The Rise and Fall of
Chagas Disease
Marilia Coutinho
University of Florida
João Carlos Pinto Dias
Centro de Pesquisas René Rachou
American Trypanosomiasis, known as Chagas disease, was discovered in
1909 under peculiar circumstances: its discoverer, Carlos Chagas, was sent
to a small village of Central Brazil to carry out an anti-malaria campaign
when he came across a blood sucking insect—the vector for the parasite infec-
tion. He had been alerted to the coincidence of peculiar symptoms and the
presence of this insect in the wood and earth dwellings of the region. He was
deeply involved in theoretical controversies in international protozoology; he
was engaged in the consolidation of a scientiªc role and corresponding insti-
tutional conditions in Brazil, and equally immersed in the nationalist sani-
tary struggles of his days. In these contexts, Chagas assembled a remarkable
discovery discourse, regarding the biology of the parasite, its life cycle and
mode of transmission. Furthermore, he provided the clinical description of a
new disease. Despite immediate international recognition, however, the un-
stable institutional arrangements surrounding his work damaged its local le-
gitimacy for decades. His authority was widely recognized abroad, but re-
jected at home.
Introduction
In a railway wagon, young Carlos Chagas, a Brazilian physician, impro-
vised his clinic and laboratory in the Winter of 1907. He was in Lassance,
a Brazilian hinterland far away from Rio de Janeiro, the capital of the
the Instituto Soroterapico de
country, where Chagas worked for
This investigation has been supported by the Program of Small Grants for Research in So-
cial and Economic aspects of Tropical Diseases of the Laboratorio de Ciencias Sociales—
Universidad Central de Venezuela, with ªnancial support from the Special Program for Re-
search and Training in Tropical Diseases (TDR)—UNDP/World Bank/WHO. The authors
are greatly indebted to Vassiliki B. Smocovitis and to Marcos Cueto for their reading and
comments.
Perspectives on Science 1999, vol. 7, no. 4
©2000 by The Massachusetts Institute of Technology
447
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
448
The Rise and Fall of Chagas Disease
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
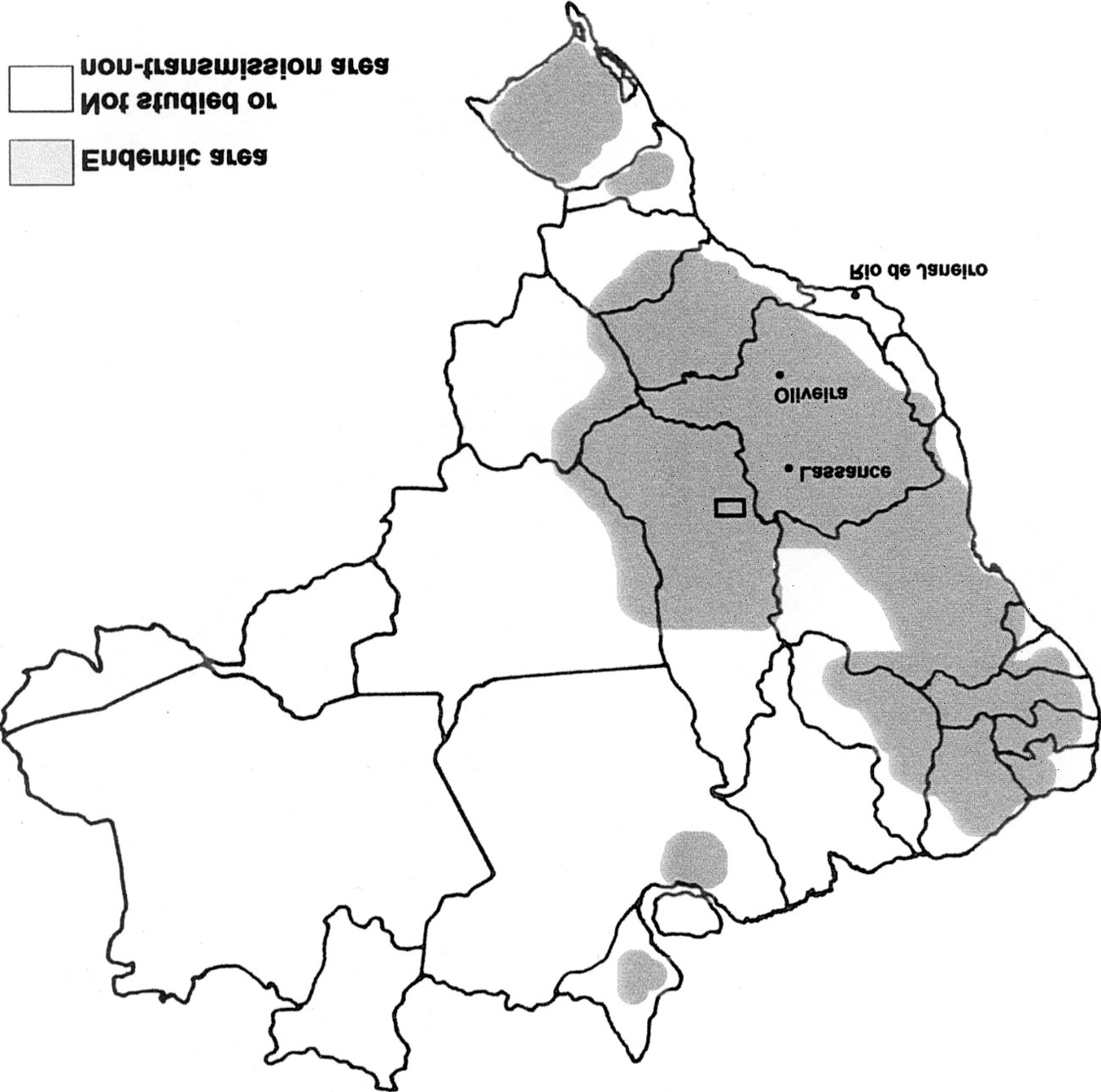
Figure 1. Geographic distribution of Chagas disease in Brazil and main loca-
tions in the history of Chagas disease; the cities of Lassance, Oliveira, and Rio de
Janeiro. Modiªed from D.P. Neves, Parasitologia Humana. Rio de Janeiro: Livraria
Atheneu, 1987: 84.
Manguinhos (Manguinhos Serum Therapy Institute; see ªgure 1). He strained
night and day with his colleague Belizario Penna against the scourge of
malaria. The construction of the Central do Brazil railroad had been inter-
rupted due to a malaria epidemic.1 Among the acquaintances that Chagas
made in Lassance was Cantarino Motta, chief-engineer of the construction,
who had requested health care intervention on his malaria stricken work-
ers. In 1908, Cantarino intruduced Chagas to a blood sucking insect that
preyed at night on the people of that region. Chagas was quiet and
1. See Chagas’ ªrst report about Lassance (Chagas 1907a).
Perspectives on Science
449
thoughtful that night while he listened to Cantarino as the engineer de-
scribed the strange symptoms that affected those people.2
Months later, in February 1909, Chagas published the ªrst of a series of
articles on what later became known as Chagas disease.3 He described a
trypanosome, a protozoan that invaded human cells. He described the in-
sect that transmitted it to humans and he described a complicated set of
symptoms that characterized the parasitic infection. He had discovered a
new tropical disease.4 In 1910 he was named member of the National
Academy of Medicine in Brazil. In 1912 he received the Schaudinn prize
in Hamburg, the most important award in parasitology at the time. Na-
tionally and internationally acclaimed for his discovery, Chagas became a
hero.
A decade after the German award, however, the existence of the disease
itself was challenged in the highest forum of Brazilian medicine, the same
National Academy of Medicine that had acclaimed him earlier. Chagas de-
fended himself against an angry group of physicians who claimed the
trypanosome was not really pathogenic, that the symptoms which Chagas
had described were doubtful, and that the discovery was not even his own
work.5
Finally, in 1933, E. Villela realized that thousands were dying of Cha-
gas disease in Belo Horizonte, close to Lassance, without even being diag-
nosed. The disease had disappeared from the minds of Brazilian doctors.6
How could a disease be so successfully “invented”7 from scratch, imme-
diately receive accolades at home and abroad, and yet soon after be so eas-
ily disqualiªed? In this paper, we explore the strange circumstances sur-
2. See Carneiro (1963), pp. 7–10; Carlos Chagas Filho (1974).
3. The ªrst article mentioning what later became Trypanosoma cruzi was “Neue
Trypanosomen.” Archiv für Schiffs-und Tropenhygiene 13 (1909), 120.
4. Chagas disease is, even now, an important tropical disease. It is caused by the parasite
Trypanosoma cruzi, a ºagellate of the Kinetoplastida Order, Family Trypanosomatidae. It is
transmitted by triatomine blood-sucking insects. According to the World Health Organi-
zation, it now affects 16 to 18 million people in South America. In spite of the successful
control programs developed recently, 25% of the Latin American population is presently
considered at risk. See WHO, http://www.who.int/ctd/html/chagcsstrat.html. The infec-
tion is complex. After the short acute phase, it develops into a chronic stage in which dif-
ferent syndromes might emerge. After several years, 27% of those infected develop cardiac
problems which may lead to sudden death, 6% develop digestive damage, and 3% present
peripheral nervous involvement. At present, Chagas disease has no cure. See World Health
Organization—Division of Control of Tropical Diseases “Chagas Disease Elimination.” See
http://www.who.ch/ctd/.
5. See Carlos Chagas Filho (1974), O. Fonseca Filho (1974).
6. See E. Villela (1930).
7. The term “invention” is used by Chagas himself to describe his discovery. See Chagas
(1928).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
450
The Rise and Fall of Chagas Disease
rounding the discovery, the initial acceptance and subsequent rejection of
Chagas disease. We examine the peculiar sequence of events leading to the
“invention” of the disease. The vector and the etiologic agent, for instance,
were discovered before the actual symptoms. We also examine the wider
context for the recognition of Chagas’ work. The discovery satisªed the
demands of an international audience focused on understanding the etiol-
ogy of tropical diseases, promoting the speciªcity of these infections, and
articulating the insect-vector theory. Finally, we contrast the conditions
for international acceptance with those that determined its rejection at
home. Chagas’ agenda was to carve a niche for experimental medical sci-
ence in Brazil. This cause did not have a great number of supporters and
never achieved consensus in the country.
In order to put together the pieces of this puzzle, we shall begin our
journey far from where the dramatic construction and de-construction of
Chagas disease took place. We will start in turn-of-the-century Europe,
where tropical medicine was emerging and growing in importance.
Microbes and national imperatives
The history of Chagas disease cannot be understood outside of the history
of early twentieth-century tropical medicine. A radical change in the per-
ception of disease had taken place with late nineteenth-century germ the-
ory. It produced a new scientiªc and optimistic perspective on the diseases
associated with the tropics. Michael Worboys places the emergence of
tropical medicine in the crossing of germ theory and the new require-
ments of “constructive imperialism,” in the turn of the century (Worboys
1976, 1993).
In 1899, P. Manson, a British army physician, deªned tropical diseases
as those caused by protozoan or more complex organisms (Worboys 1993,
p. 518). Such tropical diseases were, for him, necessarily parasitic in na-
ture and depended on a geographically limited factor for transmission.
This deªnition separated the “cosmopolitan” bacterial diseases from the
ecologically limited parasitic diseases. The deªnition was coupled to
the “insect vector theory,” according to which, in parasitic diseases, the
etiologic agent developed one or more stages of its life cycle within an in-
sect vector. This form of transmission would be typical of protozoa or
helminths. Bacterial diseases, instead, would be transmitted by direct con-
tagion. The critical support for this theory was the discovery, between
1898 and 1899, that malaria parasites were transmitted by the mosquito
(Harden 1985; Worboys 1993, p. 514).
Thus, whenever a parasite was involved in a disease, especially a proto-
zoan one, an arthropod vector was also expected. Parasite hunting became
the sport of the season.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
451
Although separated from bacteriology,8 parasitology was emerging and
growing through the emphasis placed on protozoa and worms by the rise
of tropical medicine (Worboys 1983, pp. 10–11). By the late nineteenth
century, the enthusiasm for parasites led to the search for and discovery of
many causative agents and biological cycles of “tropical” diseases. Among
these were the identiªcation of the malaria Plasmodium parasites, by
A. Laveran in 1880; the identiªcation of the malaria insect vector and life
cycle by R. Ross and G. B. Grassi in 1897; the discovery of the causative
agent of Kala azar, Leishmania donovani, by W. B. Leishman and C. Dono-
van in 1900; the identiªcation of the life cycle of Schistosoma worms, that
caused bilharzia, by R. Leiper in 1915; the elucidation of ªlariasis trans-
mission by mosquitoes by P. Manson in 1879; and the discovery of African
trypanosomiasis by Bruce, between 1896 and 1902 (Worboys 1983; Cur-
tin 1989, p. 136; Farley 1991, pp. 45–71; Desowitz 1993, p. 44).9
Causative agents of “tropical diseases” were varied in their taxonomy as
well as their ecology. The ªrst to be studied were parasitic worms. Then
came the malaria family of related human and animal diseases. Trypano-
somes came last, with the ªrst human pathogenic species identiªed only
in 1903 (Worboys 1993). The ªrst trypanosome was found in 1841 in the
blood of a trout, but the ªrst identiªcation of a disease caused by this
group of organisms in mammals was conceived only in 1880, when Evans
observed a tripanosomiasis in equines (Laveran & Mesnil 1904, p. 2).
Laveran and Mesnil argue that it was only in 1897, with Bruce’s study of
Nagana, a disease affecting equines and other mammals, that a ªrst model
of the interaction of these organisms and their hosts was established. In
1899, Rabinowitsch and Kempner did the ªrst cytological study of a
trypanosome and in 1903 Novy and McNeal established a method to de-
velop pure trypanosome cultures in blood-gelatin media.10
8. Institutional aspects of this separation include the disputes between Manson and his
emerging London School and King’s College bacteriologists, who would be willing to bite
into the new and promising tropical medicine ªeld. The convenient compromise was to
consider bacteriology dispensable to a specialty whose objects comprised chieºy protozoa
and worms (Farley 1991, pp. 25–28).
9. There were also important discoveries involving bacterial and viral infections, such
as leprosy, cholera and yellow fever. About them see Worboys (1993, 1983). The obvious
prestige of parasitological tropical medicine and the importance attributed to the discover-
ies related to it is also reºected in the Nobel awards. Among the ªrst ten laureates in medi-
cine and physiology, two were awarded the prize for contributions in tropical medicine:
R. Ross in 1902, and A. Laveran in 1907. Besides these, R. Koch, an important player in
the tropical medicine scene, received the 1905 Nobel prize for his work on tuberculosis.
See the Nobel Foundation Web Site, http://www.nobel.se, last accessed April 27, 1999.
10. This is an important path since the ability to isolate, cultivate in vitro and then
produce an experimental infection was a decisive sequence in the demonstration of the in-
volvement of “germs” in speciªc diseases (Laveran & Mesnil 1904, p. 3).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
452
The Rise and Fall of Chagas Disease
Trypanosomiases were considered to be always tropical. In the begin-
ning of the century an animal disease had been identiªed in South Amer-
ica, at the Chaco region (which includes a part of Brazil). A. Laveran and
F. Mesnil, in their 1904 work, named this the great decade of trypanosome
studies (Laveran & Mesnil 1904).
The late nineteenth and early twentieth century witnessed the estab-
lishment and rapid growth of an international institutional network for
tropical medicine. Schools, departments, and institutes of tropical medi-
cine were founded by the major colonial powers. In 1899, the ªrst such in-
stitutions were established in England: the London School of Tropical
Medicine and the Liverpool School of Tropical Medicine. Following that,
in 1900, The ªrst American tropical medicine institution was founded at
Harvard University;
in 1901 the Institut für Schiffs- und Tropen-
krankheiten was founded in Hamburg, Germany, and in the same year
Paris had its Institut de Médecine Coloniale. More chairs, schools, and in-
stitutes were subsequently created in the United States, Germany,
Brussels, and the Netherlands (Worboys 1993, p. 520).
While the inevitable rivalries between competing colonial powers took
place, there was also sharing of a common intellectual background. Inter-
national meetings and awards were opportunities for such exchanges, in-
cluding the International Sleeping Sickness Conference in London in 1907
(Worboys 1994, p. 98), the International Conferences in Hygiene and the
Schaudinn prize, awarded by the Institut für Schiffs- und Tropen-
krankheiten in Hamburg for important contributions in protozoology
every four years.
Tropical medicine became a leading specialty in the medical sciences.11
Several discoveries in Tropical Medicine were made by army doctors or
in imperial colonial medical services (Despowitz 1993, pp. 40–59, 165–
167; Worboys 1993). Schools of tropical medicine were imperial business,
justiªed by the necessity to care for the health of white settlers or to con-
trol urban epidemics that threatened colonial affairs. Tropical medicine
and public health were largely military issues. Farley describes, for exam-
ple, the invasive health care measures adopted by the United States during
the cholera and plague epidemics in the Philippines in the beginning of
the century as strictly a war action, with the isolation of infected people in
“detention pavilions” and strong repression (Farley 1991, p. 37).12 Thus,
some understand tropical medicine as scientiªc and technological expres-
sions of early twentieth century European and American imperialism
(Farley 1991, pp. 13–156; Mac Leod 1988; Arnold 1988).
11. See Worboys (1993).
12. See also Arnold (1988, pp. 12–13).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
453
From this perspective, tropical diseases are historically studied as an
European, particularly British (and, to a lesser extent, American) concern.
Worboys suggests that the problems of other regions were overlooked be-
cause metropolitan interests were not directly implicated (Worboys
1993).
In the gradient of medical interest diseases that affected white settlers,
soldiers and indigenous people alike topped the list. Urban epidemics,
such as cholera or plague, required the most stringent sanitary/military in-
tervention. They affected the safety of white settlers and, therefore, of the
empire. They could affect trade. Rural endemic diseases elicited a lesser
reaction since they affected only poor indigenous people. However, they
could impair colonization projects, such as railroad construction, agricul-
ture, etc. Subsequent historical interest reºects this gradient.13
An atypical discovery
Given these determinants of historical interest, Chagas disease never re-
ceived much attention. It was not important during the period when most
historical writings were celebrations of heroic metropolitan deeds. It was-
n’t highlighted in the following, more critical periods in medical histori-
ography either, because Brazil was not a colony by the end of the nine-
teenth century.
The history of Chagas disease is undeniably a part of the early history of
tropical medicine-parasitology, sharing determinants, intellectual milieu,
and theoretical assumptions with most other episodes. It is, however, his-
torically atypical. Whereas most diseases discovered in the period affected
European colonies, Brazil was an ex-colony.14 Unlike other colonial pow-
ers, Brazil’s former metropolis, Portugal, was scientiªcally backward.
The war against tropical diseases was part of the agenda of imperialism.
However, in Brazil, tropical medicine was associated with interests of na-
tionalist elites struggling to fulªll the requirements of economic develop-
ment and meeting the cultural standards of the “civilized world” through
the establishment of scientiªc and higher education institutions.15
Another discrepancy between the history of Chagas disease and that of
other tropical diseases concerns its discoverer. Chagas disease was discov-
ered by a Brazilian physician, with no training abroad and no connection
with military institutions.
13. See, for example, Farley (1991, pp. 3–4).
14. African colonies dealt with Bilharzia, Asian and African colonies with malaria, In-
dian and other Asian colonies with Kala azar. See Farley (1991, p. 6) and Desowitz (1993,
p. 34).
15. About the interests related to the early establishment of scientiªc and higher edu-
cation institutions in Brazil, see Schwartzman (1991, pp. 50–59).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
454
The Rise and Fall of Chagas Disease
The discovery itself was unlike other such discoveries: usually, diseases
were recognized as morbid entities, an etiologic agent was discovered
(sometimes followed by some years of controversy about its life cycle), and
then the arduous task of searching for the vector began. Sometimes this
took decades.16 By contrast, the discovery of the causative agent of Chagas
disease, Trypanosoma cruzi, of its vector, a blood sucking insect, and the
clinical description of the disease were all done in the same year: 1909.
Previous accounts of the discovery and early research on Chagas disease
are largely “heroic” re-constructions made by early twentieth-century Bra-
zilian parasitologists. Other commentators follow a similar line17: Chagas
was depicted as favored by chance because he was a “genius,” a prepared
researcher or a competent protozoologist; his reasoning took him from the
insect to the disease through a series of sequential inferences.
Later, historians attempted to provide different, and more critical, in-
terpretations. N. Sepan’s analysis of the institutional context of early cen-
tury Brazilian biomedical sciences includes comments on Chagas’ discov-
ery. She describes it as an example of biological research resulting in a
discovery of practical importance, where most of the concepts involved
were already elaborated by European scientists. According to her account,
Brazilian researchers only have followed established lines and Chagas rea-
soned by analogy with the malaria model as to the role of the blood suck-
ing insect in the transmission of a disease (Stepan 1976, pp. 118–20).
More recently, F. Delaporte presented another reconstruction. His
claims are as follows: (1) In Lassance, Chagas was actually trying to eluci-
date the cycle of a non-pathogenic parasite that affected monkeys—
Trypanosoma minasense—when he accidentally came across T. cruzi. Since
16. The etiological agent of Bilharzia, caused by worms of the genus Schistosoma, was
discovered between 1851 and 1852 by Theodor Bilharz, who identiªed the worms and
their eggs. The life cycle and species were not correctly identiªed until 1915. See Farley
(1991, p. 70). The parasite that causes Kala azar, the scourge that tormented Asia in the
late nineteenth century, was discovered in 1900 by Leishman and Donovan. It took addi-
tional years to correctly identify it as a protozoan of the genus Leishmania. Twenty six years
later the sandºy Phlebotomus argentipes was recognized as its vector and the transmission
mechanism became known only in 1940 (Desowitz 1993, p. 58). Malaria was known as a
disease from ancient times. The causative agent for malaria was ªrst observed in 1880 by
Laveran, but the transmission by the mosquito was only established in 1897 by Ross.
17. See for example Dias (1994), Carneiro (1963), Chagas Filho (1974), Fonseca Filho
(1974, pp. 43–66). Emanuel Dias was a Manguinhos physician and researcher, active from
the 1930s on. Emanuel Dias was a key ªgure in the restoration of the interest in Chagas
disease with his research on chagasic cardiopathy and his public health initiatives. Carneiro
was an observer during the Academy debate. Chagas Filho is Chagas’ son and Fonseca Filho
was part of the Manguinhos team and a defender of Chagas during the “Academy debate.”
English language accounts with a celebratory tone include: Kean (1977), Lewinsohn
(1979), Lewinson (1981).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
455
T. minasense would have been his real “research line,” he had ignored the
hematophagous (blood-sucking) fauna of the region; (2) When he dis-
sected the insects and observed parasites in their guts, he believed them to
be developmental forms of T. minasense; (3) He sent the infected insects to
O. Cruz, director of the Serum Therapy Institute of Manguinhos in Rio de
Janeiro, looking for conªrmation of his beliefs; (4) Cruz tested the insects
and rejected Chagas’ hypothesis. Chagas realized he was mistaken and that
Cruz had the opportunity to make a discovery. He made changes in the re-
ported periods of observation of blood forms in laboratory animals so as to
make the observation coincide with his presence in Rio and grant him the
discovery; (5) Since the new parasite was pathogenic, Chagas produced a
hurried description of symptoms in analogy with sleeping sickness
(Delaporte 1994/95).
M. Perleth has studied the inºuence of the German Schaudinn school of
protozoology on Chagas’ work and suggested that
Chagas’ description of American trypanosomiasis of 1909 is a
reºection of the Schaudinn School of protozoology (Perleth 1997,
p. 92).
Stepan, Delaporte and Perleth describe and interpret the discovery of
Chagas disease according to one or another version of the “diffusion
model.”18 According to it, “non-scientiªc societies” are seeded with West-
ern science and gradually grow autonomous, until they can ªnally break
loose of the colonial umbilical cord. They grow from total reliance upon
“central” (European or American) institutions and ideas to an ideal stage
of independence and self-reliance (Basalla 1967). The problem with this
model is that it does not ªt reality. First, “non-scientiªc societies” are not
passive recipients of “western science”—there is a great deal of manipula-
tion and originality from early stages.19 Second, science does not “natu-
18. The version sketched and criticized here is taken from the most cited work about
this model, G. Basalla’s (1967) “The Spread of Western Science.” Stepan comments on this
model (Stepan, 1976, pp. 14–20) and “employs” it throughout her book (p. 36 and p. 79,
for example). She remarks, however, that the increasing inter-dependence of scientists in
later stages does not ªt Basalla’s model, with which she otherwise agrees. Perleth explicitly
adopts Basalla’s model. See Perleth (1997, p. 60).
19. About colonial science and early attempts to make original contributions in Span-
ish America, see J. Canizares Esguerra “Spanish America” (n.d.) and Canizares Esguerra
(1999). About yellow fever in Brazil and the theories around it, see Chalhoub (1993).
Original and pioneering contributions in Tropical Medicine from Brazilian physicians in
the XIXth century were actively disregarded by Europeans. J. Peard (1997) describes them
and claims: “One of the most interesting critiques leveled at traditional medical historians
is that they concentrated only on the outward movement of Western medicine from its
metropolitan centers; they failed to ask how medicine practiced in faraway places subtly al-
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
456
The Rise and Fall of Chagas Disease
rally” evolve to a stage of autonomy and isolation.20 In consequence, we are
left with only one disconcerting alternative describing everything that is
done by non-central scientists as imitation of their central colleagues
(since independence never happens).
Diffusion takes for granted that everything in the “non-scientiªc” soci-
ety’s science must have been passively fertilized by someone “central.” The
only question is: who is the father? I. Löwy, for example, claimed that the
Pasteur Mission working in Rio de Janeiro from 1901 to 1905 was the fa-
ther of the Brazilian Tropical Medicine baby.21 Extended to the level of the
individual scientiªc accomplishment, the result is “imitation,” “analogy,”
and “reºection.” In the discovery of Chagas disease, Stepan saw an analogy
with the malaria model, Delaporte saw an analogy with the sleeping sick-
ness model and Perleth saw the reºection (imitation) of a German school.
No space is left for active participation and originality.
All practitioners of Tropical Medicine were working under a common
conceptual framework that included the insect-vector model. Chagas was
as much an imitator as were Leishman, Donovan or Bruce.22 Nevertheless,
no one has ever felt the need to explain away their discoveries.
In this paper, we offer a more detailed description and a different inter-
pretation of Chagas’ discovery. We depict him as an active participant, al-
though an atypical one, in the enterprise of Tropical Medicine. We claim
that only a proper understanding of this participation can account for his
unusual sequence of hypothesis, as well as his moves.
Chagas and Manguinhos
Chagas was born in 1879 in the city of Oliveira, Minas Gerais. He studied
medicine in Rio de Janeiro—then the national capital—from 1896 to
1901. His graduating hematology thesis was developed in the
tered and adapted Western medicine to local milieux and, in turn, often inºuenced medi-
cal thinking in the metropolitan centers.” See J.G. Peard (1996, 1997).
20. Actually, this condition requires active measures at the economic and political
level. And when this happens, the picture is not one of a blooming local scientiªc culture,
but one of decadence and mediocrity. About Venezuela, see H. Vessuri (1991) and T. Glick
(1984); about Brazil, see Schwartzman, (1991, pp. 237–247).
21. Regarding the Pasteur Mission, I. Löwy claims that “The temporary transfer of a
“model” European laboratory to a developing country may be related to the fact, unusual
in a peripheral country, that a Brazilian scientiªc institution, the Instituto Soroterapico de
Manguinhos (later, Instituto Oswaldo Cruz), was able to attain an international reputation
as an important centre of research in tropical medicine between 1910 and 1930.” Löwy is
not able to provide evidence, however, for the actual training of the Manguinhos scientists
by the French mission. The French mission did not transfer its laboratory equipment to
Manguinhos, nor did it employ Manguinhos personnel. See I. Löwy (1990).
22. M. Worboys, who is not concerned with diffusion, mentions Chagas’ discovery in
his work about tropical diseases and suggests that “In this case, the parasite-vector model
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
457
Manguinhos Serum Therapy Institute and was about malaria. He did not
remain in Manguinhos on that occasion and worked for some time in pri-
vate practice (Chagas Filho 1993, pp. 3–48). His relationship with the Se-
rum Therapy Institute, however, was soon re-established through its ma-
laria control programs.
Chagas was committed to academic work very early. His ªrst interest
was obviously malaria (Chagas 1905, 1906). In 1907 he identiªed new
species of mosquitoes, the vectors in malaria transmission (Chagas 1907b,
1907c, 1907d). In 1908 he published his ªrst paper in an international
journal (Chagas 1908a). He emerged as the highest Brazilian authority on
malaria and was a pioneer of its control.23
Chagas was part of the team at Manguinhos Serum Therapy Institute,
which was considered to be the ªrst reference center in Brazilian experi-
mental medicine. This Institute was created to produce anti-plague serum
when the country was threatened by an epidemic. It was inaugurated in
1900 and in 1902 Oswaldo Cruz was named director of the Institute.24
Manguinhos had a controversial as well as spectacular impact in the
area of urban sanitation. The calamitous sanitary situation drove president
Rodrigues Alves to centralize the sanitary services in a Federal Depart-
ment of Public Health. Its immediate task was to control urban epidem-
ics, like yellow fever and smallpox, and to prevent the emergence or ag-
gravation of other diseases, like plague. Oswaldo Cruz, already in charge
of the Serum Therapy Institute, was named director of the Federal Depart-
ment in March 1903. He proposed a bold plan to control yellow fever,
smallpox, and plague. It included an incisive intervention in Rio and im-
portant new actions at the Federal level. The program was presented by
Rodrigues Alves as a new sanitary law and elicited strong opposition from
different political segments, as well as from the population, whose daily
life was affected. It included the uniªcation of sanitary services, the adop-
tion of a uniªed sanitary code and compulsory vaccination. The reaction
against Cruz’s program was so strong that force was required to prevent
conºict. In 1905 Cruz announced that the yellow fever epidemic had been
controlled. By the end of 1906, Cruz, an obscure scientist in 1903, was ac-
identiªed a pathogen and its mode of transmission before the disease syndrome was de-
scribed clinically” (Worboys 1993, p. 528).
23. See Fonseca Filho (1974, p. 19).
24. Other enterprises involving a scientiªc approach to public health emerged in the
state of São Paulo during the last years of the nineteenth century, also related to the control
of endemic diseases such as smallpox, cholera and malaria. See Schwartzman (1991,
pp. 83–91). Similar experiences were being developed in other parts of Latin America,
with the emergence of their ªrst science pioneers and the articulation of basic research with
applied activities. See M. Cueto (1989a).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
458
The Rise and Fall of Chagas Disease
claimed as a national hero and internationally recognized as the man re-
sponsible for the improvement of Brazil’s public image. Meanwhile, as a
result of Cruz’s new powers, the internal conditions in Manguinhos im-
proved dramatically. The team of researchers increased in number, new in-
stallations were built and the general infrastructure was enhanced. The
deeds of the Institute received national and international recognition
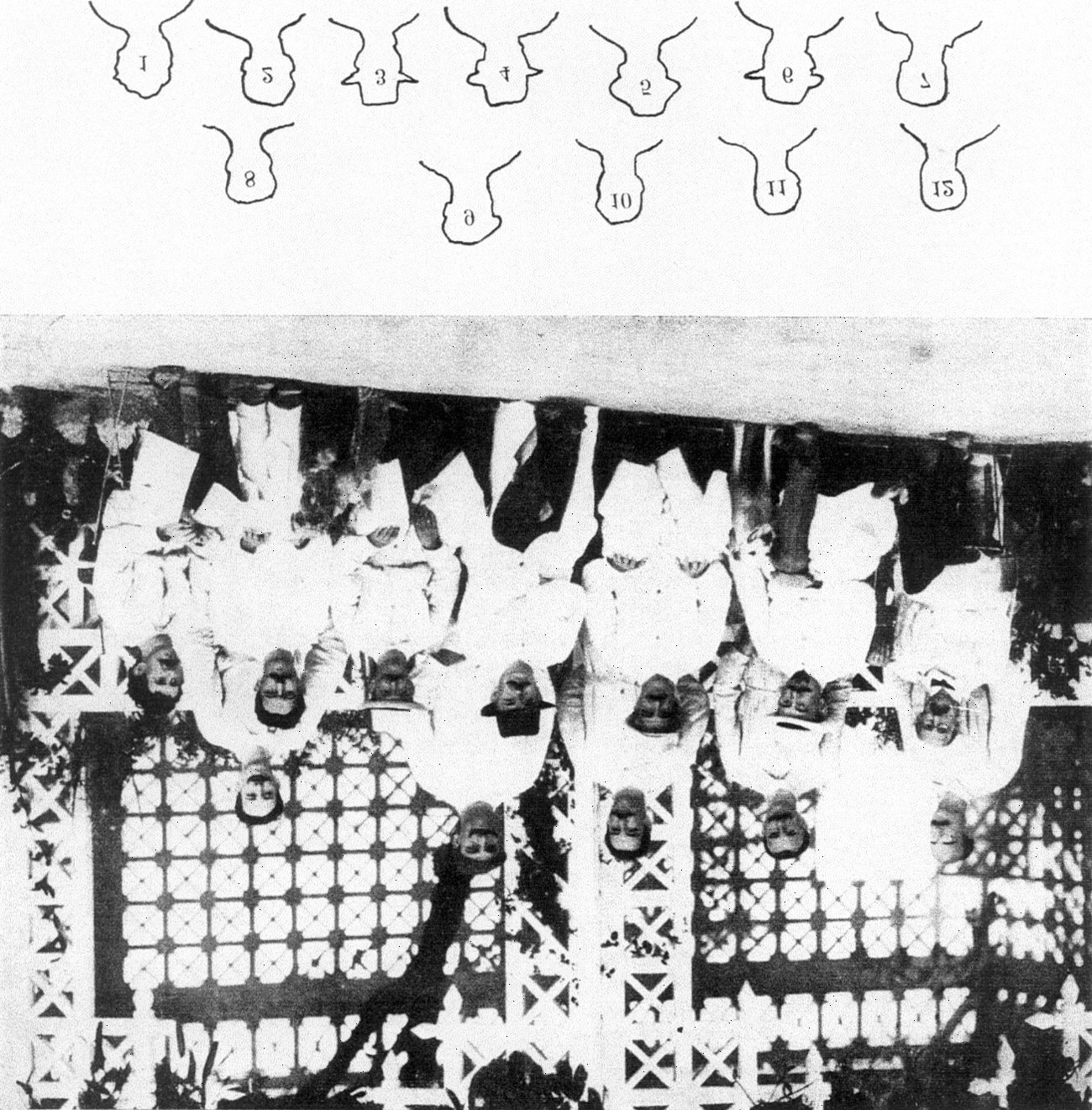
(ªgure 2).25
that,
original
Following
contributions
in microbiology
and
protozoology in Manguinhos received attention from renowned research-
ers in central scientiªc institutions.26 Stanislaus Von Prowazek, G. Giemsa
and Max Hartmann came to Brazil between 1908 and 1909. Prowazek
and Giemsa were professors at the Hamburg Institute of Tropical Medi-
cine (Institut für Schiffs—u. Tropenkrankheiten, Hamburg). Hartmann came
from the Berlin Institute of Infectious Diseases (Intitut für Infektions-
krankheiten).27
Prowazek and Hartmann had been interested in ºagellates in general
and trypanosomes in particular for a long time. Their early work on
trypanosomes had been published in 1905 and 1907 (Prowazek 1905;
Hartmann & Prowazek 1907). In the 1907 paper they discussed the roles
insisted upon by
of certain cellular organelles. Their main theses,
Hartmann in 1907 (Hartmann 1907) and by Hartmann and Chagas in
1910 (Hartmann & Chagas 1910), was the presence of two nuclei in pro-
tozoa. In their view, protozoa carried a nuclear structure responsible for lo-
comotion and another structure—a “trophic” or “generative” nucleus—
which would be the main nucleus.
To articulate their theses, Hartmann and von Prowazeck were hunting
for parasites, much like everybody else in tropical medicine. Manguinhos
25. Brazil was invited to participate in the XII International Conference in Hygiene
which took place in Berlin, in 1907. Manguinhos reported new species of mosquitoes (vec-
tors in many tropical diseases such as yellow fever and malaria), by A. Neiva, the discovery
of the exo-erythocitic cycle of Haemoproteus columbae, by Aragão and anti-malaria cam-
paigns, by Carlos Chagas. Because of all its deeds, Manguinhos received the gold medal
conferred by the judges in Berlin. See Stepan (1976, pp. 98–99).
26. One remarkable example of such contributions is the identiªcation of the exo-
erythocitic cycle of Haemoproteus columbae. This protozoan parasite was known to infect pi-
geon red blood cells and its sexual reproduction had been identiªed years before. Neverthe-
less, nothing was known about the asexual reproduction in the vertebrate host. H. B.
Aragão, a Manguinhos researcher, showed that it took place at the pulmonary endothelium
by a process called “schizogony.” See Henrique de Beaurepaire Aragão (1907). This work
had obvious repercussion as to the understanding of malaria and Aragão’s discovery was ac-
claimed worldwide. At the same time, yellow fever was being studied by other researchers.
See Fonseca Filho (1974, pp. 42–43 and pp. 32–33).
27. See Jaime L. Benchimol (1990, pp. 45–6).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
459
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Figure 2. Manguinhos in 1908. 1. Alcides Godoy; 2. José Gomes de Faria; 3.
Antonio Cardoso Fontes; 4. Max Hartman; 5. Oswaldo Cruz; 6. Stanislas von
Prowazek; 7. Adolpho Lutz; 8. Carlos Chagas; 9. Henrique da Rocha-Lima; 10.
Henrique Figueiredo de Vasconcelos; 11. Henrique Beaupaire Aragão; 12. Arthur
Neiva. From O. da Fonseca Fo. A Escola de Manguinhos. São Paulo: Fundação
Oswaldo Cruz, 1974, p. 23.
was as good a place to be: it was in the tropics, it had become an impor-
tant center for urban sanitation and it was becoming prominent for its sci-
entiªc endeavor in experimental medicine.
Around the middle of the decade, Manguinhos opened the era of
rural endemic diseases. The new focus responded to demands from govern-
mental and private companies whose activities in rural Brazil were be-
ing hampered by the unsanitary condition of their workers (Fonseca Filho
1974, p. 19). The main problem was malaria. Around 1906 the con-
460
The Rise and Fall of Chagas Disease
struction of a hydro-electric plant in Itatinga (state of São Paulo) was sus-
pended due to a malaria epidemic among the workers. The company
in charge—Companhia Docas de Santos—resorted to Carlos Chagas. He
carried out the ªrst anti-malaria campaign in Brazil. Soon after, Chagas
engaged in a similar job in the state of Rio, where the water supply
was being increased. With the experience and authority achieved
by two successful campaigns, Chagas was assigned yet another task.
Malaria was obstructing the construction of an important railroad
that was to extend the access to the hinterland by train. The company
in charge—Estrada de Ferro Central do Brazil—again requested the
help of Manguinhos professionals and Chagas was sent to Lassance, in
the state of Minas Gerais. In the beginning of the century, its inhabit-
ants were affected by malnutrition, syphilis, ancylostomiasis (hookworm
infection), endemic goiter and—of course—malaria and American
Trypanosomiasis.28
A journey to the middle of nowhere
Chagas arrived at Lassance early in June of 1907 with Belizario Penna,
who also worked in Manguinhos. He described his ªndings and ªrst steps
in a report addressed to the sub-director of the sixth division of the
Estrada de Ferro Central do Brazil, in January 25, 1908.29 He found that
most workers were infected with malaria and many of them had severe
symptoms. Chagas and Belizario set up their operations in a wagon that
moved along the railroad.30 Most of the time, they were very busy with
their anti-malaria affairs. Nevertheless, in that same year, as a good para-
site hunter, Chagas identiªed a trypanosomatid parasite in the blood of a
monkey he called Hapalle penicillata.31 He named the parasite Trypanosoma
minasense and wrote a small note on it December 15, 1908. In this 1908
note, however, Chagas mentioned not one, but two trypanosomes. He felt
conªdent about the taxonomic identiªcation of one of them, but not about
the other:
We are currently studying two trypanosome species, both from the
Hapalle penicillata. The ªrst one is a habitual parasite of the Hapalle,
being found in almost all the animals in certain regions. […] Of
28. See Chagas Filho (1993). The general epidemiological condition was also described
by J.C. Dias (1995).
29. This report is reproduced as “‘Adenda: Lassance,’ 1907, Carlos Chagas” (Chagas
1907a).
30. See Carneiro (1963, p. 8).
31. And, afterwards, Callitrix penicillata.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
461
the other trypanosome species, whose life cycle presents great inter-
est, we will later give description.32
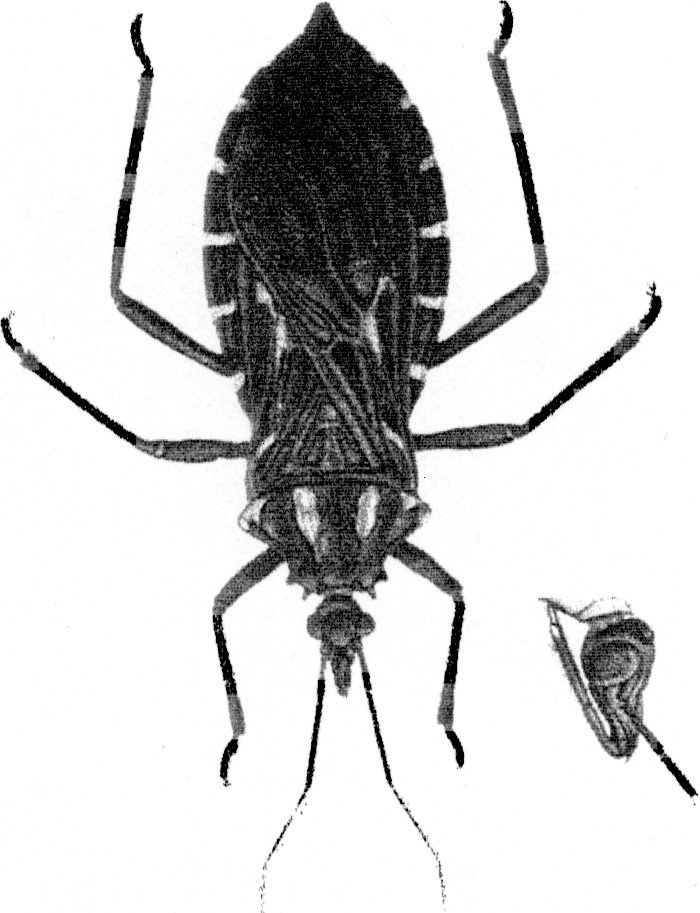
Chagas was led to his famous discovery through his introduction to the
vector, a triatomine insect (ªgure 3A). He was ªrst shown one in a visit to
Cantarino Motta, engineer in charge of the construction team of the rail-
road works in Pirapora in 1908, one year after his arrival in Lassance. The
second tripanosome mentioned in the Brazil Medico note on T. minasense
was already T. cruzi: two days after the Brazil Medico note, Chagas sent an-
other note to the Archiv für Schiff und Tropenhygiene (dated December 17,
1908). This time, it contained a brief account of T. minasense and a rich
and speculative description of Trypanosoma cruzi (Chagas 1909a). There-
fore, Chagas became acquainted with T. cruzi between June and November
1908. By early December, he knew that his parasites did not belong to the
same species. But little is known about the circumstances of the minasense
discovery. Both notes are brief and nothing can be inferred from such doc-
uments.
Cantarino Motta was a key factor in the story. The engineer, more
familiar with the habits of the local population (he had been there since
1902), showed a blood sucking hemipteran insect to Chagas. Local people
called this insect barbeiro—the “barber.” The insect apparently was nick-
named after barbers, who, in the hinterland, performed bleedings and ap-
plied leeches with therapeutic purposes.33 In an interview to a newspaper
of the state of Paraná, in 1955, Motta claimed that he also suggested a re-
lation between the insects and “some disease.” He claimed to have told Cha-
gas about a coincidence of goiter and idiocy in people and the occurrence
of the insect in the house. The insect dwelt in the interstices of wood and
earth walls (ªgure 3B). Chagas reportedly remained silent and thoughtful
after the engineer’s remarks (Carneiro 1963, pp. 8–10). The exact content
of that conversation is probably lost forever, but we do know that Chagas
promptly dissected the insect and examined the contents of salivary
glands and digestive tract (Chagas 1922). Moreover, he never abandoned
his belief in the relation between trypanosome infection and goiter, al-
though he never succeeded in gathering conclusive evidence for it.
He tentatively identiªed the insect as an hemipteran of the family
Reduviidae and of the genus Conorhinus. In the dissected digestive system
of the insect, Chagas found protozoa of crithidia form in the posterior in-
32. Chagas published two short notes on Trypanosoma minasense. See: Chagas (1908b),
and Chagas (1909a). The ªrst note is dated December 15, 1908. The second is dated De-
cember 17 and was published in February 1909.
33. See Chagas (1910).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
462
The Rise and Fall of Chagas Disease
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
Chagas,
Figure 3. A. The “barbeiro” (the insect vector of Chagas disease).
B. Wood and earth houses where the barbeiro feeds on human blood. From
Lima, Amerikanische
C.
Trypanosomenkrankheit. Chagas-Krankheit. In: C. Mense, ed., Sonderabdruck aus
Handbuch der Tropenkrankheiten. Leipzig: Verlag Von Johann Ambrosius Barth,
1929: 673–728, p. 675 and p. 676.
E. Villela & H.
da Rocha
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
463
testine of the insect (Chagas 1922). Chagas reasoned that either these were
normal parasites of the insect or intermediary forms of a parasite with a
complex life cycle, a vertebrate hemoºagellate (Chagas 1922). On the one
hand, he suspected that the crithidia could be intermediate forms of his
T. minasense, which he already knew to be an endemic vertebrate
hemoºagellate in that region (Chagas 1911; 1922, p. 68). On the other
hand, Chagas frequently stressed the association between man and insect,
which strongly suggested that man was the vertebrate host (Chagas
1909b, 1909c,34 1910). At any rate, he sent the insects to Manguinhos to
be tested. They were used by Cruz in experimental infection in many ani-
mals. Blood forms were detected in those animals after a period that
ranged from 20 to 30 days. The experiments showed not only that the
morphology of the blood forms of the parasite was very different from the
previously identiªed T. minasense but also that the laboratory animals de-
veloped certain speciªc symptoms associated with a disease. The whole ex-
perimental procedure lasted “some months” and was concluded in April
1909 (Chagas 1910).
Chagas, who had followed his insects to Manguinhos, in Rio de Janeiro,
soon after sending them, returned to Lassance. He had a disease in hand—
hopefully, a human disease. He assumed that the insect was domiciliary
and proceeded to search for infected domestic mammals in the region.35
He obviously searched for infected humans as well. First he found the par-
asite in domestic animals—cats and dogs—but ªnally he came across a
sick child in fever with free trypanosomes in the blood. The ªrst paper re-
porting the human blood forms of this speciªc patient is dated April 15,
1909. In this paper, Chagas made a tentative clinical picture of the dis-
ease. Its symptoms included acute anemia, marked organic decay, sub-
palpebral edema, frequently general edemas and considerable ganglion
swelling with large ganglions in peripheral pleads. He observed atrophy
in development in certain children and reported acute cases with fever and
other morbid manifestations.
In a more detailed paper, Chagas described the pathogenic
trypanosome. He examined the parasites in human patients and laboratory
animals, monkeys and guinea pigs. The parasites thus found are called
34. This paper was published in Portuguese and German, side by side in different col-
umns.
35. Chagas was convinced that the insects were exclusively domiciliary. Actually, they
were not. The hemipteran he found in Lassance was later identiªed as Panstrongylus
megistus, one of the possible vectors in the transmission of American tripanosomiasis. Un-
like Triatoma infestans, another triatomine vector, megistus is not exclusively domiciliary nor
are its domiciliary populations large. Chagas (1909c, 1910, 1922). About the vectors, see,
for example, H. Lent & Wygodzinsky (1979).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
464
The Rise and Fall of Chagas Disease
“blood forms.” He observed the parasites in naturally infected and labora-
tory infected triatomine insects. These parasites are called “insect forms.”
He conducted experiments on infection—both blood forms and insect
trypanosome infection in various laboratory animals—and he cultured the
parasites in the laboratory. After that, Chagas described the morphology
and biology of his parasites. To describe the morphology, he reported in
vivo observations and other microscopic studies in ªxed preparations using
more than one technique (Chagas 1909c).
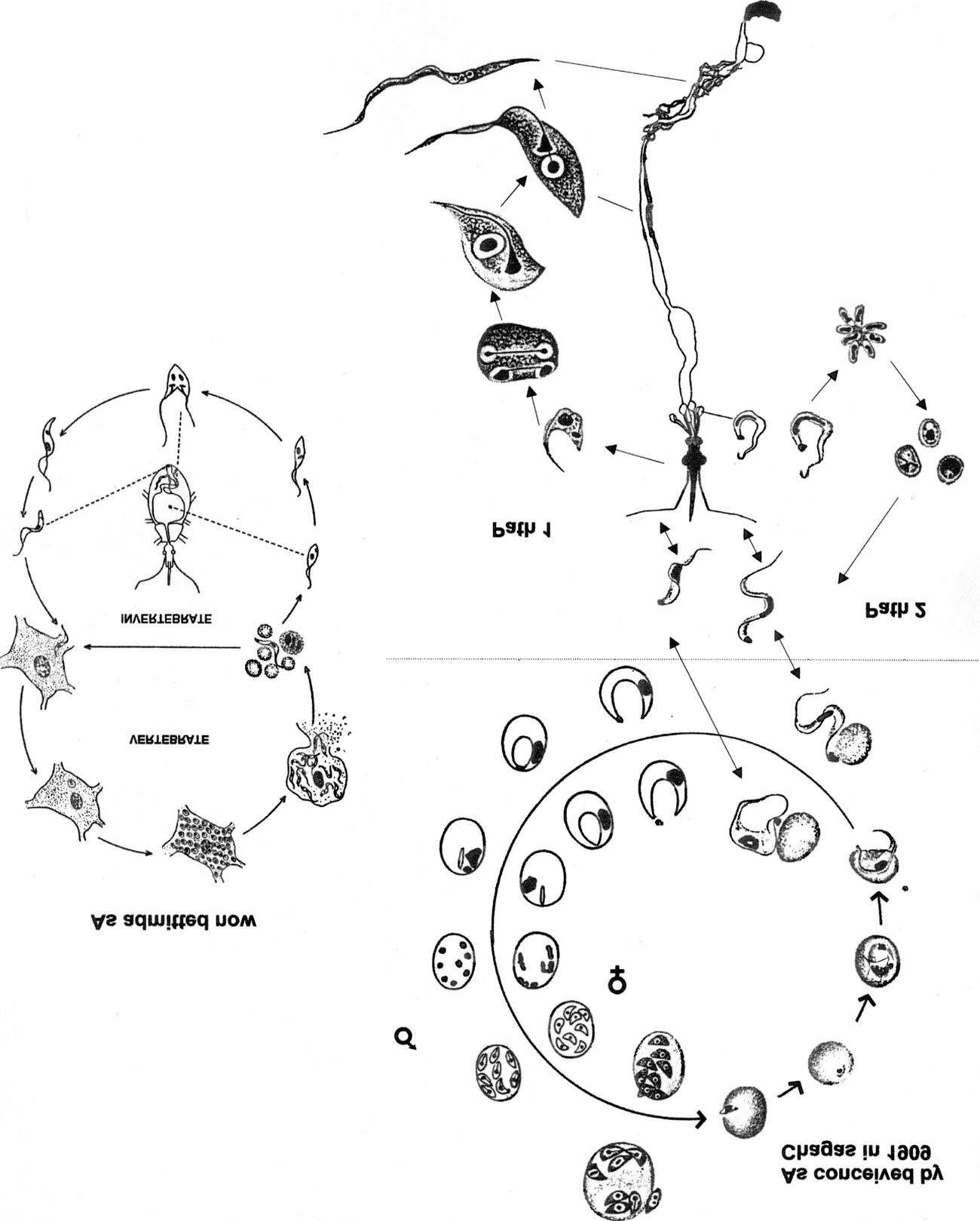
What Chagas’ experiments showed him was a parasite with two
different developmental paths inside the vertebrate host and inside the
insect. Figure 4 depicts Chagas’ model
for T. cruzi’s development.
In the vertebrate host, it had a malaria-type cycle inside blood cells, as
well as schizogonic reproduction. It also had a development path lead-
ing to the fusiform infective forms. In the insect, the parasite could ei-
ther adopt a “culture”-like reproduction behavior that apparently had
no relation to infection, or it could follow the path leading to infective
forms.
Chagas made sure that the insects were parasite free before feeding
on infected blood. He also tried to show that there was no mechanical
transfer of parasites, but a true parasite-vector biological relation-
ship, since insects which had been fed infected blood for less than three
days were not infective. On the other hand, they would remain infective
for a very long time (more than twenty days) after being fed infected
blood.
Chagas was also successful in culturing his trypanosomes and in show-
ing the controversial blepharoplast to be a “real” nucleus: it stained like
nucleus and it acted like nucleus in cell division.36
Finally, Chagas claimed that a new taxonomic genus should be created
to harbor his parasite because of the peculiarities of the trypanosome’s life
cycle, where schizogony and intra-globular life are combined with free
ºagellates in blood plasma. He called the genus ‘Schizotrypanum’ and the
parasite ‘Schizotrypanum cruzi.’
Chagas claimed that his work supported the “Schaudinn school” of
protozoology as to the straight taxonomic proximity between trypano-
somes and hematic protozoa such as malaria plasmodia (hemosporidians at
36. The blepharoplast was, for Chagas and Hartmann, the “second” nucleus. It corre-
sponds to the structure we presently call kinetoplast. The kinetoplast is a DNA-containing
structure located at the trypanosome’s single mitochondrion. The size and form of the
kinetoplast varies according to the developmental stage of the parasite. See Z. Brener
(1992).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
465
the time37), and, speciªcally, “Hartmann’s theory” of the structure of the
protozoan cell.38
The new trypanosome and its transmission became the central research
focus in Manguinhos.39
The discovery had great impact. Chagas was immediately acclaimed
a great discoverer at home and abroad. In October 26, 1910, Chagas
was named full member of the National Academy of Medicine.40 Be-
tween 1911 and 1912 Chagas was invited to speak and to receive honors
in Minas Gerais and São Paulo, and his prestige was acknowledged in
the whole country.41 In 1912, the international competition sponsored
by the Institute for Tropical Diseases of Hamburg took place. Every
four years, it granted the “Schaudinn Prize” (in memory of the pioneer
of protozoology) to the most important contribution in protozoology.
Chagas won the award. The competition included eminent researchers
and pioneers, such as Laveran, Leishman, Roux and others.42 In a short
time, American tripanosomiasis was incorporated in protozoology text-
books.43
37. Malaria parasites belonged to the group of hemosporidians in the beginning of the
century. Presently they belong to Sporozoa and Trypanosomes to Mastigophora.
38. The following year Chagas co-authored a paper with Hartmann reinforcing
Hartmann and Prowazek’s thesis of the binuclear nature of protozoa and in 1911 Chagas
published another paper on the structure of protozoa, along the same line. See
M. Hartmannn & Carlos Chagas (1910), and Chagas (1911).
39. Other physicians and researchers concerned with tropical medicine in Brazil joined
the effort as well: in 1910, Antonio Carini, at the Pasteur Institute in São Paulo, found the
lung forms that Chagas claimed to be “schizogonic” forms of the parasite in uninfected an-
imals. This was further studied by H. Aragão, from Manguinhos, who, in 1911, conªrmed
they were not developmental forms of Chagas’ parasite. They were later identiªed as an-
other organism, Pneumocystis carinii. Gaspar Vianna, another Manguinhos researcher, stud-
ied the small, round forms (“leishmania” forms) he found in almost all the tissues of in-
fected animals and showed their role in the reproduction of the parasite in the vertebrate
host (Vianna 1911). See also acknowledgment by Chagas of Carini’s ªndings, as well as of
the contributions of other researchers who studied the new parasite in Chagas (1913).
40. This was done as an exceptional procedure: for someone to be named member of the
National Academy of Medicine, a vacancy had to appear, usually by the death of another
member. See description of Chagas’ nomination in Chagas Filho (1993 pp. 90–91);
Carneiro (1963. p. 24); Carlos Chagas Filho (1974).
41. Chagas spoke at the founding of the Belo Horizonte Medical School, in Minas
Gerais, and in the major medical institutions in São Paulo. The press devoted much atten-
tion to him. See Chagas Filho (1993, pp. 97–98).
42. The other candidates were Ehrlich, E. Roux, E. Metchnikoff, A. Laveran, C. Nicolle
and W.B. Leishman. See Carneiro (1963, pp. 28–30); Carlos Chagas Filho (1974).
43. See, for example, M. Hartmannn & C. Schilling (1917) and R.W. Hegner & W.H.
Taliaferro (1925).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
466
The Rise and Fall of Chagas Disease
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
467
Figure 4. The cycle as proposed by Chagas in 1909. The infective forms of the
parasite would be inoculated into the blood of a vertebrate where they would
quickly reach the lungs. There, a complex set of transformations and the type of
multiplication known as “schizogony” (where the nucleus divides before the rest
of the cell becomes segmented) would take place. Chagas believed the different
forms exhibited by the parasite in all stages were male and female forms. They
would undergo different transformations. The product of schizogony would be
small claviform organisms that would be able to invade red blood cells. There
they would develop into mature parasites swimming in the plasma. These would
either undergo schizogony in the lungs again, or be ingested by the blood sucking
insect.
In the insect, the parasite would present two types of development: the ªrst
one (PATH 1) would be merely “culture” growth, with no signiªcance as to the
infection of the vertebrate host. Here, ingested parasites would lose their ºagella
and would become increasingly rounded. They would then undergo successive bi-
nary divisions. From this stage they would transform into crithidia-like forms
which would also be able to divide. PATH 2 is inferred by Chagas from the
rounded forms he interprets as products of sexual activity: ingested parasites
would mate, an activity not actually observed by Chagas. As a result, these
rounded forms (interpreted as “ookinets,” the name for a product of fecundation)
would be formed. They would then undergo schizogony. All this would take place
at the insects’ mid-gut. Following that, the small resultant parasites would de-
velop into fully infective forms, which would then migrate to the salivary glands,
passing through the general cavity. Infection would take place as parasites were
inoculated into the vertebrate by the sting.
The cycle ªgure is a reconstruction made by the authors. Cell drawings were
cut from Chagas’ original papers and re-arranged.
The modern cycle is depicted on the left side of the page. On the vertebrate
host, infective forms (either blood or insect forms) invade cells and become
rounded. Such “leishmania” forms multiply by binary division and mature into
infective blood forms. The cell eventually breaks open and the free parasites either
infect more vertebrate cells or are ingested by a “barbeiro.” In the insect’s diges-
tive tract they develop into critidia forms, which undergo successive binary divi-
sions. These mature into infective forms in the insect’s rectum. Modiªed from
Silva, L.H.P & Camargo, E.P. “Ciclo evolutivo do Trypanosoma cruzi.” In J.R.
Cançado, ed., Doença de Chagas. Belo Horizonte: Imprensa Oªcial do Estado de
Minas Gerais, 1968: 86–99.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
468
The Rise and Fall of Chagas Disease
The most obscure aspect of Chagas’ recognition remains the nomina-
tions he received for the Nobel Prize. Manoel A. Pirajá da Silva, a Brazil-
ian physician, was the ªrst to nominate him in 1913. Pirajá da Silva was
working in Europe when he was requested by the Nobel Committee to
nominate a candidate for the Prize. Hilário de Gouvêa, also a Brazilian
physician, made the second nomination, in 1921. Chagas never received
the Nobel Prize. In 1913, the Prize was conferred to Charles R. Richet for
his work on anaphylaxis. No one received the 1921 Prize.44
The invention of Chagas disease
In a period of less than ten months Chagas was introduced to a domiciliary
blood sucking hemipteran insect; he examined the contents of salivary
glands and guts; he found a trypanosome; he sent it to Manguinhos to in-
fect laboratory mammals; it turned out to be morphologically different
from T. minasense and pathogenic. Chagas searched for infected individuals
and found domestic animals and a sick child; ªnally, Chagas reported his
ªndings in local and international scientiªc journals.
There is no doubt that Chagas developed the human disease hypothesis
as soon as he came across the insect. This is not surprising: any good “par-
asite hunter” would be suspicious about the peculiar combination between
blood sucking insects and the health condition he encountered in
Lassance. It was natural for him to suppose that this insect might be a vec-
tor of some disease. Given the assumptions of the insect-vector theory, it
would probably be a protozoan or a helminth.
We can reconstruct the path taken by Chagas from the moment he met
the insect to the completion of his discovery as a sequence of adjusted hy-
potheses. His ªrst hypothesis comprised four components, which required
corresponding observations: (1) a vector, requiring the domiciliarity of the
insect; (2) an hematozoarian parasite, requiring vertebrate blood forms; (3)
man as the (or at least a) vertebrate host, requiring human blood forms;
and ªnally, (4) a disease, requiring symptoms.
COMPONENTS
REQUIREMENTS
1. A vector
2. An hematozoarian parasite
3. Man as the vertebrate host
4. A disease
Domiciliarity of the insect
Vertebrate blood forms
Human blood forms
Symptoms
44. See M. Coutinho (1999); M. Coutinho, O. Freire Jr. & J.C.P. Dias (1999).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
469
Each requirement was met in accordance with its difªculty. Evidence
for this hypothesis construction model abounds. The ªrst is his insistence
on the domiciliarity of the insect. Locals claimed that the barbeiro was
wild and came indoors just to feed. Today we know that they were
right. Yet, at that time, Chagas believed the insects were exclusively do-
miciliary.
The requirement of vertebrate blood forms was met through a routine
laboratory procedure, although time of residence in blood and patterns of
cell invasion were utterly unknown. Human blood forms were more
difªcult because they required an acute patient, which was rare. The worst
requirement was symptomatic consistency.
Given the ªrst component—the vector—Chagas proceeded to dissect
the insect. There he found the protozoa he was looking for. They had the
morphology of crithidia, which indicated they could either be natural par-
asites of the insect or intermediary forms of hemoºagellate—he opted for
the latter.45 The health condition of the locals made the insect-vector
model a strong bet. The updated hypothesis could be stated as: if the
crithidia are intermediate forms of a vertebrate hemoºagellate, then there should be
one or more vertebrate hosts (and a complex life cycle); one of the vertebrate hosts
might be the Callitrix and the hemoºagellate might be the T. minasense. The up-
dated hypothesis does not conºict with the early one: rather, it strength-
ens its agenda. The experimental infection was now required not only to
obtain blood forms and proceed through the early hypothesis, but also to
check the updated one. The experiments conªrmed the complex cycle in-
volving a vertebrate, revealed the difference between the candidate
trypanosomes, and gave indications as to an acute stage of the disease, in
which blood forms could be detected. He arrived at his ªnal hypothesis: if
the trypanosome is a parasite with a complex life cycle, an intermediate insect host,
and a vertebrate host (preferably human46), then it displays a cycle in the insect
and it should be transmitted through the sting, upon feeding; if it is transmitted
through the sting, then infective forms should be preferentially found in salivary
glands; if the parasite’s morphology and behavior bear similarities both with
hemosporidians and trypanosomes, then its blepharoplast is a nucleus and the para-
site can reproduce by schizogony; the disease caused by this insect should display an
45. The question of whether parasites of crithidia appearance observed in blood sucking
insects were developmental forms of complex cycle ºagellates (demanding a vertebrate host
as well) or natural parasites of the insect was an important one in those years. W. S. Patton
reviewed the literature on the current controversy concerning the possible relation between
insect intestinal crithidia and vertebrate hemoºagellates in Patton (1909).
46. In his ªrst paper, Chagas suggested that the development in humans and Callitrix
showed important life cycle differences in relation to other mammals. That should indicate
that man and the monkey were probably the natural hosts (Chagas 1909c).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
470
The Rise and Fall of Chagas Disease
acute form, relative to the bursts of ºagellates in the blood, and a chronic form, as-
sociated to the damage caused to the tissues.
At this point, Chagas’ observations and interpretations could be out-
lined as:
Observation
TANSITION
Interpretation
A. A prtozoan.
B. An insect host for
the parasite
(unproblematic)
(unproblematic)
C. A complex cycle
involving a vertebrate host
(problematic)
A parasite
A parasite cycle
A part of a complex
parasite cycle involving
another host
A disease
A human disease
Put together as a whole, the package constituted a novel and a highly
interesting, central, and prestigious object in the intellectual contexts of
the time.
Science and Medical learning for development
Chagas’ discovery provided reinforcements to others besides the insect-
vector model, or Prowazek and Hartmann. There was a political agenda
that received much support from the recognition of Chagas’ work. Chagas
believed that science was a crucial endeavor for Brazil. His understanding
of the role of science in the national culture and society was two-pronged:
on the one hand he argued that tropical medicine was a special enterprise
for Brazil and that substantial public effort should be allocated to its de-
velopment. He deªned tropical medicine in a broader way than European
pioneers at the beginning of the century, in that it comprised all those dis-
eases transmitted in an “indirect” manner, where the etiologic agent
spends part of its life outside the human host. Thus, he included more dis-
eases that affected the health of Brazilians in tropical medicine than the
earlier deªnition did. Eradication and prevention would be among the
most important tasks for development. From this perspective, tropical
medicine was both noble and patriotic (Chagas 1926).
On the other hand, Chagas understood that the microscope was medi-
cine’s basic tool. To prevent and eradicate, it was necessary to study and
identify. Germany and the United States were good examples. The tropi-
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
471
cal medicine arena promised Brazilian scientists vast possibilities and
prominent scientiªc deeds. Within the theoretical and methodological
frameworks offered by bacteriology, protozoology, and biology, among
others, Brazilian scientists should grasp the opportunities provided by
their “privileged” location with the country’s unique medical/scientiªc
objects. Chagas longed for this “nationalization of Brazilian medicine”
(Chagas 1928, pp. 184–5).
He warned his audience that although the preferential research objects
should be pathogenic organisms, scientists and doctors should be free to
carry out their sophisticated esoteric tasks:
Let no one argue, to exclude research from medical schools, that the
researcher frequently sidetracks towards the domains of pure sci-
ence, and that the evolution of medicine will proªt little from it. In
fact, I don’t know the limits between the pure and applied sciences.
Science is one only, and what today represents an abstract scientiªc
achievement, with no use, tomorrow will be an applied notion and,
sometimes, of the highest practical range.47
Tropical medicine thus had a double function: it was a militant ªght
against disease, to “improve the Brazilian race” and provide conditions for
development, and it was the “biological study of pathogenic parasites,” in-
separable from experimental medicine. Hygiene, sanitation, and high
quality (understood as international quality) medicine and science were
wrapped together.48
This was part of the “Manguinhos culture,” where the role of science
was heroic and concerned with national development. The sophisticated
basic research in the labs went hand-in-hand with the brave expeditions
47. “Nunca se allegue, para excluir a pesquiza do ensino medico, que não raro o pesquizador se
desvia para os dominios da sciencia pura, e pouco aproveitará, dahi por deante, á evolução da
medicina. Eu não sei, em verdade, onde os limites entre as sciencias puras e as de applicação. A sciencia
é uma unica, e o que hoje representa uma conquista scientiªca abstracta, sem qualquer fundo
utilitario, será amanhã uma noção applicada e, as vezes do mais alto alcance pratico” (Chagas
1928, p. 881).
48. He wrote: “The history of tropical disease is, primarily, the biological study of
pathogenic parasites. Those who study and practice medicine in warm countries cannot do
without the microscope because it is from its handling that result essential indications for
the purpose of our venture—that is, the treatment and prognostic of disease” (A historia da
doença tropical é, primacialmente, o estudo biologico dos parasitos pathogenicos. Do microscopio não
podem, agora prescindir os que estudam e praticam a medicina nos paizes quentes, porque é de seu
manejo que resultam indicações essenciaes á ªnalidade do nosso mistér, isto é, ao tratamento e ao
prognostico da doença). See Chagas (1926, p. 858).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
472
The Rise and Fall of Chagas Disease
that took Cruz’s small army to the most distant and poor areas of Brazil.
To “learn and cure” could have been their motto.49
Despite Chagas’ international recognition, few besides his close collab-
orators at Manguinhos shared his belief in the need to carry out high qual-
ity, international level, research. Few attributed a special role in develop-
ment to research.
In 1920, Chagas became the ªrst director of the National Department
of Public Health. He was named by President Epitácio Pessoa himself.
Chagas produced a deep public health reform for the country, centralizing
guidelines which should be based on solid knowledge. He was harshly
criticized for this plan, being frequently accused of surrendering to the
American model of public health (Chagas Filho 1993, p. 163, p. 171).
Like Cruz before him, Chagas faced reaction against vaccination and
against other urban modernization measures. He remained in the position
until 1926 (Chagas Filho 1993, pp. 168–9).
Forming the new generations of physicians and health professionals was
one of Chagas’ main concerns. He created the ªrst Special Hygiene and
Public Health course in Brazil in 1925. In 1926, the ªrst Tropical medi-
cine course started at the School of Medicine in Rio de Janeiro. He re-
ceived support from the Rockefeller Foundation, enabling many young
Brazilian sanitation professionals to study at Johns Hopkins University
School of Public Health. Chagas believed that medical students should be
exposed to research early in their academic lives and that the best brains
should be attracted to it. He harshly contested “backward” contenders
that defended a more academic learning in medical schools and claimed
that every advance observed in Brazil in his time could be accounted for
by the introduction of science and experimental medicine in Manguinhos.
The Serum Institute and the medical school should be one, together in the
heroic scientiªc adventure (Chagas 1928).
Fact or Artifact
Chagas’ academic boldness was not immune to the corrosive effects of con-
troversy. The celebrated scientiªc fact became vulnerable to the de-
constructive processes capable of bringing it back to a condition of doubt
and skepticism.
49. Answering requests from governmental or private corporations, Manguinhos sent
its teams of doctors and researchers to the inhospitable places where occupation was taking
place. The mode of transportation was frequently horseback. These expeditions had a pow-
erful political appeal, in a time when the Republic sought consolidation. Manguinhos’
doctors expressed a strong commitment towards the people and the nation. Accounts of
these expeditions can be found in Fonseca Filho (1974, pp. 18–19).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
473
There is evidence of some opposition to Chagas as early as 1910,
one year after his discovery. At this early stage, hostility apparently
emanated from the opening of the position of “head of service in
Manguinhos.” Rocha Lima, an important Brazilian researcher and head
of service in Manguinhos, left with Prowazeck to work at the Hamburg
Institute of Tropical Medicine. Oswaldo Cruz was upset with this.50
The position was ªlled through a meritocratic procedure that left no
doubt as to who would be the winner. Chagas’ contributions scored the
highest in the system established by Cruz to rank the candidates.51 Among
these candidates were Chagas’ close collaborators, such as Ezequiel Dias
and Henrique Aragão. Antagonism towards Chagas began to brood
there.52
The ªrst public contentions came from R. Kraus in the 1916 Pan-
American Medical Congress in Argentina. Kraus was an eminent German
microbiologist at Argentina’s Bacteriological
Institute. Chagas was
told that Kraus was going to contest his ªndings in the congress
and headed for Buenos Aires, where the two had an intense argu-
ment. Kraus found many infected triatomines in human dwellings in
certain regions of Argentina, but no cases of human infection. He
claimed that the parasite itself could be of small virulence and Chagas’
claims could be overestimated or ungrounded. Chagas answered that
the trypanosomes in that region were still not adapted to man.53 Most
accounts do not go over details about the Buenos Aires episode. In Cha-
gas Fo’s book about his father, the author states that Chagas was disturbed
by ªnding material from Manguinhos in Kraus’ laboratory. He was in-
50. A detailed analysis of this episode, along with the connections with Aragão and the
relationship between Afrânio Peixoto and R. Kraus can be found in J. L. Benchimol &
L. A. Teixeira (1993).
51. Published work that contained “important discoveries” or the introduction of new
methods were scored 7 to 9; theses, original or experimental contributions and studies in
systematics scored 4 to 6; ªnally, preliminary notes and simple descriptions scored 1 to 3.
Letter from Oswaldo Cruz, see “Um documento Histórico”(1979) and also Chagas Filho
(1993, pp. 94–96).
52. See Chagas Filho (1993, p. 96).
53. C. Chagas Filho (1974). Other Latin-American researchers disputed Chagas’ state-
ments as to many different issues at the time. One example is A. Reina Guerra, who, like
others, contested the etiologic role of T. cruzi in chronic cardiopathy, as stated by Chagas
(1916). See A. Reina Guerra (1939). It was only much later, by the late forties, that the
“Bambuí group,” led by Emmanuel Dias, could provide evidence for Chagas’ statements
about heart disease, and thus restore the legitimacy of his discovery discourse. They not
only showed Chagas’ early clinical interpretation to be correct about chronic cardiopathy,
but they also supported his claims as to “allergic” mechanisms that could sustain
inºammatory and other pathogenic processes in the chronic phase, in the presence of few
parasites. See Francisco S. Laranja, Emmanuel Dias, G.C. Nóbrega and A. Miranda (1956).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
474
The Rise and Fall of Chagas Disease
vited there by Kraus himself, but noticed the stamps from his institution
in several slides. He did not recall having received any request from
Kraus. It was clear that people from Manguinhos had been feeding Kraus’
arguments against Chagas (Chagas Filho 1993, p. 105).
When Chagas arrived from his trip to Buenos Aires, he found Oswaldo
Cruz’s health rapidly declining. He feared the consequences of Cruz’s
death to Manguinhos. Chagas’ children knew that their father was con-
scious of the opposition he faced at the institution. Cruz died in February
11, 1917 and Chagas was named director of the Institute three days later.
Figueiredo de Vasconcellos, who had been in charge of the Institute dur-
ing Cruz’s leave, became Chagas’ enemy forever. He had hoped to take
Cruz’ place. As soon as Chagas assumed the new position, he announced
his understanding of the experimental medicine mission of the institution
and his intention of emphasizing research activities. He sent researchers to
study abroad, especially in the United States (Chagas Filho 1993,
pp. 115–19).
Another important source of opposition was the prominent, although
controversial role Chagas was playing in Brazilian public health. When
Chagas was named director of the Department of Public Health in 1920,
Afrânio Peixoto, a powerful man in the Brazilian medical establishment,
was upset. He wanted the job and he did not share the meritocratic values
underlying Chagas’ recognition abroad. There is evidence that Peixoto had
great inºuence over the National Academy of Medicine (Chagas Filho
1993, pp. 188–9, p. 192).
The twenties were the period when Chagas consolidated his prestige in
European and American Institutions and, paradoxically, faced the worst
and most effective attacks from Brazilian physicians. In 1921 he received
an honorary doctorate from Harvard and in 1925 he became member of
the Hygiene Committee of the League of Nations.54 In Brazil, the chal-
lenges to Chagas’ discovery climaxed in the “Academy debate” that hap-
pened between 1922 and 1924, in which H.B. Aragão, Afrânio Peixoto,
and Figueiredo de Vasconcelos were important players. In November 30,
1922, Afrânio Peixoto spoke to the National Academy of Medicine at the
reception of Figueiredo de Vasconcellos, former Manguinhos researcher.
He said:
You could have found some mosquitoes, you could have invented a
rare and unknown disease, about which much was said, but whose
54. He was the ªrst Brazilian doctor honoris causa in Harvard. He was invited to many
other countries, such as Portugal, Spain, Germany, and Belgium, where he interacted with
medical researchers. He also visited Latin American medical institutions. About his travels
abroad in the twenties, see Chagas Filho (1993, pp. 122–27).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
475
victims almost no one knew, hidden in a countryside dwelling of
your province, a disease that you could magnanimously distribute
among your fellow countrymen, accused of being cretins.55
Chagas sent Miguel Couto, then president of the Academy, two letters
of protest, which were read at the December 14, 1922 session. He de-
manded the appointment of a commission of academics to judge his dis-
covery and he offered to resign from that Academy in case the commission
did not validate his claims. He demanded that the commission judge
whether the disease was a new morbid entity, with well deªned etio-
pathogeny, characteristic symptoms, and deªned clinical syndromes and
also judge his ethical procedure, the credits of his ªndings, and its scien-
tiªc and social relevance.56 This was a wide range of demands, resulting
from the fact that, during the challenge, all aspects of his discovery were
at stake, including his own participation. Kraus questioned the epidemio-
logical distribution of the disease and the virulence of the parasite. Peixoto
suggested that it was rare and unknown and its symptoms were question-
able. Opponents called it “the Lassance disease” instead of Chagas’ dis-
ease,57 thus discussing both Chagas’ claims about its wide distribution and
the authorship of the discovery. Figueiredo de Vasconcelos and Henrique
Aragão, both from the original Manguinhos team, claimed that the dis-
covery should be attributed to Oswaldo Cruz, not to Carlos Chagas
(Carneiro 1963, p. 65).
It was a strained and difªcult process. Almost one year later, Chagas
contested the approach adopted by the commission saying he wouldn’t ac-
cept a judgment that wasn’t based on a real epidemiological assessment
made through local examination—he wanted the commission members to
take a journey through the country. The commission threatened to resign
(Carneiro 1963). Another participant, O. da Fonseca Filho gave his ac-
count of the discussion that took place in the Academy between Novem-
ber 8 and December 6, 1923: Afrânio Peixoto abandoned the site and left
Figueiredo de Vasconcelos and Parreiras Horta to defend him against
Clementino Fraga, who represented Chagas. Fraga presented accounts
55. Peixoto was using irony, a privileged weapon for this physician. He was praising
Vasconcellos for not having done as Chagas. Peixoto was a powerful man in medical insti-
tutions, both in Rio and in Bahia, where he came from. He was also comfortable among
the local elite. Afrânio Peixoto 1922, in Fonseca Filho (1974, p. 65). See also Chagas Filho
(1993, p. 225).
56. See Carneiro (1963, pp. 64–75).
57. See the account given by Carneiro (1963, pp. 64–75), about the debate to which he
attended as member of the Academy and follower of Chagas’ contenders. The expression
“Chagas disease” was coined years before by the president of the National Academy of
Medicine, Miguel Couto.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
476
The Rise and Fall of Chagas Disease
given by other doctors and researchers concerning the extent of the distri-
bution of human infection by the parasite and that matter was decided in
Chagas’ favor.58 In the November 16 session, Bento Cruz, Oswaldo Cruz’s
son, argued in favor of Chagas priority in the discovery.59 Finally, on De-
cember 6, 1923, the conºict seemed to be over. However, at least up to the
middle thirties, the disease was ignored in medical curricula and hospital
diagnosis as well.60 It took time and effort to restore the legitimacy of
Chagas disease.61
The majority of the participants in the Academy debate did not share
Chagas’ afªliation to international scientiªc communities. They ignored
the disciplinary context that rendered Chagas’ protozoological ªndings so
relevant. Since all the aspects of his discovery were neatly bound together,
the legitimacy of his protozoological assertions was checked by epidemio-
logical and clinical arguments.
Chagas’ familiarity with the international scientiªc styles of his time
was not enough to protect his statements. His recognition by the corre-
spondent communities was equally insufªcient. The correctness of his hy-
potheses and his errors had little to do with the de-constructive process.
Discovery construction is complex and social to a large extent. However, it
cannot be reduced to institutional sanctioning: Chagas achieved a formal
victory and a functional defeat. Although the commission’s conclusions fa-
vored him, the disease lost its capacity to mobilize scientiªc production. It
only became undisputed and was studied again after Chagas’ death.
Concluding remarks
This is a story about obvious scientiªc success and also about defeat. On
the one hand, no one would dispute Chagas’ success in the early days of
the discovery: he was rapidly recognized and received all the accolades a
58. Fonseca Filho (1974, pp. 64–66). Clementino Fraga’s account was very detailed and
especially careful, scientiªcally updated and precise in the protozoology section. Fraga’s
letters containing Olympio da Fonseca’s and Magarino Torre’s ªndings and opinions are re-
produced in Chagas Filho (1993, pp. 205–215).
59. See Chagas Filho (1993), reproduced in pages 199–200.
60. See E. Villela (1930). The positions of Chagas’ enemies (like Afrânio Peixoto) as
professors at the medical schools of the time, with recognized leadership in faculty envi-
ronments can largely explain the exclusion of the disease as a study topic.
61. There are reasons to believe that the anti-Chagas group might be responsible for
Chagas’ failure to be awarded the Nobel Prize. Other early century tropical disease dis-
coverers were awarded the Prize: Ronald Ross in 1902 and Charles Louis Alphonse Laveran
in 1907. Four out of six of Chagas’ contenders in the Schaudinn Prize competition were
awarded the Noble Prize as well: Laveran, in 1907; Paul Ehrlich and Elie Metchnikoff, in
1908; and Charles Jules Henri Nicolle, in 1928. Chagas seems to have been in the “Nobel
track.” In Brazil, however, The Nobel Commission inquiries met an atmosphere of skepti-
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
477
good scientist might desire. On the other hand, by now, no one would
doubt that the de-construction was extremely effective. It was a scientiªc
defeat, since there was very little advancement of knowledge about any as-
pect of Chagas disease until his death in 1934. It was also a public health
disaster, since the disease was not studied, students were not trained to di-
agnose it and sanitation measures for its prevention were not undertaken.
Considering the recent success of various prevention campaigns using
simple methods, it is reasonable to assume that millions of Latin Ameri-
cans died prematurely as a consequence of the de-construction of Chagas
disease.62
To understand such a paradoxical chapter of the history of science, we
might proªt from a drama metaphor. In the Chagas disease play, there is
something weird with the sequence from the ªrst to the second act. The
characters are different, the setting is differently arranged and the effects
are not the same. They are so different that they cannot be acts of the same
performance. We realize that we are, in fact, watching different plays.
In the ªrst play, Chagas was the hero. The supporting actors were the
good guys, sharing with him meritocratic values, modernizing perspec-
tives, and an understanding of the international nature of science and its
role in development. Facing local health problems with this perspective
was a priority. These values comprised the prevailing version of national-
ism in the ªrst play.63 Cruz, Chagas’ enthusiastic protector, was alive and
strong, enjoying the climax of his political prestige in the Federal Govern-
ment. The central object, Trypanosoma cruzi, was reasonably well behaved
community praised
in the
parasitological tropical medicine above all and was clamorous and sup-
portive with the new discovery.
international medical
laboratory. The
When Cruz died, the second play took the stage. An incomplete troupe
kept on the old performance, but with no success on Brazilian ground. In
the second play, nationalism assumed different colors: any modernizing
cism surrounding the disease. Research on this matter is in progress. See M. Coutinho
(1999a); M. Coutinho, O. Freire Jr. & J.C.P. Dias (1999); Nobel Foundation Web Site
(2000). About the restoration of Chagas disease’s legitimacy, see M. Coutinho (1999b).
62. The South Cone Initiative of the WHO, involving Argentina, Brazil, Chile, Para-
guay and Uruguay, is one such case. The infection reduction in Brazil and Uruguay in the
period from 1985–1996 for the age group of 0–14 years is 96%. For all the countries in
the program, the reduction has been of 83%. See World Health Organization (2000).
63. Other examples of a nationalistic motivation for the study of local health problems
are the Andean biology tradition in Peru initiated in the 1930’s, studied by M. Cueto, the
Escola Tropicalista Bahiana of the 1860’s-1890’s in Brazil, studied by J. Peard, and the lep-
rosy control in Colombia in the 1920’s, studied by D. Obregón. In the ªrst two cases, pio-
neers confronted the still prevalent beliefs about tropical degeneration and inferiority with
science. See M. Cueto, (1989b); J. Peard (1996, 1997); D. Obregón (1996).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
478
The Rise and Fall of Chagas Disease
initiative was seen with suspicion. Revealing to the world a consumptive
disease such as the American Trypanosomiasis was considered anti-patri-
otic.64 The supporting actors had no idea what science was all about and
could not care less about Chagas’ international prestige. However, we
must never forget that they were the ones in charge, in spite of Chagas’ ad-
ministrative positions and in spite of his formal victory in the Academy.
They opposed and sabotaged Chagas in every instance;65 they denied
better salaries and full time employment for his researchers,66 which grad-
ually led to Manguinhos’ decline; they controlled medical education in
Brazil and prevented the students from learning about Chagas’ disease.
The parasite, well behaved in the laboratory, proved to be a very difªcult
pathogen to study. It was not easily detectable in the bloodstream in the
chronic stage of the disease and there was no deªnite diagnostic procedure
to detect the acute cases, where the parasites could be found. T. cruzi re-
mained elusive for years. Across the ocean, tropical medicine had changed
and was no longer oriented to parasites and vectors.
The change of tide simply destroyed the whole ediªce of scientiªc ex-
cellence that Cruz and Chagas had erected. To explain why this scientiªc
enterprise in particular and many others in Latin America suffer from such
instability, we must understand the interplay of factors determining the
fate of scientiªc initiatives in each case. H. Vessuri’s account of the devel-
opment of science in Argentina shows it to be punctuated by promising
initiatives and their rapid failure. The early development of plant genet-
ics, abruptly aborted when the pioneers were forced to emigrate in 1947;
the attempts to stimulate the study of physics, astronomy, mathematics,
and chemistry in the 1930s and 1940s by Enrique Gaviola, which met an
“unresponsive, short-sighted milieu”; the electronic components research
halted by the military coup of 1966, among others, are sad examples of
this trend. Vessuri points out that talented Argentine scientists faced un-
favorable socio-political conditions as soon as they were seen as a threat to
the status quo—whatever that was at the moment.67
64. Afrânio was the champion of this nationalistic discourse. He claimed that Chagas
had made his reputation over the tragedy of Brazilian country folk who suffered from goi-
ter and idiocy. See Carneiro (1963, pp. 70–75); Pedro de Toledo claimed that Chagas jeop-
ardized Brazil’s chances of competing with other nations for the immigrants that were
pouring out of Europe. Parreiras Horta suggested that Chagas had broadcast to the world
an image of Brazil as a country of weak and sickly people, incapable of productive work.
Chagas Filho (1993, pp. 203–3).
65. About the political difªculties faced by Chagas in the government, see Chagas
Filho (1993, p. 142).
66. See Chagas Filho (1993, p. 173).
67. See Vessuri (1996a).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
479
The conºuence of independent interests involved in granting support
and recognition for the activities undertaken by Manguinhos (Brazilian
authorities’, the medical community’s, the international tropical medicine
community’s, etc.) help to account for the early recognition that Chagas
received. Nevertheless, their very independence may also account for the
later de-construction. As soon as the contingently favorable factors were
gone, traditional interests and petty politics took over and quenched the
embryonic scientiªc enterprise.
To understand the interplay of factors we must consider both the local
and the wider international contexts for science. The discovery of Chagas
disease and the subsequent research it engendered cannot be described
solely in terms of the local demands and health conditions. Manguinhos
was meeting the political interests of important local social segments with
sanitation initiatives much like those found all over
the world.
Manguinhos’ scientists were enjoying support for their scientiªc endeav-
ors in the country because of the products they rendered in sanitation and
hygiene at the local level. However, although “science,” broadly under-
stood as an enterprise that produced useful knowledge, was incorporated
as something vaguely valuable, Brazilian scientists never succeeded in
convincing society that their activity was socially relevant. The idea that a
space for science was unsatisfactorily established in Brazil has been explored
by Schwartzman (1991). In other countries, such as Argentina, political
instability and government brutality against the scientiªc community
have been major explanations for scientiªc failure (Vessuri 1996a). The
abortion of promising scientiªc initiatives in Latin America, however,
cannot be blamed on military coups per se. A public consensus about the
role of scientiªc investigation beyond immediate practical results has
never been achieved. This has been exempliªed by Vessuri, in Argentine
physics, astronomy, mathematics, and chemistry in the 1930’s and 1940’s
(Vessuri 1996a). The pitfalls of consensus building with respect to the role
of science are not exclusively the responsibility of the traditional elites, ei-
ther. T. Glick discussed the consequences of leftist dependentista theories
when, in the 1970’s their advocates took over Venezuela’s science and
technology agency, the CONICIT. Believing that “imported” science “was
a means of cultural domination,” they questioned the utility of basic sci-
ence. As a consequence, there was a divorce between basic and applied sci-
entists, which hampered research development.68 This condition of dis-
agreement differed from that enjoyed by the European scientists, who
worked in countries where science was a traditionally established enter-
prise.
68. See Glick (1984).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
480
The Rise and Fall of Chagas Disease
Chagas’ discovery cannot be described as a simple application or mim-
icry of European tropical medicine either. When Chagas met the blood-
sucking insect in Lassance, he did not come to the human disease hypo-
thesis by simple substitutions on the malaria puzzle, as Stepan claims
(Stepan 1976, pp. 118–20). The analogy with malaria appears as a
secondary addition to Chagas’ early model. It was inserted there to provide
support for M. Hartmann’s theory. This is when the Schaudinn school co-
mes in, and it stops there. Accordingly, Chagas was not yet committed to
the Schaudinn school of protozoology in 1907, when he ªrst went to
Lassance, as Perleth’s explanation would require.69 Chagas generated his
human disease hypothesis because he was a legitimate practitioner of trop-
ical medicine and, as such, he shared the community’s emphasis on the in-
sect-vector theory, with all its examples. He mobilized the concepts he
was familiar with as soon as he met the barbeiro and, in his own words, he
invented a disease (Chagas 1928). After that, back in Rio de Janeiro, he
proªted much from his interaction with the German researchers. They
helped with the interpretation of cytological experiments and he followed
their theoretical perspective. The binucleata model was never pursued in
Trypanosomiasis research again. Finally, Delaporte’s claims about the anal-
ogy with sleeping sickness to explain Chagas’ early model of the disease
are not supported by the historical evidence.
The establishment of a stable scientiªc tradition from a successful epi-
sode, its strengthening and diversiªcation, the extension of its relations to
other social actors, and the reproduction of its patterns have never taken
place in Brazil. The country had a scattering of successful episodes, but
their effects on the scientiªc establishment dwindled quickly. In this re-
spect, other Latin American countries are similar, as seen. They lacked the
institutional and political conditions to support the internationalization
sought by isolated groups of scientists.70
International factors played a role in the success of Chagas’ discovery,
and also in its subsequent decline. The same can be said about local fac-
tors. This is certainly true about any scientiªc endeavor. What is relevant
here is the independence of the factors and the resulting isolation of Cha-
gas and his institution. Internationalization might not be the key to suc-
cess, but isolation seems to be a certain road to ruin.
69. In order for the discovery to be a “reºection of the Schaudinn school of
protozoology,” Chagas would have to be committed to it before he elaborated his hypothe-
sis. Therefore, before he went to Lassance. See M. Perleth (1997, p. 92).
70. In his history of Brazilian science, S. Schwartzman (1991) details the rise and de-
cline of each successful initiative. About other Latin American countries and Latin Amer-
ica in general, see Vessuri (1991, 1996b). See also the “success stories” reported by T. F.
Glick (1994), and Cueto (1989a).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
481
References
Aragão, H. B. 1907. “Sobre o cyclo evolutivo do halterídio do pombo.”
Brazil Medico 21: 141–142, 301–303.
Arnold, D. 1988. “Introduction: disease, medicine and empire.” In D. Ar-
nold, Imperial medicine and indigenous societies. Manchester University
Press.
Basalla, G. 1967. “The Spread of Western Science.” Science 156: 611–
622.
Benchimol, J. L. & L.A. Teixeira 1993. Cobras, lagartos e outros bichos: uma
história comparada dos Institutos Oswaldo Cruz e Butantan. Rio de Janeiro:
Editora UFRJ.
Benchimol, J. L. (ed.) 1990. Manguinhos; do sonho à vida—A ciência na Belle
Époque. Rio de Janeiro: Casa de Oswaldo Cruz..
Brener, Z. 1992. In S. Wendel, Z. Brener, M.E. Camargo, A. Rassi (Eds.),
Chagas Disease—American Trypanosomiasis: its impact on transfusion and
clinical medicine.(ISBT BRAZIL’92, SAO PAULO, BRAZIL). http://
www.dbbm.ªocruz.br/tropical/chagas/chapter3.html.
Canizares Esguerra, J. 1999. “Nation and Nature: Creole Patriotic Repre-
sentations of Nature in Colonial Spanish America.” International Semi-
nar on the History of the Atlantic World, 1500–1800. Charles Warren
Center for Studies in American History, Harvard University. Working
Paper 98–31.
———. “Spanish America: From Baroque to Modern Colonial Science.”
To appear in the Eighteenth Century volume of the Cambridge History of Sci-
ence. Roy Porter, volume ed., Ronald Numbers and David Lindberg,
general eds. Cambridge University Press.
Carneiro, M. 1963. História da Doença de Chagas. Curitiba.
Chagas, C. 1905. Prophylaxia do impaludismo. Rio de Janeiro, Instituto de
Manguinhos.
———. 1906/7 “Prophylaxia do impaludismo.” Brazil Médico 20: 315–
317; 337–340; 419–422; 21: 151–154.
———. 1907a. “Adenda: Lassance,” 1907, Carlos Chagas. In Joaquim
Romeu Cançado and Moisés Chuster, eds., Cardiopatia Chagásica. Belo
Horizonte: Fundação Carlos Chagas, 1985: 391–413.
———. 1907b. Novas espécies de culicideos brazileiros. Rio de Janeiro:
Instituto de Manguinhos.
———. 1907c. “O novo genero Myzorhynchella de Theobald. Duas novas
anophelinas brazileiras pertencentes a este genero.” Brazil Medico 21:
291–293; 303–305.
———. 1907d. “Uma especie do genero Taeniorhynchus.” Brazil Medico
21: 313–314.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
482
The Rise and Fall of Chagas Disease
———. 1908a. “Beitrag zur Malariaprophylaxis.” Z. Hyg. Infektkr 60:
321–334.
———. 1908b. “Trypanosoma minasense.” Brazil Medico 22: 471.
———.
“Neue Trypanosomen.” Archiv
für
Schiffs-und
1909a.
Tropenhygiene 13: 120.
———. 1909b. “Nova especie morbida do homem, produzida por um
trypanozoma (trypanozoma Cruzi).” Brazil Médico 16.
———. 1909c.
“Nova
tripanozomiase humana. Estudos
a
morfologia e o ciclo evolutivo do Schizotrypanum cruzi, n. gen., n. s, ajente
etiolojico de nova entidade morbida do homem.” Memórias do Instituto
Oswaldo Cruz 1: 1–62.
sobre
———. 1910. “Nova entidade morbida do homem.” Brazil Médico, 43.
———. 1911. “Sobre as variações cíclicas do cariozoma em duas especies
de ciliados parazitos. Contribuição para o estudo do nucleo nos
infuzorios / Über die zyklischen Variationen des Caryosoms bei zwei
zum Studium des
Arten
Infusorienkernes.” Memorias do Instituto Oswaldo Cruz 3: 136–144.
parasitischer
Ciliaten.
Beitrag
———. 1913. “Revisão do cyclo evolutivo do ‘Trypanozoma cruzi.”
Brazil Medico, June 15, 23.
———. 1916. “Pathogenic processes of American Trypanosomiasis.”
Memórias do Instituto Oswaldo Cruz 8: 3–38.
———. 1922. “Descoberta do Trypanosoma cruzi e veriªcação da
Tripanozomiase Americana. Retrospecto Histórico.” Memórias do
Instituto Oswaldo Cruz 15: 67–76.
———. 1926. “Aula inaugural da Cadeira de Medicina Tropical—14 de
Setembro de 1926.” In A. Prata (ed.) Carlos Chagas—Coletânea de
Trabalhos Cientíªcos. Brasília: Editora Universidade de Brasília, 1981:
831–860.
———. 1928. “Lição de abertura dos cursos da Faculdade de Medicina do
Rio de Janeiro—1928.” In A. Prata (ed.) Carlos Chagas—Coletânea de
Trabalhos Cientíªcos. Brasília: Editora Universidade de Brasília, 1981:
861–883.
Chagas Filho, C. 1974. “Histórico sobre a Doença de Chagas,” In J.R.
Cançado, ed., Doença de Chagas. Belo Horizonte: Imprensa Oªcial: 5–
21.
———. 1993. Meu Pai. Rio de Janeiro: Casa de Oswaldo Cruz/
FIOCRUZ.
Chalhoub, S. 1993. “The Politics of Disease Control: Yellow Fever and
Race in Nineteenth Century Rio de Janeiro.” Journal Latin American
Studies 25: 441–463.
Coutinho, M. 1999a. “O Nobel perdido.” Folha de São Paulo, February 7,
caderno 5: 11.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
483
———. 1999b. “Ninety Years of Chagas Disease: A Success Story At The
Periphery.” Social Studies of Science 29: 519–549.
Coutinho, M., O. Freire Jr. & J.C.P. Dias 1999. “The Nobel Enigma:
Carlos Chagas’ nominations for the Nobel Prize.” Memórias do Instituto
Oswaldo Cruz 94: 123–129.
Cueto, M. 1989a. Excelencia Cientiªca en la Periferia. Lima: Grade/
Concytec.
———. 1989b. “Andean Biology in Peru.” Isis 80: 640–658.
Curtin, D. 1989. Death by Migration. Cambridge University Press.
Delaporte, F. 1994/95. “Chagas, a lógica e a descoberta.” História, Ciências,
Saúde—Manguinhos 1: 39–53.
Desowitz, R.S. 1993. The Malaria Capers. New York: W.W. Norton &
Co.
Dias, E. 1944. Doença de Chagas; noções Rio de Janeiro: Ministério da
Educação e Saúde, Serviço Nacional de Educação Sanitária.
Dias, J.C.P. 1995. “Entrevista com João Carlos Pinto Dias.” The Oral His-
tory Program of the Núcleo de Pesquisas sobre Ensino Superior -Universidade de
São Paulo. Belo Horizonte, MG, Brazil, April 1995.
Farley, J. 1991. Bilharzia; A History of Imperial Tropical Medicine. Cam-
bridge University Press.
Fonseca Filho, O. 1974. A Escola de Manguinhos—Contribuição para o estudo
do desenvolvimento da medicina experimental no Brazil. São Paulo: EGRT.
Glick, T. 1984. “Science and Society in 20th-century Latin America.”
Cambridge History of Latin America, vol. VI, Part I: 463–535.
———. 1994. “The Rockefeller Foundation and the Emergence of Genet-
ics in Brazil.” In M. Cueto, ed., Missionaries of Science. Bloomington: In-
diana University Press: 149–164.
Harden, V.A. 1985. “Rocky Mountain Spotted Fever Research and the
Development of the Insect Vector Theory, 1900–1930.” Bulletin of the
History of Medicine 59: 449–466.
Hartmann, M. & C. Schilling 1917. Die Pathogenen Protozoen. Berlin.
Hartmann, M. & S. von Prowazek 1907. “Blepharoplast, Caryosom und
Centrosom. Ein Beitrag zur Lehre von der Doppelkernigkeit der Zelle.”
Archiv für Protistenkunde 10: 306–335.
Hartmann, M. & C. Chagas 1910. Estudos sobre ºajelados. Rio de Janeiro:
Leuzinger.
Hartmann, M. 1907.
“Das System der Protozoen.” Archiv
für
Protistenkunde 10: 139–158.
Hegner, R.W. & W.H. Taliaferro 1925. Human Protozoology. New
York.
Kean, B.H. 1977. “Carlos Chagas and Chagas Disease.” The American Jour-
nal of Tropical Medicine and Hygiene 26: 1084–87.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
484
The Rise and Fall of Chagas Disease
Laranja, F.S., E. Dias, G.C. Nóbrega and A. Miranda 1956. “Chagas’ dis-
ease. A clinical, epidemiological and pathologic study.” Circulation 14:
1035–1060.
Laveran, A. & F. Mesnil 1904. Trypanosomes et Trypanosomiases. Paris:
Masson et Cie.
Lent, H. & P. Wygodzinsky 1979. “Revision of
the Triatominae
(Hemiptera, Reduviidae) and their signiªcance as vectors of Chagas
disease.” Bulletin of the American Museum of Natural History 163: 123–
520.
Lewinsohn, R. 1979. “Carlos Chagas (1879–1934): The discovery of
Trypanosoma cruzi and of American Trypanosomiasis.” Transactions of the
Royal Society of Tropical Medicine and Hygiene 74: 513–23.
Lewinson, R. 1981. “Carlos Chagas and the discovery of Chagas’ disease
(American Trypanosomiasis).” Journal of the Royal Society of Medicine 74:
451–55.
Löwy, I. 1990. “Yellow Fever in Rio de Janeiro and the Pasteur Institute
Mission (1901–1905): the Transfer of Science to the Periphery.” Medical
History 34: 144–163.
Mac Leod, R. 1988. “Introduction.” In R. Mac Leod & M. Lewis, eds.,
Disease, Medicine and Empire. London: Routledge: 1–18.
Nobel Foundation Web Site, http://www.nobel.se, last accessed in January
20, 2000.
Obregón, D. 1996. “The Social Construction of Leprosy in Colombia,
1884–1939.” Science, Technology and Society 1: 1–23.
Patton, W.S. 1909. “The life cycle of a species of Crithidia parasitic in the
s.” Archiv für
tracts of Tabanus hilarius and Tabanus
intestinal
Protistenkunde 15: 333–362.
Peard, J.G. 1996. “Tropical Medicine in Nineteenth-Century Brazil: The
Case of the ‘Escola Tropicalista Bahiana’, 1860–1890.” In David Ar-
nold, ed., Warm Climates and Western Medicine. Amsterdam: Rodopi:
108–132.
———. 1997. “Tropical disorders and the forging of a Brazilian medical
identity, 1860–1890.” Hispanic American Historical Review 77: 1–44.
Perleth, M. 1997. Historical Aspects of American Trypanosomiasis (Chagas
Disease). Frankfurt am Main: Peter Lang.
Prowazek, S. 1905. “Studien über säugetiertrypanosomen.” Arbeiten Der
Kaiserlichen. Geseundheitsamt 22.
Reina Guerra, A. 1939. Contribución al estudio de la tripanosomiais en El Sal-
vador. San Salvador, PhD thesis.
Schwartzman, S. 1991. A Space for Science. University Park, Pennsylvania:
The Pennsylvania University Press.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Perspectives on Science
485
Stepan, N. 1976. Beginnings of Brazilian Science: Oswaldo Cruz, Medical Re-
search and Policy 1890–1920. New York: Science History Publications.
Um documento Histórico 1979. Ciência e Cultura 31: 10, suplemento.
Vessuri, H. 1991. “Universalismo y nacionalismo en la ciencia moderna.
Una aproximación desde el caso venezolano.” Quipu 8: 255–271.
———. 1996a. “La ciencia académica en América Latina en el siglo XX.”
In J.J. Saldaña, ed., Historia Social de las Ciencias en América Latina. Mex-
ico City: UNAM: 437–479.
———. 1996b. “Bitter Harvest. The Growth of a Scientiªc Community
in Argentina.” In J.Gaillard, V.V.Krishna and R.Waast, Eds., Scientiªc
Communities in the Developing World. Part 3: Scientiªc Communities in
Latin America. New Delhi: Sage Publications: 307–335.
Vianna, G.O. 1911. “Contribuição para o estudo da anatomia patolojica da
‘Moléstia de Carlos Chagas’ (Esquizotripanose humana ou tireoidite
parasitária).” Memórias do Instituto Oswaldo Cruz 3: 276–294.
Villela, E. 1930. “A ocurrencia da molestia de Chagas nos hospitaes de
Bello Horizonte e na população de seus arredores.” Annaes da Faculdade
de Medicina da Universidade de Minas Geraes 1: 1–18.
Worboys, M. 1976. “The Emergence of Tropical Medicine: a Study in the
Establishment of a Scientiªc Specialty.” In G. Lemaine et al., eds., Per-
spectives in the Emergence of Scientiªc Disciplines. Paris: Mouton: 73–96.
———. 1983 “The Emergence and Early Development of Parasitology.”
In K.S. Warren & J.Z. Bowers, eds., Parasitology—A Global Perspective.
New York: Springer-Verlag: 1–18.
———. 1993. “Tropical Diseases.” In W.F. Bynum & R. Porter, eds.,Com-
panion Encyclopaedia of the History of Medicine. London: Routledge: 512–
536.
———. 1994. “The Comparative History of Sleeping Sickness in East
and Central Africa, 1900–1914.” History of Science 32: 89–102.
World Health Organization—Division of Control of Tropical Diseases
“Chagas Disease Elimination.” See http://www.who.ch/ctd/. Last ac-
cessed January 20, 2000.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
e
d
u
p
o
s
c
/
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
/
7
4
4
4
7
1
7
9
0
4
7
0
p
o
s
c
.
1
9
9
9
7
4
4
4
7
p
d
.
.
.
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3