insec- ticide-treated bed nets in low-resource settings. This overlap is important because the poor often do not have access to all the different levels of a health-care system. When they do access the system at any level, care must be available to let them address the most pressing conditions. Using this distribution system, shown in Figure 1, can improve health along the lines connecting needed interventions to better health outcomes. This distri- bution system may increase access by lowering costs and increasing incentives for delivery. Ainsi, increased access to prevention and treatment measures reduces both morbidity and mortality from these diseases. The figure shows how this works by connecting all the interventions needed to reduce morbidity and mortal- ville. To be maximally effective, regulatory mechanisms should be in place and enforced to ensure that medications are effective and properly prescribed.36 Better health outcomes from malaria prevention and treatment can result in better economic and social outcomes. WHO estimates that malaria reduces eco- nomic growth in some African countries by 1.3 percent per year.37 Because reduc- tions in gross domestic product compound over time, it is estimated that the econ- omy of sub-Saharan Africa could have been up to 32 percent larger in 2001 if malaria had been eradicated 35 years earlier.38 These economic costs often have on social impact because they contribute to poverty and dependence on aid pro- grams. This approach is designed to ensure that those who have been underserved by the health-care industry have consistent and sustainable access to health care. Proximity to a health-care provider is an important determinant of access. Each aspect of this model aims to bring more advanced care closer to those in rural communities who must often travel long distances to receive care. This model can significantly alleviate the accessibility problem. This approach has the potential to succeed because it combines for-profit and nonprofit methods of health-care delivery, and also uses existing successful distri- bution mechanisms. Governments, NGOs, and for-profit businesses have succeed- ed in implementing different aspects of this model, but their efforts have often innovations / volume 6, number 2 131 Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Marc J. Epstein and Eric G. Bing failed to become scalable. Integrating their approaches should make it possible to address the accessibility problem more effectively. Like some other models of increased access to products for developing coun- tries,39 this model has been created by examining the excellent, successful organi- zations and projects that have been established to address these needs. These proj- ects have been limited to one country or have focused on one disease or need, and often they provide only one delivery mechanism to a limited population. Sometimes they are run by governments, at other times by NGOs, at times by pri- vate for-profit businesses, and occasionally by a combination of these entities. The knowledge and systems often already exist, but only by integrating the products and services and coordinating the delivery mechanisms will it be possible to signif- icantly improve health outcomes in developing countries. OUTCOMES AND IMPACT Significant positive outcomes are likely to occur if organizations use this more comprehensive health-care distribution model to deliver needed interventions in low-resource settings. It may increase access to care because it leverages the bene- fits of business models to address the issues of efficiency, cost-effectiveness, and sustainability that have inhibited many efforts to deliver health care in low-income countries. Delivering supplies, éducation, diagnosis and treatment, medications, and emergency care through this system may also reduce morbidity and mortali- ty. These delivery systems and improved health outcomes may then result in improved economic and social outcomes. Health and wealth have been shown to be inextricably linked, and poor health affects both economic and social outcomes.40 Conversely, improving health out- comes can have a significant impact on household wealth, decision making, socioeconomic status, and education. A system that leverages local enterprises to deliver products and services can increase profits and return on investment, and also promote local economic development, quality of life, and individual and com- munity self-reliance.41 Many diseases also have economic costs in lost productivity and mortality that inhibit growth and contribute to poverty.42 Ventures that involve the world’s poorest entrepreneurs can have significant economic impacts, by increasing consumer buying power (through reduced prices), increasing the demand for products and services, and increasing both job creation and infra- structure development.43 Social impacts from similar initiatives can include increased self-esteem, dignity, and respect, both for the entrepreneurs who earn sustainable income and for the communities that become less dependent on for- eign or government handouts. Bridging the Gap: Improving Health-Care Delivery in Resource-Constrained Environments The model and methods we described above provide an outline for complete and comprehensive health-care systems for developing countries. In resource-con- 132 nouveautés / Meaningful Markets Downloaded from http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Delivering Health Care to the Global Poor strained settings, cependant, many of the redundancies and overlap between providers we have described might not be possible or desirable. Plutôt, specific countries will likely adapt this approach in the ways they see as most appropriate for their capacity and needs. They may also be able to use these examples to iden- tify new programs and integrate or mimic successful organizations to maximize the impact of the limited funds available for health. In many countries, health-care providers compete with each other and little coordination exists between different levels of the system. Souvent, these providers serve only marginally overlapping markets with radically different types of servic- es. Donc, significant benefits can follow from integrating this system into a more holistic health-care system for both rural and urban populations. In an integrated system, a flow of supplies from more advanced providers can facilitate large purchases of supplies at discounted prices and sales to less advanced providers, who can disseminate these much-needed supplies to rural and urban populations. Cell phones and the Internet have facilitated innovations in telemed- icine, which can bring advanced clinical diagnostics and treatment to even the most rural populations. By using technology and proven models for product and service delivery, these providers can coordinate their efforts to minimize the cost of improving health- care systems in developing countries. Coordination of the products and services provided can also ensure that physical infrastructure does not inhibit health-care systems from providing improved care to rural populations. Benefits of an Integrated System: Moving to Implementation The efforts, systèmes, and examples described above provide several lessons for those interested in improving the dissemination of health information, technolo- gies, des produits, and services in developing countries: 1. Brand names can stimulate demand for and trust in health-care providers. 2. Commercial models are effective at delivering scalable health-care services to the poor, can be integrated into current delivery systems, and can promote economic development. 3. No single provider can (or should) do everything. 4. Greater coordination is required between each player in a health-care sys- tem. 5. Regulatory controls will help ensure the quality of products and services. 6. Increased access to capital will help private-sector entrepreneurs grow. Brand names can stimulate demand for and trust in health-care providers. Living Goods, CFW shops, MicroClinics, CareShops, and FFH all demonstrate the power of a brand name in stimulating demand for health-care services in developing countries. Researchers have pointed out how important brand names are to illiter- ate consumers.44 The logo can become immediately recognizable to even the least educated consumers, allowing them to more readily identify a pharmacy or clinic innovations / volume 6, number 2 133 Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Marc J. Epstein and Eric G. Bing and seek care. En outre, brand names provide consumers with greater consisten- cy in the type and quality of care they receive. This improves the trust they have in their providers, and may stimulate future demand for services. Commercial models are effective at delivering scalable health-care services to the poor, can be integrated into current delivery systems, and can promote economic development. Many of the organizations described above have integrated for-prof- it subsidiaries or for-profit businesses into their business models to deliver health care to consumers more effectively. This not only helps align the incentives of direct providers with the goals of organizations in a search for improved sustain- ability, but also stimulates local economies. To the extent that many of these organ- izations are development organizations, these interventions can better serve their goals by improving the lives on both sides of any transaction: one community member’s health improves while another community member earns a small prof- it. Other successful organizations have integrated product and service delivery models, such as hub-and-spokes systems, which can facilitate the delivery of goods and services more efficiently than other systems. Connecting a set of outlying nodes to central locations can often reduce distribution costs. The providers can be thought of as operating in a tiered hub-and-spoke system, where micropharma- cies are hubs to microentrepreneurs, microclinics to micropharmacies, etc.. By coordinating care in this way, health-care systems can maximize their impact cost- efficiently. No single provider can (or should) do everything. As Table 2 shows, no provider offers a completely comprehensive product or service. Toujours, considerable overlap can exist between potential providers. Microentrepreneurs, micropharmacies, and mobile delivery and treatment centers are meant to increase access and alleviate the burden on doctors and nurses. When a single provider tries to do too much, costs rise and the system is not making effective use of the trained health-care workers available. In such situations, cost effectiveness is imperative to stretch scarce health-care resources as far as possible to save and improve lives. Greater coordination is required between each player in a health-care system. Many of the successful organizations described above have achieved scale by allow- ing a larger purchaser to increase buying power in the market for pharmaceuticals. Others improved their supply chains through mobilized delivery of health prod- ucts. Still others had local partners in each country where they operate to better integrate them into the health-care infrastructure. When interventions use the available health-care infrastructure and understand how to leverage existing pro- grams, they alleviate the burden on other providers and become a part of existing government, NGO, and business efforts that will best achieve their goal of improv- ing health outcomes. Regulatory controls will help ensure the quality of products and services. Strong temptations exist for unscrupulous providers to maximize profits by reducing the quality of products and services or delivery; many examples support this claim.45 134 nouveautés / Meaningful Markets Downloaded from http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Delivering Health Care to the Global Poor To counter this situation, quality standards must be in place and regulatory poli- cies must be enforced. Ideally, such standards and policies will be in the public sec- tor and be conducted in a transparent way, free from corruption. Cependant, when such controls are not available in the public sector, a competitive private sector will be motivated to develop them to increase quality and trust in products and servic- es.46 These lessons learned are some of the determinants of success in health-care delivery. These efforts, along with others that try to improve the dissemination of health information, des produits, and services, face significant opportunities and chal- lenges that can affect their success. Increased access to capital will help private-sector entrepreneurs grow. The lack of access to capital greatly hinders the development and expansion of the private sec- tor in developing countries.47 While microlenders in countries throughout the world have helped entrepreneurs with very small loans, the more substantial loans needed by small and medium-size enterprises in developing countries are not readily available. To expand successfully, these enterprises need access to capital to market their services, purchase in bulk, and staff and strengthen their administra- tive and financial operations and capabilities.48 If financial institutions expand financial services to such enterprises in developing countries, that could prove profitable both to the enterprises and the financial institutions and also be benefi- cial to society. OPPORTUNITIES AND THE USE OF TECHNOLOGY The delivery matrix in Table 2 can be expanded by providers to address other dis- eases and conditions. Par exemple, cardiovascular disease now accounts for 20% of deaths in developing countries.49 Expanding the products and services provided in this health-care system would require additional financial and human resources, but the distribution system can be adapted to address changing health-care needs as resources permit. We also see opportunities to leverage technology to reduce costs and improve quality in this integrated health-care system. The use of cellular phones has increased efficiency in health-care delivery by vastly increasing the communication between patients and health-care providers,50 and between different types of health-care providers. One survey estimated that by 2010, 85% of Africans would have cellular phones.51 Health-care providers have only begun to explore how to use these devices to provide quicker and more efficient health-care interventions, but cell phones are already significantly helping expand health-care access. Phones can be used to order supplies or alert a health-care worker of a patient’s arrival. They can permit patients to describe symptoms to health-care workers, allowing doctors and nurs- es to screen them more efficiently. They can facilitate diagnosis and treatment more effectively through telemedicine. Health-care providers and microfinance institutions that rely on loan repayment have also lowered the cost of collecting innovations / volume 6, number 2 135 Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023 Marc J. Epstein and Eric G. Bing payments by training clients and loan officers to utilize the capabilities of cell phones. Mobile technology can also be used to support provider and staff training and ongoing supervision to ensure that providers and staff have up-to-date health and business knowledge. A public-private partnership between the United Nations Foundation and the Vodafone Foundation, called mHealth, has supported many adaptations of mobile technologies in health-care settings. mHealth has identified four main potentials of mobile technologies to improve health outcomes. It can increase access to health care and health-related information, improve capabilities to diagnose and track diseases, improve access to public health information, and expand access to ongo- ing medical education and training for health workers. Around the world, mHealth projects have already been shown to increase compliance with treatment regimens (especially for patients with tuberculosis), improve public health aware- ness, stimulate demand for health-care services, improve disease management (especially for diabetes patients), and improve efficiency in health-care systems.52 Electronic Health Point (EHP) is a for-profit service that opened its first units in 2009 in Punjab. As mentioned earlier, it is developing microclinics in India with a comprehensive set of services. The business model uses telemedicine and tech- nology to link a doctor and modern health care to rural communities through video-conferencing and wireless broadband Internet. The telemedical consultants cost the patient less than $1 per visit.53
Pesinet, an NGO that operates in Mali, exemplifies how using cellular phones
can drastically reduce the cost of providing health-care care services in developing
des pays. Pesinet provides an integrated health-care and insurance program for
children aimed at battling malnutrition and diarrheal diseases, which account for
17 percent of childhood deaths in developing countries.54 For little more than $1 per month per child, a trained weighing agent comes to a family’s home and weighs its children, starting at twice a week for newborns. The agent then enters the information into a mobile phone and sends it to a doctor who looks at the data for abnormalities, and calls the mother to schedule an appointment for the next day if necessary. Any medicines the doctor provides at the appointment are sold at a fifty percent discount, making it easier for these families to afford the care they need to keep their children healthy and alive. Pesinet can afford these subsidies because the information technology has significantly reduced the cost of diagnos- ing illness. This and other projects that leverage technology to reduce costs have the potential to greatly improve access to health-care services for the poor. Smart cards are also becoming a useful tool in health-care distribution by pro- viding cheap and accurate biometrics. In India, the National Health Insurance Program has added smart cards to its effort to reach out to the nation’s poorest 300 millions de personnes. Containing personal data and fingerprints for an entire family, the smart card costs less than $1 and works at any public or private hospital enrolled
in the program. In India, consumers can compare the costs of different insurance
plans based on the information on their smart cards. This promotes competition
between insurance companies, helping drive down costs, and ultimately helping
136
nouveautés / Meaningful Markets
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Delivering Health Care to the Global Poor
reduce what families must pay for care. Smart cards also have the potential to serve
as storage units for electronic medical records—and give health-care providers
instant access to all of a patient’s medical information. In addition to reducing
medical errors, this can help drive down the cost of care, making visits more effi-
cient by better utilizing the time of health-care workers.
When coupled with mobilized card readers, smart card technology can
become especially useful. Par exemple, dans 2006, parts of Malawi were hit by
drought. Crop failures inevitably ensued. Normally during such crises, food pack-
ages are delivered to those in need. Local farmers, cependant, were concerned that
the aid shipments would be delayed as they had been in the past, and indicated that
they would just prefer a cash payment to help them purchase food. Concern
Worldwide, an NGO, teamed up with Opportunity International Bank Malawi
(OIBM), to distribute this cash by using smart cards containing biometric data and
account information. OIBM provided a mobile bank, located in an armored truck,
that traveled from village to village. This permitted Malawians to obtain a substi-
tute for food aid that they could use on whatever they most needed in the recov-
ery process. Through smart cards and mobile card readers, OIBM successfully pro-
vided an emergency intervention that helped maintain the health of a population
in crisis. This is just one more example of how technology can be leveraged to dis-
tribute resources in environments with limited infrastructure.
CHALLENGES
Many challenges make it difficult for any health-care system to succeed in deliver-
ing services in developing countries. D'abord, a need for more diverse health-care
services has been developing in the last few decades. The epidemiology of diseases
in developing countries is transitioning from infectious diseases like malaria to
more chronic ones like cardiovascular disease and diabetes. The United Nations
estimates that this transition has already resulted in a 20% decrease in the disease
burden caused by communicable diseases in developing countries, and the World
Diabetes Foundation estimates that by 2025, 80% of new diabetes cases will be in
developing countries.55 As this disease burden continues to shift, so will the types
of treatments and preventative measures required to keep people healthy and func-
tioning. This situation will place a great strain on health-care systems, as suppliers
and more basically trained providers must be retrained and change their product
and service lines to match the new needs of communities. Because non-communi-
cable diseases often result in longer periods of disability and require more expen-
sive treatment, the demand for health-care services will also increase as the devel-
oping world continues through this period of transition. Spending on health care
may also become less cost effective as disease patterns shift.
The demand for health services also grows as population grows. In sub-
Saharan Africa, the most underdeveloped of the world’s regions, the population is
expected to double to 1.7 billion by mid-century and reach 3 billion by 2100.56 À
that point, it would be home to more than one-third of the world population. Ce
nouveautés / volume 6, number 2
137
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
staggering growth will crowd health infrastructures and may even contribute to
the spread of disease in urban areas.
In addition, regulatory policy will present difficult choices. In developed
économies, a significant amount of training is required for people who distribute
medicines and treatment. Care providers are legally required to have this training.
In low-resource settings, similar barriers can hinder the distribution of health
interventions. De même, some providers in the private sector, such as traditional
healers, may be unregulated. By creating standards and certifications that are
appropriate but not overly burdensome, regulators can improve access and safety.
Despite these challenges, the examples above demonstrate how innovation in
health-care delivery can expand access to needed health-care products and servic-
es. The role that information technology will play in health-care systems also has
yet to be decided. Cell phones, computers, and the Internet are likely to revolution-
ize the treatment and prevention of disease as they become more accessible to the
developing world.
CONCLUSION
Governments, NGOs, and for-profit businesses have made great strides in improv-
ing health-care delivery in developing countries. Many have tried bold new meas-
ures to solve the accessibility problem, and have achieved some success. Even so,
their efforts are still failing to reach many of the poorest. It will take a reimagining
of the entire health-care delivery system to best reach those who die every day
because they lack access to the health care they need. No single entity can do this
alone. The best way to address the accessibility problem is through cooperative
efforts between governments, NGOs, and businesses. Each has unique competitive
advantages in health-care delivery, so it is important that each have a role in deliv-
ering health care to the poor. Microentrepreneurs, mobile health-care delivery sys-
thèmes, clinics, pharmacies, and hospitals are all needed in the private and public sec-
tor to provide more consistent and sustainable access to health care.
It is unfortunate that about 150,000 people die every day. But it is tragic that
30,000 of those who die are children, especially since many of those deaths can be
prevented through low-cost prevention and treatment services that remain out of
the reach of the world’s poorest.57 The technologies and personnel exist to begin to
address this issue—but without learning lessons from successful, scalable distribu-
tion systems and integrating already strained providers into a more comprehensive
health-care delivery system, it will be impossible to leverage existing resources to
begin to alleviate some of the world’s most glaring inequalities in health.
All of the components of this more comprehensive system already exist today.
By integrating those components and relying more on commercial models,
expanding successful programs, and developing appropriate regulatory controls, it
is possible to immediately improve public health, reduce the costs of care, et
reduce mortality. It is critical to do this now.
138
nouveautés / Meaningful Markets
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Delivering Health Care to the Global Poor
Acknowledgement
The authors acknowledge and thank Josh Ozer, Dean William Glick, and profes-
sors Rebecca Richards-Kortum and Terrance Williams for their significant support
de, and collaborative assistance with, this work.
1. UNICEF, Levels and Trends in Child Mortality (New York: UNICEF, 2010).
2. United Nations, Millennium Development Goals Report 2008 (New York: United Nations, 2008);
Gareth Jones et al., “How many child deaths can we prevent this year?” The Lancet 362 (Juillet 2003):
65–71.
3. World Health Organization (WHO), The Global Burden of Disease: 2004 Update (Genève,
Suisse: WHO, 2008).
4. Nirmala Ravishankar et al., “Financing of Global Health: Tracking Development Assistance for
Health from 1990 to 2007,” The Lancet 373 (Juin 2009): 2113–2124.
5. World Health Organization, World Health Report 2006 (Genève, Suisse: WHO, 2006).
6. Based on National Health Accounts (NHA) reports from most recent year available between 1995
et 2002 for Ethiopia, Kenya, Malawi, Namibia, Nigeria, Rwanda, Tanzania, Uganda, Zambia, et
Zimbabwe. Available at http://web.worldbank.org/WBSITE/EXTERNAL/TOPICS/EXTHEALTH-
NUTRITIONANDPOPULATION/EXTHSD/0,,contentMDK:22676278~menuPK:376799~pageP
K:148956~piPK:216618~theSitePK:376793~isCURL:Oui,00.html; other sources confirm this state-
ment for other countries.
7. Ruairi Brugha and Anthony Zwi, “Improving the quality of privately provided public health care
in low and middle income countries: Challenges and strategies,” Health Policy and Planning 13
(1998): 107–120; Lucy Gilson et al., Challenging Inequity through Health Systems (Genève: WHO
Commission on the Social Determinants of Health, 2007); Marriott, “Blind Optimism:
Challenging the myths about private health care in poor countries” Oxfam Briefin Paper
(Février 2009); Rainer Sauerborn, “Low quality of care in low-income countries: Is the private
sector the answer?” International Journal for Quality in Health Care 13 (2001): 281–282.
8. Charles Hongoro and Lilani Kumaranayake, “Do they work? Regulating for-profit providers in
Zimbabwe,” Health Policy and Planning 15 (2000): 368–377; Christoph Boller et al., “Quality and
comparison of antenatal care in public and private providers in the United Republic of Tanzania,»
Bulletin of the World Health Organization 81 (2003): 116–122.
9. Benjamin Loevinsohn and April Harding, “Buying results? Contracting for health service delivery
in developing countries,” The Lancet 366 (2005): 676–681; Joanne Yoong et al., “Private sector par-
ticipation and health system performance in sub-Saharan Africa,” PLoS One 5 (2010): e13243;
World Bank, Africa Development Indicators (Washington, CC: World Bank, 2006).
10. Hassan Masum et al., “Accelerating Health Product Innovation in sub-Saharan Africa,»
Innovations 2 (2007): 129–149.
11. Suresh De Mel, David McKenzie, and Christopher Woodruff, “Returns to Capital in
Microenterprises: Evidence from a Field Experiment,” The Quarterly Journal of Economics 123
(2008): 1329–1372.
12. Sam Daley-Harris, State of the Microcredit Summit Campaign Report 2009. Available at
http://www.microcreditsummit.org/uploads/scors/SOCR2009_English.pdf.
13. Janna Greve, “Healthcare in developing countries and the role of business: A global governance
framework to enhance the accountability of pharmaceutical companies,” Corporate Governance
8 (2008): 490–505.
14. C. K. Prahalad, The Fortune at the Bottom of the Pyramid: Eradicating Poverty Through Profits
(Upper Saddle River, New Jersey: Wharton School Publishing, 2010).
15. Freedom from Hunger (FFH), MicroBusiness for Health: Health Products and Counseling at the
Doorstep; Freedom for Hunger Annual Reports 2008, 2009 (Davis, Californie: FFH, 2007, 2008, 2009).
16. VisionSpring, “What we do.” Available at http://www.visionspring.org/what-we-do/why-eye-
glasses.php.
nouveautés / volume 6, number 2
139
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Marc J. Epstein and Eric G. Bing
17. LivingGoods, “LivingGoods BRAC Joint Venture in Uganda.” Available at http://www.living-
goods.org/brac.asp. Accessed April 20, 2011.
18. Greg Van Kirk, “The MicroConsignment Model: Bridging the ‘Last Mile’ of Access to Products
and Services for the Rural Poor,” Innovations 5 (2010): 101-127.
19. V. Kasturi Rangan, Dalip Sehgal, and Rohithari Rajan, “The Complex Business of Serving the
Poor: Insights from Unilever’s Project Shakthi in India,” in Business Solutions for the Global Poor:
Creating Social and Economic Value, éd. V. Kasturi Rangan (San Francisco, Californie: Jossey-Bass,
2007): 144–154.
20. WHO, The Global Burden of Disease: 2004 Update.
21. The HealthStore Foundation, “About the HealthStore Foundation Overview.” Available at
http://www.cfwshops.org/overview.html; Michelle Fertig and Herc Tzaras, “Franchising Health
Care for Kenya: The HealthStore Foundation Model,” in Microfranchising: Creating Wealth at the
Bottom of the Pyramid, éd. Jason S. Fairbourne, Stephen W. Gibson, and W. Gibb Dyer, Jr..
(Northampton, MA: Edward Elgar 2007): 164–182.
22. MicroClinic, “Our Solution.” Available at http://www.microclinics.com/oursolution.asp.
Accessed April 20, 2011.
23. Janani, “We are.” Available at http://www.janani.org/factsheets/janani_corporate_brochure.pdf.
Accessed May 3, 2011.
24. Roger Bate, “Fake Drugs Kill the Poor,” Economic Affairs 27 (2007): 84.
25. World Resources Institute, What Works: CareShop Ghana. Improving Access to Essential Drugs
through Conversion Financing (Washington, CC: World Resources Institute).
26. HealthStore Foundation, “Overview”; Fertig and Tzaras, “Franchising Health Care for Kenya.”
27. Maximo Torero and Shayamal Chowdhury, Increasing Access to Infrastructure for Africa’s Rural
Poor (Issue brief no. 16; Washington, CC: International Food Policy Research Institute, 2005).
28. Andrea Coleman, “Riders for Health: Health Care Distribution Solutions in Sub-Saharan Africa”
(2007 Case #GS-58; Stanford, Californie: Stanford Graduate School of Business, 2007).
29. Riders for Health, “Welcome to Riders for Health.” Available at www.riders.org. Accessed April
20, 2011.
30. Coleman, “Riders for Health.”
31. African Infectious Disease Village Clinics (AIDVC), “Our Mission.” Available at http://aidvillage-
clinic.org/flash/index.html. Accessed April 20, 2011.
32. C. K. Prahalad, “Aravind Eye Care: The Most Precious Gift,” in Pralahad, The Fortune at the
Bottom of the Pyramid: Eradicating Poverty through Profits (Upper Saddle River, New Jersey: Wharton
School Publishing, 2010): 283–298.
33. Ibid..
34. World Health Organization, World Malaria Report 2009 (Genève, Suisse: WHO, 2009).
35. William J. Clinton Foundation, “News: Making Malaria Medications More Affordable.” Available
at http://clintonfoundation.org/news/news-media/making-malaria-medications-more-afford-
capable. Accessed April 20, 2011.
36. International Finance Corporation (IFC), The Business of Health in Africa: Partnering with the
Private Sector to Improve People’s Lives (Washington, CC: IFC, 2007). Available at
http://www.ifc.org/ifcext/healthinafrica.nsf/Content/FullReport.
37. World Health Organization, The Global Burden of Disease 2002 Estimates (Genève, Suisse:
WHO, 2002).
38. World Health Organization (2000). Economic Costs of Malaria Are Many Times Higher than
Previously Estimated. Press release, WHO/28, Avril 25, 2000. Available at
http://www.who.int/inf-pr-2000/en/pr2000-28.html.
39. Laura J. Frost and Michael R. Reich, Access: How do Good Health Technologies Get to Poor People
in Poor Countries? (Cambridge, MA: Harvard Center for Population and Development Studies,
2008); David Wheeler et al, “Creating Sustainable Local Enterprise Networks,” MIT Sloan
Management Review 47 (2005): 33–40.
40. David M. Cutler, Adriana Lleras-Muney, and Tom Vogl, Socioeconomic Status and Health:
Dimensions and Mechanisms (Paper no. 14333; Cambridge, MA: National Bureau of Economic
140
nouveautés / Meaningful Markets
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023
Delivering Health Care to the Global Poor
Research, 2008).
41. MicroClinic, “Our Solution.”
42. Hoyt Bleakley, “When does Improving Health Raise GDP? Comments on Ashraf, Lester, et
Weil” (remarks delivered at the 2008 NBER Macro Annual, Juillet 23, 2008). Available at
http://home.uchicago.edu/~bleakley/Bleakley_Comments_ALW.pdf. Accessed April 20, 2011.
43. Ted London, “Making Better Investments at the Bottom of the Pyramid,” Harvard Business
Review (May 2009): 106–112.
44. Madhubalan Viswanathan, José Antonio Rosa, and James Edward Harris, “Decision-Making and
Coping by Functionally Illiterate Consumers and Some Implications for Marketing
Management,” Journal of Marketing 69 Non. 1 (Janvier, 2005): 15–31.
45. Hongoro and Kumaranayake, “Do they work?»; Boller et al., “Quality and comparison.”
46. International Finance Corporation (IFC), The Business of Health in Africa: Partnering with the
Private Sector to Improve People’s Lives (Washington, CC: IFC, 2007). Available at
http://www.ifc.org/ifcext/healthinafrica.nsf/Content/FullReport. Accessed April 20, 2011.
47. IFC, The Business of Health.
48. IFC, The Business of Health.
49. WHO, The Global Burden of Disease: 2004 Update.
50. Patricia N. Mechael, “The Case for mHealth in Developing Countries,” Innovations 4 (2009):
103–118.
51. The Economist, “Finishing the job: A special report on telecoms in emerging markets,»
Septembre 24, 2009. Available at http://www5.economist.com/node/14483856. Accessed April
20, 2011.
52. United Nations Foundation and Vodafone Foundation, mHealth for Development: Le
Opportunity of Mobile Technology for Health Care in the Developing World. Available at
http://www.unfoundation.org/global-issues/technology/mhealth-report.html. Accessed April
20, 2011.
53. E Health Point, “About Us.” Available at http://www.ehealthpoint.com/?page_id=2. Accessed
Avril 20, 2011.
54. WHO, Global Burden of Disease 2002 Estimates.
55. Colin D. Mathers, Alan D. Lopez, and Christopher J. L. Murray, “The Burden of Disease and
Mortality by Condition: Données, Methods, and Results 2001” in Global Burden of Disease and Risk
Factors, éd. Alan D. Lopez et al. (Washington, CC: World Bank, 2006), Chapter 3.
56. Martin Walker, “The World’s New Numbers,” The Wilson Quarterly (Spring 2009): 24–31.
57. United Nations. Millennium Development Goals Report 2005 (New York: United Nations, 2005).
nouveautés / volume 6, number 2
141
Téléchargé depuis http://direct.mit.edu/itgg/article-pdf/6/2/117/704805/inov_a_00073.pdf by guest on 08 Septembre 2023