The Review of Economics and Statistics
VOL. CIV
JANUARY 2022
NUMBER 1
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
N. Meltem Daysal, Marianne Simonsen, Mircea Trandafir, and Sanni Breining*
Abstract—We investigate the effects of early-life medical treatments on
the treated children and their families. We use a regression discontinuity
design that exploits changes in medical treatments across the very low
birth weight (VLBW) cutoff. Using administrative data from Denmark, we
establish that VLBW children have better health and higher test scores. We
find that these benefits spill over to other family members: mothers enjoy
better mental health, and siblings have higher test scores. Maternal mental
health improvements seem to be driven by better focal child health and
sibling spillovers by improved interactions within the family and parental
compensating behavior.
I.
Introduction
AN extensive body of research in economics suggests
that early-life conditions have long-lasting impacts on
individual well-being, including health, educational attain-
ment, and labor market outcomes (Almond & Currie, 2011;
Almond, Currie, & Duque, 2018). Growing evidence also in-
dicates that disabled children affect the socioeconomic out-
comes of other family members, such as parental labor supply
(Gunnsteinsson & Steingrimsdottir, 2019; Deshpande, 2016;
Powers, 2003), health (Burton, Lethbridge, & Phipps, 2008),
and marital stability (Kvist, Nielsen, & Simonsen, 2013) and
sibling academic achievement (Black et al., 2017). A natural
question then is whether, and by how much, interventions
that improve child health also affect these spillovers in the
family. In this paper, we address this question by investigat-
ing the spillover effects of early-life medical treatments on
the socioeconomic outcomes of other family members, fo-
cusing on the specific case of treatments provided to very
low birth weight (VLBW) children—those with birth weight
below 1,500 grams.
Received for publication May 15, 2019. Revision accepted for publication
June 3, 2020. Editor: Brian A. Jacob.
∗Daysal: University of Copenhagen, CEBI, and IZA; Simonsen: Aarhus
University and IZA; Trandafir: University of Southern Denmark and IZA;
Breining: Ramboll Management Consulting.
Doug Almond, Prashant Bharadwaj, Aimee Chin, Gordon Dahl, Nabanita
Datta Gupta, Joe Doyle, Mark Duggan, Bill Evans, David Figlio, Kristiina
Huttunen, Katrine Løken, Bhash Mazumder, and seminar participants at
Bergen, Concordia, Gothenburg, Houston, IZA, Mainz, Michigan, Tilburg,
VIVE, York, Zurich, Second SDU Workshop on Applied Microeconomics,
SFI-Lund Workshop on Health Economics, Essen Health Conference, and
Copenhagen Education Network provided helpful comments and discus-
sions. The activities of CEBI are financed by the Danish National Research
Foundation, grant DNRF134. S.B. and M.S. gratefully acknowledge finan-
cial support from CIRRAU. The authors bear sole responsibility for the
content of this paper.
A supplemental appendix is available online at https://doi.org/10.1162/
rest_a_00982.
Medical interventions targeting VLBW children constitute
an ideal setting to study spillover effects for several reasons.
First, they have been found to substantially improve the health
(Cutler & Meara, 1998; Almond et al., 2010; Bharadwaj,
Løken, & Neilson, 2013) as well as the academic achievement
(Bharadwaj et al., 2013) of treated children. Second, although
VLBW children represent a small share of all births, they
account for a substantial portion of newborn health care ex-
penditures. For example, VLBW babies in the United States
represent around 1.5% of all births, but the neonatal intensive
care unit costs associated with these babies alone account for
30% of all newborn health care costs (Johnson et al., 2013).
Finally, focusing on treatments provided to VLBW children
allows us to overcome identification challenges arising from
potentially correlated unobservables within the family, such
as shared genetic factors that affect both the receipt of medi-
cal treatments by targeted children and the outcomes of other
family members. Specifically, we use a regression discontinu-
ity design that exploits changes in medical treatments across
the very low birth weight threshold to address the nonran-
dom assignment of medical treatments (Almond et al., 2010;
Bharadwaj et al., 2013). We restrict our analysis to the fami-
lies of focal children (defined as the children with birth weight
in a small window around 1,500 grams) with gestational age
above 32 weeks because the medical guidelines prescribe ad-
ditional medical treatments to children with gestational age
below 32 weeks regardless of their birth weight.
Using population-level data from Denmark, we first repli-
cate the finding in the previous literature that VLBW children
are significantly less likely to die within the first year of life
relative to newborns with slightly higher birth weight. We
also confirm the finding that these children have higher math
and language test scores in ninth grade. Our estimates are re-
markably comparable in magnitude to the reductions in infant
mortality and improvements in test scores from the previous
studies using data from the United States, Chile, and Norway
(Almond et al., 2010; Bharadwaj et al., 2013). We add to these
studies by expanding the outcome set to include a range of
common childhood disabilities (intellectual disability, atten-
tion deficit hyperactivity disorder, behavioral and emotional
disorders, cerebral palsy, and epilepsy), as well as by inves-
tigating effects on hospital and emergency room (ER) visits
up to fifteen years after birth. Our findings suggest that chil-
dren slightly below the 1,500 gram threshold have the same
The Review of Economics and Statistics, January 2022, 104(1): 1–16
© 2020 The President and Fellows of Harvard College and the Massachusetts Institute of Technology
https://doi.org/10.1162/rest_a_00982
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
–
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
2
THE REVIEW OF ECONOMICS AND STATISTICS
likelihood of a childhood disability by age 10 as compared to
children slightly above the threshold. While there is no im-
pact on child disability, the medical treatments provided to
VLBW children seem to result in better health during school
years as proxied by reduced hospital and ER contacts.
We next turn to investigating the spillover effects of early-
life medical treatments on other family members. We exam-
ine the effects on siblings’ health (hospital and ER contacts)
and academic achievement (ninth-grade math and language
test scores, enrollment beyond compulsory education). For
parents, we focus on labor market outcomes (employment
status, number of days worked), annual gross income, and
mental health as proxied by antidepressant use. Where possi-
ble, we present the short-term effects (one to five years after
the birth of the focal child) separately from the long-term
effects (six to fifteen years after the birth of the focal child).
We try to address the potential multiple inference issues re-
sulting from the large number of outcomes we study in two
ways. First, we create indices summarizing the relevant vari-
ables in each outcome domain and time horizon, standard-
ized at the level of the birth cohort of the focal child. Second,
we adjust the p-values to take into account the multiple in-
ference problem using a procedure proposed by Anderson
(2008).
Our results suggest that early-life medical interventions
have no impact on parental behavior that affects total house-
hold resources: we do not observe discontinuous changes
across the VLBW cutoff in parental labor force participation
or income in either the short run or the long run. This is per-
haps not surprising given that Denmark has one of the most
generous social safety nets in the world, including 52 weeks
of parental leave, generous cash payments to families with
children, heavily subsidized child care, and free and universal
health care. Our results instead suggest that early-life med-
ical interventions may improve intrahousehold interactions.
In particular, we find that the mothers of VLBW focal chil-
dren are significantly less likely to use antidepressants soon
after the focal child is born and that these mental health gains
diminish as the focal child ages. We provide evidence sug-
gesting that both focal child survival and improved focal child
health are important drivers of these mental health gains.
Our results also suggest that early-life medical treatments
have substantial positive spillovers on sibling test scores.
We find that the siblings of VLBW newborns have ninth-
grade test scores that are on average 0.375 standard devia-
tion higher. Our results further highlight that test score gains
are observed across skill domains: language and math test
scores are higher by 0.386 and 0.255 standard deviations, re-
spectively. These results are economically large, correspond-
ing to a reduction of 33% to 69% in the test score gap be-
tween the children in the top and bottom 10% of the income
distribution. We show that these sibling spillovers are un-
likely to be driven by correlated health shocks within the
family that would result in siblings’ exposure to early-life
medical treatments themselves or by differential focal child
survival at the cutoff. Instead, our evidence points to im-
proved intrafamily interactions as a potential channel behind
the sibling spillovers.
Finally, we provide indirect evidence on the role of parental
reallocation of resources within the family. If the production
of human capital exhibits dynamic complementarities, then
parental investments have higher returns for children with
high initial endowment than for children with low initial en-
dowment. If parents engage in compensating behavior, our re-
sults suggest that the siblings of VLBW focal children should
receive more parental resources than the siblings of focal chil-
dren with birth weight slightly above 1,500 grams. We find
that the siblings of VLBW focal children experience higher
test score gains if they have high initial endowments them-
selves (as proxied by their birth weight), a pattern consistent
with compensating behavior by their parents, especially in
the presence of dynamic complementarities in human capital
accumulation.
Our paper makes three contributions. First, we add to the
studies that document spillover effects of child health. The
majority of this research examines the effects of having a
disabled child on parental outcomes, such as labor supply
(Gunnsteinsson & Steingrimsdottir, 2019; Deshpande, 2016;
Powers, 2003) and health (Burton et al., 2008). One notable
exception is Black et al. (2017), who investigate spillovers to
siblings and find that the second child in a family has worse
test scores when the third child is disabled.1 Our paper doc-
uments that improvements in child health that do not operate
through child disability status may still result in significant
sibling spillovers.
Second, we contribute to the economic literature on the
returns to early-life medical interventions. These studies al-
most exclusively investigate the effects on treated children
(Cutler & Meara, 1998; Chay, Guryan, & Mazumder, 2009;
Field, Robles, & Torero, 2009; Almond et al., 2010; Bharad-
waj et al., 2013; Daysal, Trandafir, & van Ewijk 2015, 2019;
Hjort, Sølvsten, & Wüst, 2017; Bütikofer, Løken, & Kjell Sal-
vanes, 2019).2 The main insight that emerges from our work
is that medical treatments may have far-reaching effects on
family well-being through spillovers even in developed coun-
tries with generous welfare systems.
Third, our results speak to the economic literature that re-
lies on sibling fixed-effects models to account for unobserved
heterogeneity across households in estimating the effects of
various exposures. To the extent that siblings have spillovers
1There is also evidence on sibling spillovers more generally. For example,
Dahl, Løken, and Mogstad (2014) show that take-up of family-friendly poli-
cies affects siblings’ subsequent use of these policies, Joensen and Nielsen
(2018) and Nicoletti and Rabe (2019) find that siblings’ education choices
and test scores causally affect younger siblings’ academic outcomes, and
Altonji, Cattan, and Ware (2017) and Heissel (forthcoming) document
that older siblings’ risky behavior have an impact on younger siblings’
outcomes.
2One exception is Adhvaryu and Nyshadham (2016), who examine the
effects of a large-scale iodine supplementation program in Tanzania on
parents’ investments in children and find that the siblings of treated children
were more likely to be immunized.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
–
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
3
on each other, sibling fixed-effects models would not estimate
the true treatment effects.
Our results are also pertinent to the ongoing discussions
about the cost effectiveness of early-life medical treatments.
During the past few decades, medical spending for the very
young increased substantially faster than spending for the
average individual. For example, US annual spending on in-
dividuals aged 1 to 64 increased by 4.7% between 1960 and
1990, while per capita spending on infants under 1 year old
increased by 9.8% per year (Cutler & Meara, 1998). Techno-
logical innovations are widely considered the main driver of
this medical cost growth in general and in the specific case
of early-life treatments (Newhouse, 1992; Cutler & Meara,
1998). As medical expenditures keep increasing, understand-
ing the benefits of early-life medical interventions becomes
even more important. Our finding that medical treatments for
VLBW children have positive externalities on other family
members indicates that conventional calculations understate
the net benefits of these treatments.
II.
Institutional Background
The majority of Danish health care services, including
birth-related procedures, are free of charge, and all residents
have equal access (Danish Ministry of Health and Preven-
tion, 2008). The first European neonatal intensive care unit
was established in 1965 at Rigshospitalet in Denmark, and
the use of early-life medical technologies has since followed
the international development (Mathiasen et al., 2008). Dan-
ish neonatal medicine textbooks pay particular attention to
VLBW children (those weighing less than 1,500 grams, re-
gardless of gestational age) and very premature newborns
(those with a gestational age less than 32 weeks, regard-
less of birth weight). These birth weight and gestational age
classifications are frequently found in medical research pa-
pers based on Danish data where the focus is often on their
higher mortality rates (Thomsen et al., 1991; Hertz, Holm, &
Haahr, 1994). Medical handbooks suggest courses of treat-
ment based on either birth weight or gestational age (Schiøtz
& Skovby, 2001). Specific recommendations in terms of nu-
trition and vitamin supplements exist for VLBW children
(Peitersen & Arrøe, 1991). In addition, papers indicate that
children below 1,500 grams or born before 32 weeks of ges-
tation are more likely to receive additional treatments such as
cranial ultrasound (Greisen et al., 1986), antibiotics (Topp,
Uldall, & Greisen, 2001), prophylactic treatment with nasal
continuous positive airway pressure, prophylactic surfactant
treatment and high priority of breast feeding, and use of the
kangaroo method (Jacobsen et al., 1993; Verder et al., 1994;
Verder, 2007; Mathiasen et al., 2008).
Anecdotal evidence from hospital and regional specific
notes also outline special services that are provided to fami-
lies with children below 1,500 grams or below 32 weeks of
gestational age. These services include referrals to a physio-
therapist who guides and instructs parents on how to stimulate
the development of the child and on various baby exercises.
It is also mentioned that all children below 1,500 grams or
below 32 weeks of gestational age are routinely checked one
to two months after discharge and again when they are 5
months, 1 year, and 2 years old.3
III. Empirical Strategy
Identification of the (spillover) effects of early-life health
interventions is complicated by the nonrandom assignment
of medical treatments. In particular, there may be unobserved
determinants of the outcomes of other family members that
are correlated with the receipt of medical treatments by tar-
geted children, such as shared genetic factors. In order to
address this endogeneity, we follow Almond et al. (2010)
and Bharadwaj et al. (2013) and use a regression discontinu-
ity design that exploits changes in medical treatments across
the VLBW threshold. Specifically, we estimate
(cid:3)
(cid:2)
yi jt = f
bw j − 1500
+ βVLBWj + δXi jt + (cid:2)i jt ,
(1)
where yi jt is an outcome of family member i of focal child j at
time t after the birth of the focal child, bw j is the birth weight
of focal child j, f (·) is a first-degree polynomial in distance
to the VLBW cutoff that is allowed to differ on both sides
of the cutoff, VLBWj is an indicator for focal child j having
very low birth weight (bw j < 1500), and Xi jt is a vector of
covariates.4
We start our analysis by replicating and extending the
findings in the previous literature on the impact of medical
technologies on focal children themselves: we set i = j in
equation (1). We then turn to effects on other family mem-
bers. The parameter of interest, β, is an intention-to-treat esti-
mate of the effects that additional medical treatments received
by VLBW newborns may have on themselves and on their
families.
Our baseline regressions use a triangular kernel that assigns
decreasing weights to observations further away from the cut-
off. We choose our bandwidth based on a rule-of-thumb pro-
cedure suggested by Calonico, Cattaneo, and Titiunik (2014),
which yields optimal bandwidths between 118 grams and 251
grams with an average of 189 grams (see appendix table A2).
We choose 200 grams as our preferred bandwidth to ensure
that newborns on either side of the VLBW cutoff are nearly
identical. This bandwidth is the same as the one used by
Bharadwaj et al. (2013) for Norwegian data and reflects the
relatively small number of observations available in Denmark
and Norway. The vector of covariates, Xi jt , includes indica-
tors for heaping at multiples of 50 grams in all specifications
unless mentioned otherwise (Barreca et al., 2011).5 Some
3Unfortunately, our data do not include any information on specific early-
life treatments.
4An alternative strategy would rely on the 32-week cutoff for gestational
age. This strategy is infeasible with our data because gestational age is
recorded in full weeks.
5Given that birth weight is measured in grams, heaping is generally sym-
metric around our cutoff point, and hence our strategy is less likely to be
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
4
THE REVIEW OF ECONOMICS AND STATISTICS
of our robustness checks additionally control for child and
family characteristics (see section IV).
We are interested in exploring a variety of outcomes across
multiple domains for several family members. This gives rise
to a multiple inference problem: we may estimate statistically
significant effects of the VLBW status on some outcomes
simply by chance. We address this issue in two ways fol-
lowing the recommendations of Anderson (2008). First, we
create indices for each family member and each domain (see
section IV and appendix table A1 for details). While this pro-
cedure helps with reducing the dimensionality, we are still
left with a relatively large number of indices. Hence, as a
second step, we adjust the p-values to take into account the
multiple inference problem based on a procedure proposed
by Anderson (2008).6
Finally, we construct robust confidence intervals follow-
ing Calonico et al. (2014, 2019). These confidence intervals
are centered on bias-corrected estimates instead of the usual
(conventional) estimates and use the standard errors from a
specification with a higher-order polynomial in the running
variable, which in our case is a second-degree polynomial.
Therefore, in addition to the coefficient estimates and their
robust standard errors, we also report the bias-corrected es-
timates that are used to construct these robust confidence
intervals.
IV. Data
Our key data set is the Birth Register, which includes in-
formation about the universe of births in Denmark starting
from 1970. For each child, the data include information on
the exact date of birth, gender, and plurality. Birth weight is
recorded in 250 gram intervals between 1973 and 1978, in
10 gram intervals in the period 1979 and 1990, and at the
gram level since 1991. Gestational age was added beginning
in 1982. Using parental identifiers, we are able to link chil-
dren to their parents and siblings and determine parity. We
also link these data to other register data that provide infor-
mation on both parents and children regarding demographic
characteristics, labor market outcomes, health outcomes, and
academic achievement.
We first use data on focal children to investigate whether
early-life medical interventions have an impact on focal child
health and academic achievement. Our mortality index in-
cludes two previously studied short-term outcomes, 28-day
and 1-year mortality. In addition, we construct two health in-
dices. Our short-term health index uses indicators for being
hospitalized during each year between the ages of 1 and 5,
affected by the criticism raised by Barreca et al. (2011). Indeed, we show
in section VC that our results are robust to the exclusion of these controls.
6The false discovery rate (FDR) is the average fraction of true null hy-
potheses among the rejected hypotheses, and the q-value is the level of the
FDR desired by the researcher (Benjamini & Hochberg, 1995; Benjamini,
Krieger, & Yekutieli, 2006). We report the lowest q-value, that is, the lowest
sharpened FDR, at which an estimated effect is still significant (see Ander-
son, 2008, for details). This is conceptually similar to a p-value in that it
represents the probability of a type 1 error.
while our long-term health index uses separate indicators for
being hospitalized and for having an ER visit during each year
between the ages of 6 and 15. Given the previous medical lit-
erature linking very low birth weight to child developmental
disabilities (Schieve et al., 2016), we also construct a disabil-
ity index based on separate indicators for being diagnosed by
age 10 with one of the following conditions: intellectual dis-
ability, attention deficit hyperactivity disorder, behavioral and
emotional disorders, cerebral palsy, and epilepsy. Our first
measure of human capital accumulation is a test score index
based on course-specific test scores from ninth-grade qual-
ifying exams in reading and math, available between 2001
and 2010.7 Finally, we create an index of enrollment beyond
compulsory education (nine years during our sample period)
using indicators for enrollment in high school or vocational
school at age 18, enrollment in an academic track at age 18,
enrollment in higher education at age 24, and enrollment in
a university at age 24.
We then turn to spillover effects on the family. The out-
comes for siblings mirror the outcomes for focal children
with the exception of mortality and disability diagnosis. In
particular, we create a short-term health index using indica-
tors for being hospitalized during each year when the focal
child is 1 to 5 years old and a long-term health index using
indicators for being hospitalized or having an ER visit dur-
ing each year when the focal child is 6 to 15 years old. We
construct a test-score index based on ninth-grade math and
language test scores and an index of enrollment beyond com-
pulsory education based on siblings’ enrollment in (higher)
education at ages 18 and 24.
For parents, we focus on mental health and labor market
outcomes separately for mothers and fathers. Our two men-
tal health indices are based on indicators for having filled at
least one antidepressant prescription during each year when
the focal child is 2 to 5 and 6 to 15 years old.8 For labor mar-
ket outcomes, we study effects on employment and income.
We create two employment indices for each parent based on
the number of days worked, as well as indicators for being
employed in each calendar year when the focal child is 1 to
5 and 6 to 15 years old. We similarly create income indices
based on the log real annual gross income over the same range
of focal child age.
We construct each index in two steps. We first standardize
each variable by the birth cohort of the focal child such that it
has a mean of 0 and a standard deviation of 1. Next, we take
the average of the standardized variables that make up the
index, and because some of these variables are correlated,
we restandardize the index at the level of the birth cohort
of the focal child. Appendix table A1 lists each variable in-
cluded in the construction of each index. We provide results
7All exams are graded by the teacher and by an external examiner, who
can overrule the teacher.
8The prescription drug register begins recording data from 1995 so we
can construct measures of antidepressant use only starting from focal child
at age 2.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
5
using selected outcomes or alternative aggregation strategies
in appendix tables A6 to A8.
Some of our checks use focal child characteristics (gesta-
tional age, indicators for gender, parity, plurality, birth year,
and birth region), maternal characteristics at the birth of the
focal child (age, years of education, indicators for marital
status and immigrant status), and sibling characteristics (ges-
tational age, birth weight, and indicators for gender, parity,
plurality, and birth year).9
We define the analysis sample in several steps (see ap-
pendix table A3). First, we select focal children born between
1982 and 1993.10 We then exclude observations for which
either birth weight or gestational age is missing and restrict
the sample to those with birth weight within 1,300 to 1,700
grams. Given that we are particularly interested in sibling
spillovers, we further restrict the sample to the 3,677 focal
children with siblings.11 As discussed in section II, newborns
with a gestational age of less than 32 weeks are always cov-
ered by medical guidelines for receiving additional medical
interventions, regardless of their VLBW classification. Since
there is no discontinuity in eligibility for medical treatments
(Bharadwaj et al., 2013), we do not expect to observe a dis-
continuity in focal child outcomes or the outcomes of their
family members. Therefore, we use the 1,521 focal children
with gestational age below 32 weeks and their families only
in a falsification check, and from here on, we focus exclu-
sively on the 2,156 focal children with gestational age of at
least 32 weeks (hereafter the FC sample) and their families.
Parents are identified from the birth register. Our data in-
clude parental identifiers for all the mothers. If the mother is
married to a man at the time of birth, authorities automatically
register the husband as the biological father. When the mother
is unmarried, the biological father needs to claim paternity of
the child. Parental identifiers for the fathers are missing for
only forty of the focal children in the FC sample. Thus, the
parent sample virtually overlaps with the FC sample.
Siblings are defined as children born to the same mother
from different pregnancies. We include both older and
younger siblings because the receipt of additional medical
treatments around the VLBW cutoff does not seem to have
an impact on future fertility decisions.12 We focus on sib-
9Maternal education is missing for 315 observations corresponding to 154
mothers. We replace these with the median number of years of education by
birth cohort and include an indicator for imputed maternal education. Our
results (available on request) are robust to excluding these observations or
the indicator for missing mother’s education.
10Our sample includes focal children born after 1982, when both birth
weight and gestational age are recorded. We include cohorts born before
1994 for two reasons. First, this allows us to study human capital accumu-
lation information for all cohorts, which makes it possible to compare the
effects of early-life health interventions on the focal children in our context
to those in previous studies. Second, evidence suggests that medical guide-
lines around the VLBW cutoff are less likely to be binding in recent years
(see, for example, note 20 in Bharadwaj et al., 2013).
11The results for the sample, including the 922 focal children who have no
siblings born within our sample period, are quantitatively and qualitatively
similar (available on request).
12A focal child may have more than one sibling. We treat each sibling-
focal child pair as an independent observation. This is not a concern for
lings who are old enough for us to observe their academic
outcomes. Tests are administered when children are around
15 to 16 years old, so data on test scores are available for
cohorts of siblings born between 1986 and 1997. Enrollment
outcomes are measured at ages 18 and 24 and include siblings
born between 1970 and 1993. The resulting sample includes
3,311 siblings of focal children with gestational age of at least
32 weeks (the sibling sample).13
V. Results
A. Tests of the Validity of the Regression
Discontinuity Design
The validity of an RD design rests on the assumption that
individuals do not have precise control over the assignment
variable. Since women cannot precisely predict the birth
weight of their children, the variation in birth weight near
the VLBW cutoff is plausibly as good as random (Almond
et al., 2010; Bharadwaj et al., 2013). The key identification
assumption of the RD design could be violated if physicians
systematically misreport birth weight, especially in the pres-
ence of financial incentives for manipulation (Shigeoka &
Fushimi, 2014; Jürges & Köberlein, 2015).
In order to test this assumption, we examine the frequency
of births by birth weight within our bandwidth around the
cutoff. Appendix figure A1 plots the distribution of observa-
tions in the FC/parent sample and in the sibling sample by
birth weight of the focal child. We use 10 gram bins because
birth weight is reported in 10 gram intervals for most of our
sample period.14 Similar to previous studies (Almond et al.,
2010; Bharadwaj et al., 2013), we observe reporting heaps
at multiples of 50 and 100 grams but there is no evidence of
irregular heaping around the VLBW cutoff. We check this
more formally by estimating a local-linear regression similar
to our baseline model, using the number of births in each birth
our identification because parity and total family size are relatively smooth
across the cutoff in the FC sample. In addition, we find no evidence of a
discontinuity at the cutoff when we examine the probability of having a
younger sibling, the number of younger siblings, and the birth spacing be-
tween focal children and younger siblings (see table 1). Finally, our results
are qualitatively similar when we cluster the standard errors at the mother
level in order to correct for the bias in standard errors caused by the poten-
tial correlation in the error terms between pairs of siblings from the same
household (available on request).
13Test scores are missing for approximately 20% of the eligible cohorts in
the sibling sample. This is because children can be exempted from taking
the test if, for example, they have a documented disability. This could be
a concern if medical treatments provided to focal children have an impact
on the test taking of siblings. We find no discontinuity at the cutoff in
the probability that a sibling takes the language test (estimate 0.029, bias-
corrected estimate [b.c.e.] 0.051, s.e. 0.070, mean 0.808) or the math test
(estimate 0.048, b.c.e. 0.069, s.e. 0.068, mean 0.804), or in the age when
they take the test (estimate −0.139, b.c.e. −0.106, s.e. 0.120, mean 16.035).
Enrollment information is available for all eligible cohorts.
14Some degree of rounded running variables is common across studies
relying on regression discontinuity designs; a prominent example is to use
age in quarters (Card, Dobkin, & Maestas, 2008) or years (Oreopoulos,
2006). While rounding can, of course, cause discretization bias (Dong,
2015), we believe this is a minor issue in our case with access to relatively
fine-grained data.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
6
THE REVIEW OF ECONOMICS AND STATISTICS
TABLE 1.—DISTRIBUTION OF COVARIATES ACROSS THE VLBW CUTOFF
A. Focal child characteristics (N = 2,156)
Boy
Birth order
Multiple birth
Gestational age
Family size
Has younger siblings
Number of younger siblings
B. Sibling characteristics (N = 3,311)
Estimate
(1)
−0.028
0.229
0.065
−0.353**
0.054
−0.066
−0.189
Boy
Birth order
Multiple birth
Gestational age
Birth weight
VLBW
Age difference–older sibling
Age difference–younger sibling
C. Mother’s characteristics at the birth of the focal child (N = 2,156)
−0.003
−0.115
0.026
−0.319
−128.494*
0.012
−0.119
−0.400
Age
Education (years)
Immigrant
Married
D. Father’s characteristics at the birth of the focal child (N = 2,116)
1.118
−0.246
−0.021**
0.047
Age
Education (years)
Immigrant
Not reported
2.044**
0.172
0.013
−0.008
Bias-Corrected
Estimate
(2)
Robust
Standard Error
(3)
Sharpened
q-Value
(4)
Mean of Dependent
Variable
(5)
[−0.079]
[0.166]
[0.092]
[−0.508]
[0.009]
[−0.020]
[−0.205]
[−0.033]
[−0.154]
[0.011]
[−0.464]
[−188.938]
[0.019]
[−0.397]
[−0.691]
[1.040]
[0.218]
[−0.052]
[0.003]
[2.132]
[0.465]
[−0.006]
[−0.004]
(0.077)
(0.173)
(0.070)
(0.258)
(0.160)
(0.078)
(0.133)
(0.068)
(0.147)
(0.017)
(0.449)
(105.751)
(0.033)
(0.782)
(0.449)
(0.800)
(0.389)
(0.027)
(0.080)
(0.873)
(0.400)
(0.039)
(0.023)
{0.919}
{0.919}
{0.851}
{0.576}
{1.000}
{1.000}
{0.713}
{1.000}
{0.919}
{1.000}
{0.919}
{0.618}
{1.000}
{1.000}
{0.713}
{0.851}
{1.000}
{0.576}
{1.000}
{0.507}
{0.919}
{1.000}
{1.000}
0.456
1.911
0.208
34.097
2.937
0.611
0.899
0.520
2.121
0.023
38.209
2,898.7
0.046
6.586
4.515
27.735
11.239
0.068
0.535
30.547
11.608
0.074
0.021
Sample of (family members of) focal children with birth weight within a 200 g bandwidth around the 1,500 g cutoff and gestational age of at least 32 weeks. Column 1 reports the estimated coefficient of the VLBW
variable from a separate local-linear regression with a triangular kernel of the characteristic listed in the row for the family member indicated in the panel heading. Column 2 reports the corresponding bias-corrected
estimate, column 3 the robust standard error (Calonico et al., 2014, 2019), column 4 the sharpened q-value for the set of tests included in the table (Anderson, 2008), and column 5 the mean of the variable in the row
calculated among (family members of) focal children with birth weight above 1,500 g. Asterisks indicate statistical significance (significant at **5% and *10%), based on robust confidence intervals centered on the
bias-corrected estimates (for details, see Calonico et al., 2014, 2019).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
weight bin as the dependent variable (McCrary, 2008). We do
not find any evidence of a discontinuity in the frequency of
births at the VLBW cutoff.15 These results suggest that birth
weight is unlikely to be manipulated in our context.
In the remainder of this section, we check if there are differ-
ences in observable characteristics across the VLBW cutoff
by estimating our baseline model with the covariates as de-
pendent variables. If the RD design is valid, then there should
be no discontinuities at the VLBW cutoff.16 Table 1 provides
the results. Panels A, C, and D use the FC/parent sample and
check whether focal child and parental characteristics are
balanced, while panel B uses the sibling sample to check for
discontinuities in the covariates of siblings. Column 1 pro-
vides the conventional point estimate from the local-linear
regression, and columns 2 and 3 present the bias-corrected
15The estimates corresponding to appendix figures A1a and A1b are 0.092
(b.c.e. −7.507, standard error s.e. 6.955) and 0.196 (b.c.e. −12.614, s.e.
17.429). The results are qualitatively similar when using the logarithm of
the number of births as the dependent variable instead. In this case, the
estimated coefficients are 0.013 (b.c.e. −0.223, s.e. 0.188) and 0.027 (b.c.e.
−0.238, s.e. 0.324).
16Visual evidence on selected covariates is provided in appendix figures
A2 to A4.
estimate and the robust standard error (Calonico et al., 2019).
We report sharpened q-values, that is, p-values based on the
numbers in columns 2 and 3 further corrected for multiple
inference and in column 4 (see section III and Anderson,
2008, for details). Finally, column 5 reports the mean of the
covariate in the sample of (family members of) focal chil-
dren with birth weight of at least 1,500 g. The results show
that observations just below the VLBW cutoff are generally
similar to those just above the VLBW cutoff. There are few
characteristics with marginally significant discontinuities at
the threshold, and none of these survive the adjustment for
multiple inference: the lowest q-value is 0.5.
Overall, the analyses in this section indicate no evidence
of manipulation of the running variable around the VLBW
cutoff or of discontinuities in the observable characteristics
of focal children, their parents, and their siblings.
B. Baseline Results
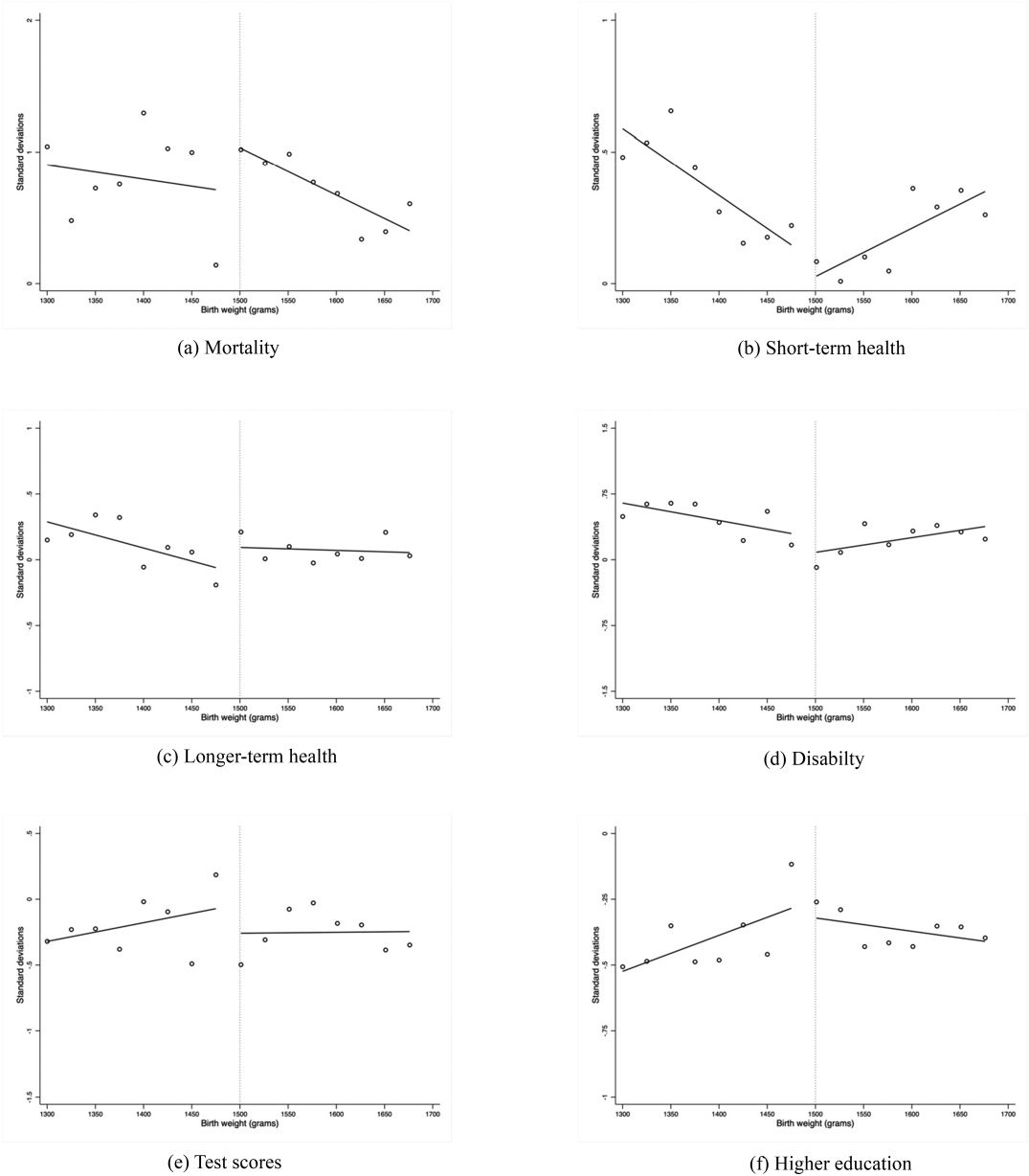
Figure 1 provides visual evidence on the relationship be-
tween birth weight and the outcomes of focal children. Fig-
ures 1a to 1d focus on child health, while figures 1e to 1f focus
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
7
FIGURE 1.—EVOLUTION OF SUMMARY INDICES OF FOCAL CHILDREN AROUND THE VLBW CUTOFF
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Sample of focal children with gestational age of at least 32 weeks. Each dot represents the average of the summary index indicated in the panel for a 40 g bin. Focal children with birth weight of 1,500 g are excluded.
The lines plot a first-degree polynomial estimated separately on either side of the VLBW cutoff.
8
THE REVIEW OF ECONOMICS AND STATISTICS
TABLE 2.—SHORT-TERM EFFECTS OF VLBW CLASSIFICATION
TABLE 3.—LONG-TERM EFFECTS OF VLBW CLASSIFICATION
Mother
(3)
—
Father
(4)
—
Health
Mean outcome
Observations
Focal Child
(1)
Siblings
(2)
Mother
(3)
Father
(4)
−0.324***
[−0.437]
(0.144)
{0.052}
0.039
1,960
0.090
[0.167]
(0.155)
{0.332}
0.115
3,311
−0.168
0.233
[−0.199]
[0.427]
(0.293)
(0.122)
{0.239}
{0.293}
−0.011 −0.026
2,116
2,155
Focal Child
(1)
Siblings
(2)
—
−0.508**
[−1.011]
(0.408)
{0.065}
0.726
2,156
0.133
[0.161]
(0.190)
{0.415}
0.190
1,978
−0.049
[−0.041]
(0.142)
{0.471}
0.103
3,311
−0.347*** −0.016
[−0.338]
[0.098]
(0.173)
(0.124)
{0.415}
{0.052}
0.023
0.042
669
689
—
—
0.068
0.066
Mortality
Mean outcome
Observations
Health
Mean outcome
Observations
Labor market
outcomes
Mean outcome
Observations
[0.211]
(0.150)
{0.293}
−0.060
2,143
0.109*
[0.286]
(0.153)
{0.213}
−0.070
2,144
[0.205]
(0.156)
{0.303}
0.051
2,099
0.112*
[0.289]
(0.171)
{0.239}
−0.048
2,100
Income
—
—
Mean outcome
Observations
Sample of (family members of) focal children with birth weight within a 200 g bandwidth around the
1,500 g cutoff and gestational age of at least 32 weeks. Each cell reports the estimated coefficient of
the VLBW variable from a separate local-linear regression with a triangular kernel of the summary index
listed in the row for the family member indicated in the column (see appendix table A1 for details on
the construction of the summary indices). All regressions control for heaping at multiples of 50 g. Bias-
corrected estimates are listed in brackets, robust standard errors in parentheses, and sharpened q-values
in braces below the coefficient estimates. The mean of the outcome is reported for (family members of)
focal children with birth weight above 1,500 g. Asterisks indicate statistical significance (significant at
***1%, **5%, and *10%) based on robust confidence intervals centered on the bias-corrected estimates
(for details, see Calonico et al., 2014, 2019).
on academic achievement. The figure shows that focal chil-
dren with birth weight slightly lower than 1,500 grams have
lower mortality than children who weigh slightly more than
1,500 grams. Conditional on survival, however, the short-
term health of children seems to be similar across the VLBW
cutoff. We also do not observe any discontinuity in the dis-
ability index in figure 1d, but there is some indication of
improved long-term health during primary school–age years
from the index based on hospital admissions and ER vis-
its in figure 1c. Turning to academic achievement, figure 1e
shows that focal children with birth weight slightly lower than
1,500 grams have visibly higher test scores in ninth grade. The
improved test scores, however, do not seem to result in higher
enrollment beyond compulsory education (figure 1f).
Column 1 in tables 2 and 3 presents the corresponding
regression results from our baseline model. Each cell re-
ports the estimated coefficient of the VLBW variable from
a separate local-linear regression with a triangular kernel of
the summary index. Bias-corrected estimates are listed in
brackets, robust standard errors in parentheses, and sharpened
q-values in braces. We also report the mean of the outcome for
observations above the cutoff. Consistent with the graphical
evidence, we find that VLBW newborns have lower mortality
in the short run and lower hospital and ER visits in the long
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Disability diagnosis by
0.234
—
—
—
age 10
Mean outcome
Observations
Ninth-grade test scores
Mean outcome
Observations
Higher education
Mean outcome
Observations
[0.246]
(0.294)
{0.415}
0.249
2,156
0.314**
[0.564]
(0.234)
{0.065}
−0.257
952
0.044
[0.146]
(0.180)
{0.415}
−0.380
2,156
0.375***
[0.524]
(0.193)
{0.052}
−0.216
1,539
0.048
[0.086]
(0.141)
{0.415}
−0.211
2,759
Labor market outcomes
—
—
Mean outcome
Observations
Income
Mean outcome
Observations
See the notes to table 2.
—
—
—
—
—
—
0.093
[0.098]
(0.153)
{0.415}
−0.028
2,124
0.080*
[0.252]
(0.152)
{0.239}
0.037
2,074
0.095
0.076
[0.214]
[0.171]
(0.149)
(0.139)
{0.332}
{0.293}
−0.063 −0.068
2,074
2,125
run: mortality is 0.508 standard deviation lower (table 2), and
hospitalizations and ER visits during school years are 0.324
standard deviation lower (table 3).17 We also find that focal
children just below the VLBW cutoff have on average 0.314
standard deviation higher test scores in the ninth grade, but
they are not significantly more likely to be enrolled beyond
compulsory education.
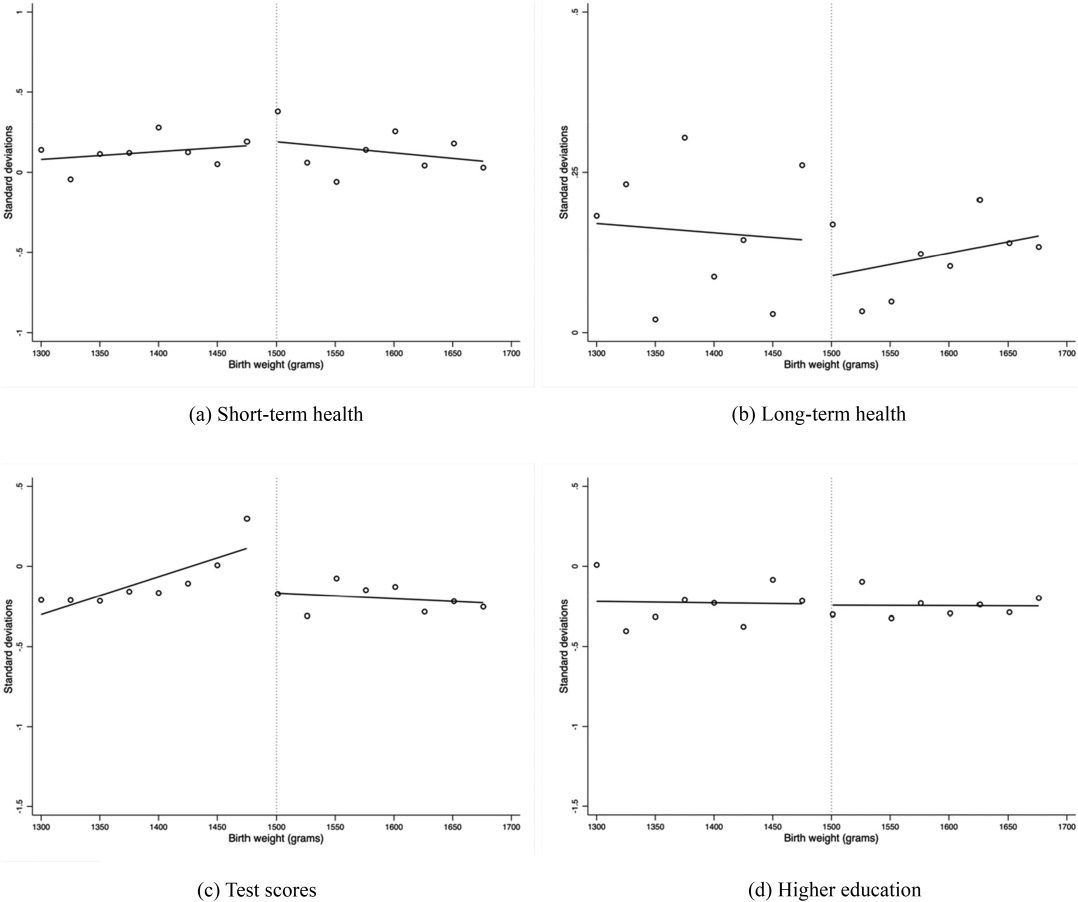
We next turn to spillover effects on the siblings. Figure 2
provides visual evidence while the corresponding regression
results are presented in column 2 of tables 2 and 3. Figure 2
shows that the siblings of focal children with birth weight
slightly lower than 1,500 grams have visibly higher test scores
in ninth grade. On the other hand, there is no evidence of
important spillovers on health or enrollment outcomes. The
regression results confirm that the early-life medical treat-
ments offered to VLBW children have significant positive
17As an example, the 95% robust confidence interval for the mortality
effect (−0.508) is constructed using the bias-corrected estimate and the
robust standard error as: −1.011 ± 0.408 × 1.96 = [−1.811, −0.211].
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
9
FIGURE 2.—EVOLUTION OF SUMMARY INDICES OF SIBLINGS AROUND THE VLBW CUTOFF, GA32+ SAMPLE
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Sample of siblings of focal children with gestational age of at least 32 weeks. Each dot represents the average of the summary index indicated in the panel for a 40 g bin. Siblings of focal children with birth weight of
1,500 g are excluded. The lines plot a first-degree polynomial estimated separately on either side of the VLBW cutoff.
spillovers on the test scores of the siblings without gains in
higher education or health outcomes. In particular, we find
that siblings of VLBW newborns have ninth grade test scores
that are on average 0.375 standard deviation higher.18
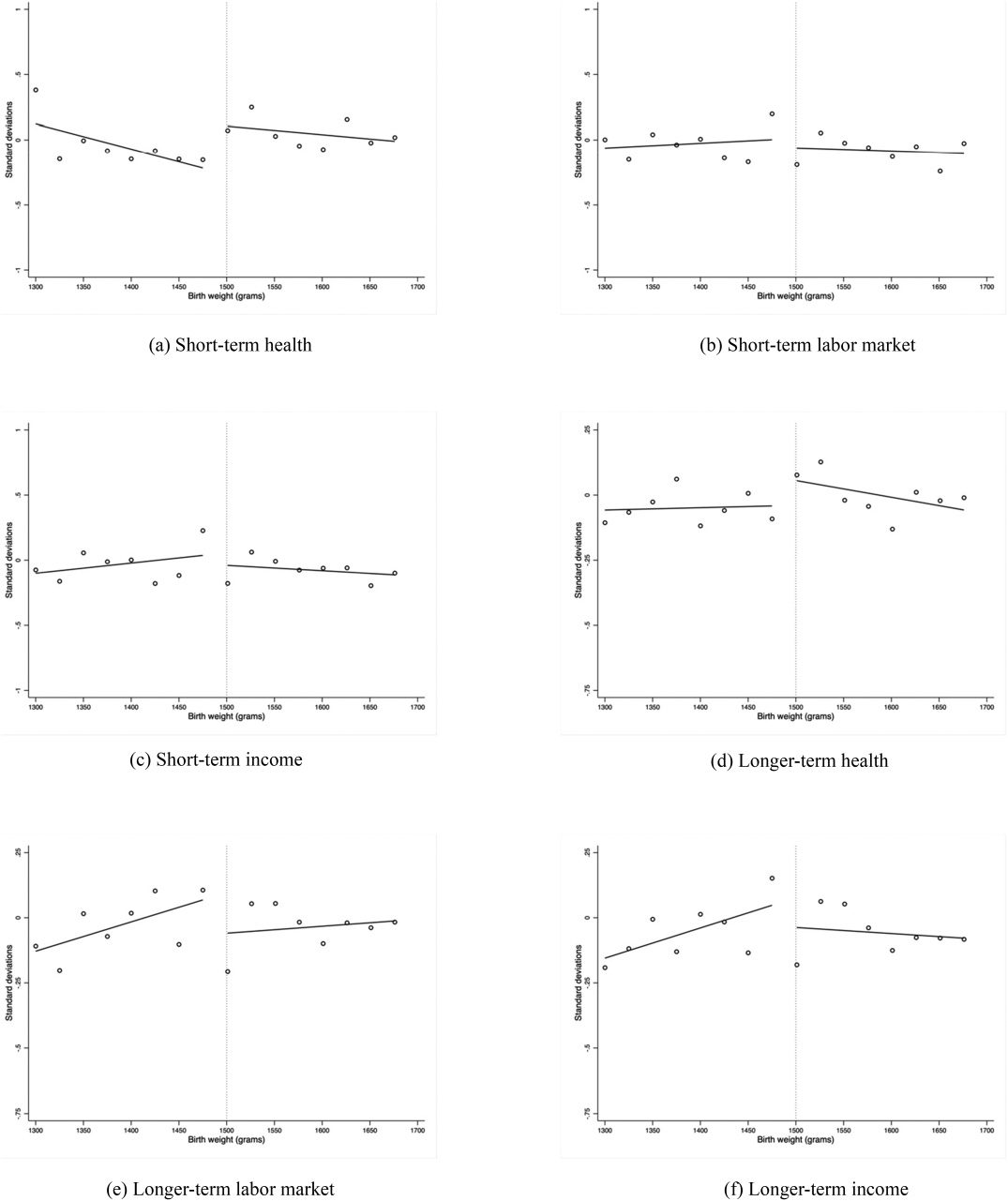
Finally, in figures 3 and 4 and in the remaining columns
of tables 2 and 3, we examine potential spillovers to parental
outcomes. Figure 3 suggests that the mothers of VLBW new-
borns have potentially better mental health, as proxied by
reduced antidepressant use, than do the mothers of heavier
babies. On the other hand, there are no apparent disconti-
18Among the test takers in the sibling sample, the maximum age difference
between older siblings and focal children is 7.6 years, meaning that none
of the older siblings take the test before the focal children are born.
nuities in maternal labor market outcomes or income, and
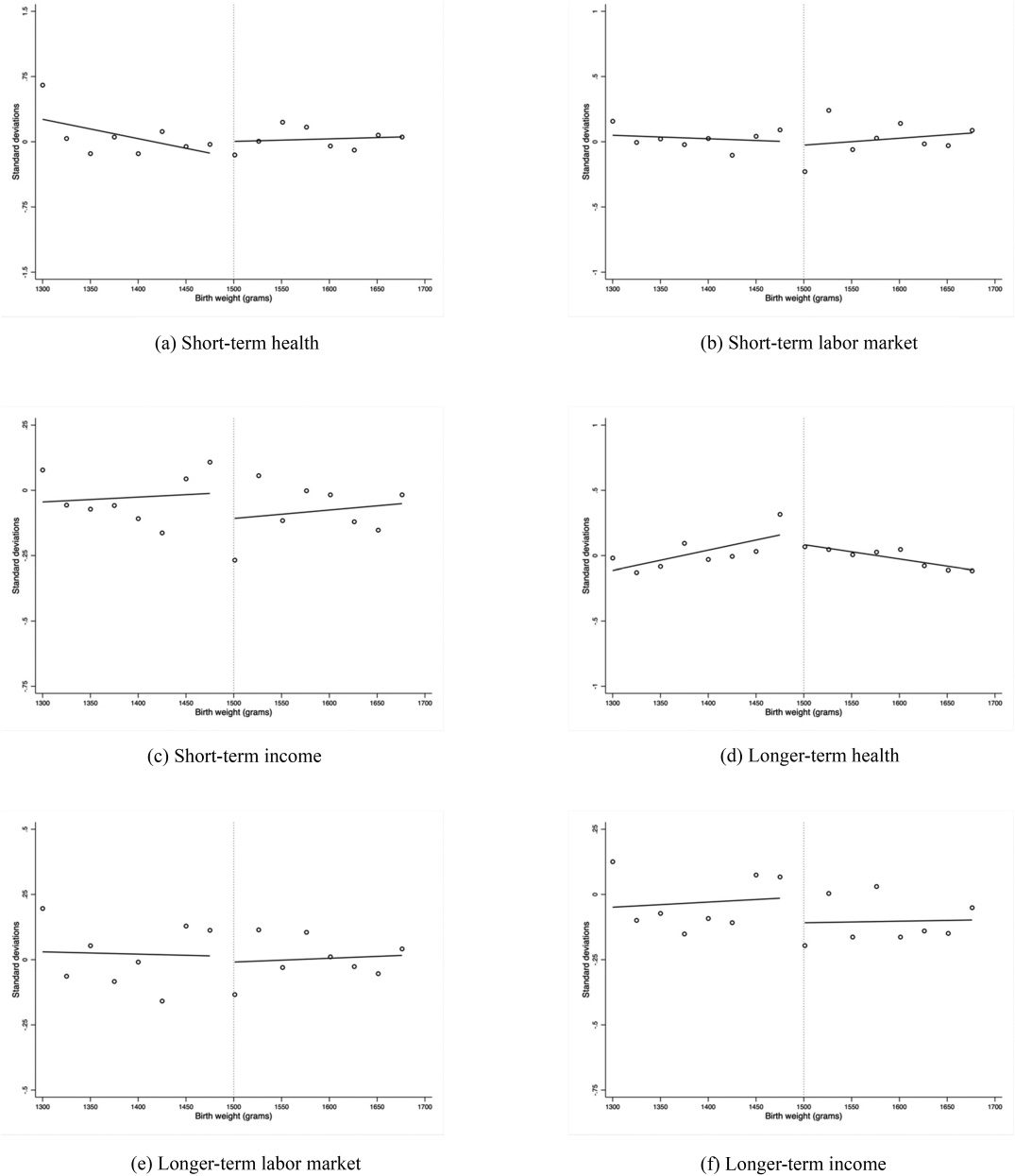
surely not immediately after the birth of the focal child. Fig-
ure 4 similarly shows that the distributions of paternal labor
market outcomes and income are generally smooth across
the VLBW cutoff. However, the fathers of VLBW newborns
do not seem to experience the mental health improvements
enjoyed by the mothers. The corresponding regression re-
sults reported in columns 3 and 4 of tables 2 and 3 confirm
the visual evidence. We generally do not find significant dis-
continuities at the VLBW cutoff in the measures of family
resources (parental labor market outcomes and income). In
the few cases when we find marginally significant gains, the
results do not survive the adjustment for multiple inference:
the lowest q-value is 0.213. However, we do find evidence
10
THE REVIEW OF ECONOMICS AND STATISTICS
FIGURE 3.—EVOLUTION OF SUMMARY INDICES OF MOTHERS OF FOCAL CHILDREN AROUND THE VLBW CUTOFF
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Sample of mothers of focal children with gestational age of at least 32 weeks. Each dot represents the average of the summary index indicated in the panel for a 40 g bin. Mothers of focal children with birth weight of
1,500 g are excluded. The lines plot a first-degree polynomial estimated separately on either side of the VLBW cutoff.
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
11
FIGURE 4.—EVOLUTION OF SUMMARY INDICES OF FATHERS OF FOCAL CHILDREN AROUND THE VLBW CUTOFF
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
Sample of fathers of focal children with gestational age of at least 32 weeks. Each dot represents the average of the summary index indicated in the panel for a 40 g bin. Fathers of focal children with birth weight of
1,500 g are excluded. The lines plot a first-degree polynomial estimated separately on either side of the VLBW cutoff.
12
THE REVIEW OF ECONOMICS AND STATISTICS
of improved maternal mental health soon after the birth of
the focal child that dissipates as the child ages. In particular,
our results indicate that antidepressant use by the mothers
of VLBW newborns is on average 0.347 standard deviation
lower. Consistent with the visual evidence in figure 4, we find
no evidence of a similar effect for the fathers.
C. Robustness Checks
In this section we present robustness checks for the in-
dices that were statistically significant in the baseline regres-
sions and survived the adjustment for multiple inference: fo-
cal child mortality, focal child long-term health, focal child
test scores, sibling test scores, and maternal short-term health
(appendix figures A6 to A8 and A10 to 12 and appendix ta-
ble A5 provide the corresponding checks for the remaining
indices). Appendix figure A5 and column 1 of appendix table
A4 investigate the robustness of our estimates to the choice
of bandwidth. Appendix figure A5 presents the results for all
bandwidths between 100 and 300 grams in 10 gram steps.
Our baseline effect is indicated with a square, and the verti-
cal bars plot the corresponding 95% robust confidence inter-
val following Calonico et al. (2014, 2019). The figure shows
that the magnitudes of the estimates are remarkably consis-
tent across different bandwidths. In column 1, we allow the
bandwidths to differ across outcomes using the optimal band-
widths suggested by the Calonico et al. (2014) strategy. Given
the stability of the estimates to alternative bandwidths, it is
not surprising that the results are again very robust.
We next check the sensitivity of our results to the choice of
degree of polynomial in birth weight. The results in column
2 show that our findings are robust to using a second degree
of polynomial. Column 3 investigates the sensitivity of the
results to the inclusion of the control variables described in
section IV. If the key assumption in our RD design is satisfied
(i.e., birth weight is as good as random around the cutoff),
then including additional relevant covariates should not affect
the estimates much but increase precision instead. The results
show that this is generally the case.
Columns 4 and 5 turn to the role of heaping. Heaping can
lead to biased estimates if it does not occur in a symmetric
way around the cutoff. Following Barreca et al. (2011, 2016),
our main specification controls for heaping at 50 gram inter-
vals. We conduct two checks to probe this further. First, we
estimate models excluding the heaping dummies (column 4).
Second, in column 5 we estimate “doughnut” regressions that
exclude the (family members of) focal children who weighed
1,500 grams (Barreca et al., 2016). The results are again sim-
ilar to the main estimates, suggesting that our baseline results
are not driven by heaping.
Our baseline model uses a triangular kernel. In column 6,
we show that our findings are robust to using a rectangular
kernel that places equal weights on each observation. Col-
umn 7 checks the sensitivity of our inference by clustering
standard errors at the birth weight level and confirms that the
results remain statistically significant at conventional levels.
Finally, we conduct two falsification tests. First, we esti-
mate our baseline model in the sample of (family members
of) focal children with a gestational age of less than 32 weeks.
Since these children are eligible to receive additional medical
treatments regardless of their birth weight, any discontinuity
in their outcomes or in the outcomes of their family members
would suggest a violation of the key identification assump-
tions underlying the RD design. The results in column 8 indi-
cate that the indices studied are relatively smooth across the
VLBW threshold in this sample.
Second, we check whether we observe similar disconti-
nuities in the indices at other points in the distribution of
birth weight of the focal child. If the observed gains are in-
deed driven by the medical treatments received by focal chil-
dren, then we should not observe systematic discontinuities
in the outcomes at other potential cutoffs. We examine cut-
offs from 1,300 grams to 3,100 grams, keeping the bandwidth
fixed at 200 grams. The results presented in appendix figure
A9 indicate that the discontinuities observed at 1,500 grams
are indeed distinct. Although the effects at 1,300 grams are
more noisily estimated, it is clear in most figures that the
largest and only significant discontinuity is found at 1,500
grams.19 Overall, these findings strongly suggest that the ob-
served (spillover) effects are due to the impact of medical
treatments provided to the VLBW focal children.
D. Discussion
In section I, we confirm the findings in the previous liter-
ature that early-life medical treatments have significant ef-
fects on focal child survival and academic achievement. In
order to compare our findings with the previous literature,
we present the results using selected components of the mor-
tality and the test score indices in appendix table A6. We
show that the probability of death within the first 28 days
(1 year) of life is 4.1 (5.4) percentage points lower among
VLBW newborns. These are large gains when compared to
the average mortality rates of those above the cutoff (6.2%
and 7.7%, respectively) but they are comparable in magnitude
to the reductions in infant mortality from previous studies: 1
percentage point (mean: 5.5%) in the United States (Almond
et al., 2010), 4.5 percentage points (mean: 11%) in Chile, and
3.1 percentage points (mean: 3.6%) in Norway (Bharadwaj
et al., 2013). We find that VLBW newborns have language
and math test scores higher on average by 0.229 and 0.315
standard deviations, respectively.20 The estimated effect on
math test scores is comparable to those found by Bharad-
waj et al. (2013), who estimate effects of 0.152 standard
19In the case of focal child and sibling test scores, we also find marginally
significant discontinuities at 2,500 grams, another birth weight cutoff for
specialized medical treatments. These effects are three to four times smaller
than the estimated effects at 1,500 grams.
20These results are not driven by delayed school entry as proxied by the
age at which focal children take the ninth-grade test (Landersø, Nielsen,
& Simonsen, 2017). Indeed, we find that the distribution of the age when
focal children take the test is smooth across the VLBW threshold (estimate
−0.033, b.c.e. −0.115, s.e. 0.127, mean 16.137).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
13
deviation in Chile and 0.476 standard deviation in Norway.
We add to this literature by investigating effects on focal child
human capital accumulation beyond compulsory schooling
as well as disability and hospital/ER contacts. We do not find
effects on enrollment beyond compulsory schooling. Further
analyses based on individual components of the index show
that there is also no impact on the “intensive” margin, as the
share of focal children enrolled in an academic track at age
18 is not significantly higher among VLBW children (see
appendix table A6). In order to reconcile the test score gains
with the lack of effects on enrollment, we estimate a quantile
RD specification based on the method proposed by Frandsen,
Frölich, and Melly (2012). The results presented in appendix
table A9 indicate that early-life medical treatments do not
improve the test scores of the focal children at the bottom
of the test score distribution. This suggests that the children
affected by the medical treatments are not on the margin of
dropping out or of making the choice between an academic
or a vocational track. While we also do not find any effects on
focal child disability status, our results consistently point to
health improvements during the school years, highlighting a
potential channel behind the academic achievement results.21
The main novelty in our paper is the investigation of
spillover effects to other family members. Our results sug-
gest that early-life medical interventions have little impact
on parents’ decisions that affect total household resources:
we see no discontinuity in the labor market or income in-
dices of either mothers or fathers. Since Denmark is a de-
veloped country with a particularly generous social safety
net, this may not be surprising. We do, however, find evi-
dence that early-life treatments provided to VLBW children
improve maternal mental health. The mental health gains are
short-lived and tend to dissipate as focal children age. One
natural explanation for this pattern could be improved focal
child survival. We check whether this is the case in two ways.
First, we estimate our baseline model in the sample of fam-
ily members of focal children who survive past the first year
of life. The estimated effect shown in column 1 of appendix
table A10 is smaller than our baseline estimate, suggesting
that child survival is indeed a channel through which early-
life medical treatments may affect maternal mental health.
Second, we consider several groups of focal children whom
we expect to be affected differently by early-life medical in-
terventions. For example, twins are on average lighter than
singletons, meaning that a VLBW singleton may be in poorer
health than a VLBW twin. Therefore, we would expect the
VLBW singletons in our sample to benefit more from med-
ical treatments than twins do. In addition, the large medi-
cal literature on the “fragile male” hypothesis states that the
male fetus is simply more at risk than the female fetus (Naeye
et al., 1971). Hence, we would expect that the VLBW boys in
21In order to shed some light on this, we estimate our baseline model with
the focal child test score index as the outcome while additionally controlling
for focal child long-term health index. The estimated coefficient of the
VLBW variable in this case is 0.260 (b.c.e. 0.496, s.e. 0.233).
our sample benefit more than girls from the additional treat-
ments provided to VLBW children. Indeed, columns 2 to 5
in appendix table A10 indicate that our mortality results are
driven by singletons and by boys. However, there are long-
term improvements in health across all four groups, support-
ing our earlier conclusion that early-life medical treatments
have health benefits beyond just survival. More important,
the table shows large improvements in the mental health of
the mothers of focal children with no survival benefits (twins
and girls). This suggests that general improvements in the
health of focal children, and not just their survival, is a chan-
nel behind the spillover effects on maternal mental health.
Turning to siblings, we find that early-life medical in-
terventions have economically significant long-run gains in
sibling academic achievement. The results based on course-
specific test scores presented in appendix table A8 show that
the test score gains are driven by both math and language
test scores. Siblings of VLBW newborns have on average
0.386 (0.255) standard deviation higher language (math) test
scores relative to the siblings of newborn who weigh slightly
more than 1,500 grams. One way to gauge the magnitudes of
these effects is to compare it to other policy-relevant test
score gaps. For example, among all children born during
the period covered by our sibling sample, the difference in
language (math) scores between the children of nonimmi-
grants and immigrants is 0.264 (0.404) standard deviation.
Our results imply that medical interventions are equivalent
to eliminating the language disadvantage for children of im-
migrants and reducing the gap in math scores by more than
half. We also calculate that the difference in language (math)
test scores among those born in households above the 90th in-
come percentile and those born in households below the 10th
income percentile is 0.557 (0.769) standard deviation. Our
coefficients imply that medical interventions can reduce the
income-based test score gap at age 16 by 33% to 69%. These
effects are in line with those found by Duncan and Sojourner
(2003) for income-based test score gaps at ages 3 through 8
for children exposed to an early-education program targeting
low birth weight children in the United States.
Similar to the focal child results, we find that siblings’ test
score gains do not translate into a higher likelihood of pursu-
ing education beyond the compulsory level. In contrast to the
effects on focal children, however, the results from the quan-
tile RD approach indicate that early-life medical treatments
improve the test scores of siblings across the entire test score
distribution (see appendix table A9). This seems to still not
affect the children on the margin of dropping out, likely due
to the fact that only 22% of students do not continue beyond
compulsory schooling. However, as more students from the
lower half of the test score distribution see improvements in
their academic achievement, we now find effects at the “in-
tensive” margin: siblings of VLBW children are more likely
to follow an academic track instead of a vocational track (see
appendix table A8).
These positive spillovers on academic achievement are un-
likely to be driven by correlated health shocks within the
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
14
THE REVIEW OF ECONOMICS AND STATISTICS
family that make siblings themselves more likely to receive
medical interventions early in life. The fact that we do not
observe discontinuities in the hospital/ER visits of siblings at
the cutoff offers the first evidence that this is unlikely to be
the case. We conduct two more checks to shed more light on
this issue. First, we exclude VLBW siblings and confirm that
our main results are not driven by them.22 Second, if the fam-
ilies of VLBW focal children are more prone to having health
shocks than the families of slightly heavier children, then our
human capital achievement results may capture the effects of
these unobserved family traits instead of the spillovers from
early-life medical interventions. In that case, we may expect
to see differences across the VLBW cutoff in the short-term
survival rates of older siblings before being exposed to the
VLBW focal children. Using the 28-day and 1-year mortal-
ity rate of older siblings as outcomes suggests that this is not
a concern in our context.23 The sibling spillovers are also
not driven by differential focal child survival at the cutoff. In
contrast to mother’s mental health, we find similar improve-
ments in sibling test scores to our baseline results when we
estimate the baseline model in the sample of families where
focal children survive the first year (column 1 of appendix
table A10).
The fact that we observe significant test score gains among
siblings of VLBW children without effects on total household
resources or sibling health suggests that early-life medical
treatments may be changing intrafamily interactions or the
intrahousehold allocation of resources. Data limitations do
not allow us to investigate these hypotheses directly, but we
provide indirect evidence on both. It is well understood in
economics that the family, especially parent-child interac-
tions, plays a central role in the human capital accumulation
of children (Cunha & Heckman, 2007; Cunha, Heckman,
& Schennach, 2010; Almond & Currie, 2011). In order to
shed further light on this, we estimate our baseline model
while controlling for the maternal short-term mental health
index and find that this reduces the estimated effect on sib-
ling text scores by about 50%.24 This suggests that improved
parent-child relations may be important for sibling academic
achievement.
The research also indicates that children’s early-life health
endowments have an impact on the academic outcomes of
other children in the family by changing parental investments.
Evidence of such spillover effects is found in both developing
and in developed countries, and the magnitudes of the effects
are economically large (Yi et al., 2015; Black, Devereux, &
Salvanes, 2007). We can provide some indirect evidence on
22The estimated coefficient of the VLBW variable is 0.401 (b.c.e. 0.466,
s.e. 0.205, N = 1,456) for the language test score and 0.263 (b.c.e. 0.416,
s.e. 0.183, N = 1,465) for the math test score. After excluding VLBW
siblings, only ten siblings with a gestational age below 32 weeks remain in
the sample. Dropping these from the sample does not change the results.
23The estimated coefficient of the VLBW variable is 0.016 (b.c.e. 0.027,
s.e. 0.020, N = 3,594) for 28-day mortality and 0.021 (b.c.e. 0.031, s.e.
0.022, N = 3,594) for one-year mortality.
24The estimated coefficient of the VLBW variable is 0.182 (b.c.e. 0.437,
s.e. 0.250, N = 546).
this if we make the assumption that there are dynamic com-
plementarities in the production of human capital, as Cunha
and Heckman (2007) suggested. In this case, children with
high initial endowments would benefit most from parental
investments because “skills beget skills.” To illustrate, con-
sider two children with low initial endowment, A and B, who
are identical in every respect except that A has a sibling with
birth weight slightly below the VLBW cutoff while B has
a sibling with birth weight slightly above the cutoff. If both
sets of parents engage in compensating behavior, then child
B has more resources taken away from her and allocated to
her sibling than child A does (because the VLBW sibling
of child A benefits from the additional medical treatments).
Therefore, in the long term, child B ends up with a lower
level of skills than child A. Now consider a similar pair of
identical children, C (who has a VLBW sibling) and D (who
does not), but with high initial endowment. Just as before,
child D has more resources taken away from her and so ends
up with a lower level of skills in the long term than child C.
However, because of dynamic complementarities, child D is
harmed even more by the fewer resources she receives be-
cause the return to those resources would be higher for her
than for child B. Therefore, the difference in skills between
children C and D (high initial endowment) is larger than the
difference in skills between children A and B (low ability).25
To check whether we observe this pattern in our data, we
rely on birth weight as an indicator of initial endowments
because the previous literature finds that it is highly corre-
lated with later-life academic, health, and labor market out-
comes (Black et al., 2007; Figlio et al., 2014). We define
“high-endowment” siblings as those whose birth weight is
higher than the birth weight of the median child born dur-
ing our sample period. The results, shown in appendix table
A11, suggest that high-endowment siblings benefit more than
low-endowment siblings do from the additional medical treat-
ments received by VLBW focal children. This suggests that
parental compensating behavior (possibly combined with dy-
namic complementarities in the production of human capital)
may also be one of the factors behind the observed spillover
effects.
VI. Conclusion
This paper investigates the spillover effects of early-life
medical treatments provided to VLBW children on other fam-
ily members. Using register data from Denmark, we confirm
the findings in the previous literature that VLBW children
eligible to receive early-life treatments are less likely to die
in the first year of life and have higher academic achieve-
ment in ninth grade. We add to this literature by showing that
focal children’s likelihood of having a childhood disability
25Alternatively, the difference in skills between children C and D can be
larger than the difference in skills between children A and B if parents
reallocate more resources to the focal child in order to compensate for the
larger difference in endowments within the family. This explanation is also
consistent with compensating behavior by the parents.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
SPILLOVER EFFECTS OF EARLY-LIFE MEDICAL INTERVENTIONS
15
is not affected by early-life medical treatments, but they are
still more likely to enjoy better health during school years, as
proxied by reduced hospital/ER contacts.
The main innovation in our study is that we document the
presence of spillover effects to other family members. While
total household resources do not differ between the families
of VLBW children and the families of slightly heavier new-
borns, the mothers of VLBW children are significantly less
likely to take antidepressants soon after the birth of the chil-
dren. These health gains diminish as the focal child ages.
Our results suggest that both increased focal child survival
and improvements in focal child health contribute to the im-
provements in maternal mental health. Turning to siblings,
we find that the siblings of focal children who were slightly
below the VLBW cutoff have better ninth-grade language
and math test scores. These gains are not driven by corre-
lated health shocks within the family or by differential focal
child survival at the cutoff. Instead, we present evidence sug-
gesting that improved interactions in the family and parental
compensating behavior may be important reasons behind the
spillovers to siblings.
Our results underscore the importance of health interven-
tions targeted to other family members as an important fac-
tor in the accumulation of human capital. Our findings also
have important implications for understanding the efficacy of
early-life medical interventions. In particular, they underline
the need to consider potential externalities when assessing
the net benefits of medical treatments. Finally, our results
have implications for studies on the effects of early-life health
endowments using sibling fixed-effects estimators. The fact
that we find substantial positive spillovers on the siblings of
treated children suggests that within-sibling comparisons of
achievement gains may underestimate the true impact of ini-
tial health endowments on later-life outcomes.
REFERENCES
Adhvaryu, Achyuta, and Anant Nyshadham, “Endowments at Birth and
Parents’ Investments in Children,” Economic Journal 126 (2016),
781–820. 10.1111/ecoj.12186
Almond, Douglas, and Janet Currie, “Human Capital Development before
Age Five,” in Orley Ashenfelter and David Card, eds., Handbook of
Labor Economics (Amsterdam: North-Holland, 2011).
Almond, Douglas, Janet Currie, and Valentina Duque, “Childhood Circum-
stances and Adult Outcomes: Act II,” Journal of Economic Literature
56 (2018), 1360–1446. 10.1257/jel.20171164
Almond, Douglas, Joseph J. Doyle, Amanda E. Kowalski, and Heidi
Williams, “Estimating Marginal Returns to Medical Care: Evidence
from At-Risk Newborns,” Quarterly Journal of Economics 125
(2010), 591–634. 10.1162/qjec.2010.125.2.591
Altonji, Joseph G., Sarah Cattan, and Iain Ware, “Identifying Sibling Influ-
ence on Teenage Substance Use,” Journal of Human Resources 52
(2017), 1–47.
Anderson, Michael L., “Multiple Inference and Gender Differences in
the Effects of Early Intervention: A Reevaluation of the Abecedar-
ian, Perry Preschool, and Early Training Projects,” Journal of the
American Statistical Association 103 (2008), 1481–1495. 10.1198/
016214508000000841
Barreca, Alan I., Melanie Guldi, Jason M. Lindo, and Glen R. Waddell,
“Saving Babies? Revisiting the Effect of Very Low Birth Weight
Classification,” Quarterly Journal of Economics 126 (2011), 2117–
2123. 10.1093/qje/qjr042
Barreca, Alan I., Jason M. Lindo, and Glen R. Waddell, “Heaping-Induced
Bias in Regression-Discontinuity Designs,” Economic Inquiry 54
(2016), 268–293. 10.1111/ecin.12225
Benjamini, Yoav, and Yosef Hochberg, “Controlling the False Discovery
Rate: A Practical and Powerful Approach to Multiple Testing,” Jour-
nal of the Royal Statistical Society. Series B (Methodological) 57
(1995), 289–300. 10.1111/j.2517-6161.1995.tb02031.x
Benjamini, Yoav, Abba M. Krieger, and Daniel Yekutieli, “Adaptive Lin-
ear Step-Up Procedures That Control the False Discovery Rate,”
Biometrika 93 (2006), 491–507. 10.1093/biomet/93.3.491
Bharadwaj, Prashant, Katrine Vellesen Løken, and Christopher Neilson,
“Early Life Health Interventions and Academic Achievement,”
American Economic Review 103:5 (2013), 1862–1891. 10.1257/
aer.103.5.1862
Black, Sandra E., Sanni Breining, David N. Figlio, Jonathan Guryan,
Krzysztof Karbownik, Helena Skyt Nielsen, Jeffrey Roth, and Mar-
ianne Simonsen, “Sibling Spillovers,” NBER working paper 23062
(2017).
Black, Sandra E., Paul J. Devereux, and Kjell G. Salvanes, “From the
Cradle to the Labor Market? The Effect of Birth Weight on Adult
Outcomes,” Quarterly Journal of Economics 122 (2007), 409–439.
10.1162/qjec.122.1.409
Burton, Peter, Lynn Lethbridge, and Shelley Phipps, “Children with Dis-
abilities and Chronic Conditions and Longer-Term Parental Health,”
Journal of Socio-Economics 37 (2008), 1168–1186. 10.1016/j.socec
.2007.01.032
Bütikofer, Aline, Katrine V. Løken, and Kjell Salvanes, “Infant Health Care
and Long Term Outcomes,” this REVIEW 101 (2019), 341–354.
Calonico, Sebastian, Matias D. Cattaneo, Max H. Farrell, and Roció Titiu-
nik, “Regression Discontinuity Designs Using Covariates,” this RE-
VIEW 101 (2019), 442–451.
Calonico, Sebastian, Matias D. Cattaneo, and Rocio Titiunik, “Robust Non-
parametric Confidence Intervals for Regression-Discontinuity De-
signs,” Econometrica 82 (2014), 2295–2326. 10.3982/ECTA11757
Card, David, Carlos Dobkin, and Nicole Maestas, “The Impact of Nearly
Universal Insurance Coverage on Health Care Utilization: Evidence
from Medicare,” American Economic Review 98 (2008), 2242–2258.
10.1257/aer.98.5.2242
Chay, Kenneth Y., Jonathan Guryan, and Bhashkar Mazumder, “Birth Co-
hort and the Black-White Achievement Gap: The Roles of Ac-
cess and Health Soon after Birth,” NBER working paper 15078
(2009).
Cunha, Flavio, and James Heckman, “The Technology of Skill Formation,”
American Economic Review 97 (2007), 31–47. 10.1257/aer.97.2.31
Cunha, Flavio, James Heckman, and Susanne Schennach, “Estimating
the Technology of Cognitive and Noncognitive Skill Formation,”
Econometrica 78 (2010), 883–931. 10.3982/ECTA6551
Cutler, David M., and Ellen Meara, “The Medical Costs of the Young and
Old: A Forty-Year Perspective” (pp. 215–246), in David A. Wise,
ed., Frontiers in the Economics of Aging (Chicago: University of
Chicago Press, 1998).
Dahl, Gordon, Katrine V. Løken, and Magne Mogstad, “Peer Effects in Pro-
gram Participation,” American Economic Review 104 (2-14), 2049–
2074. 10.1257/aer.104.7.2049
Danish Ministry of Health and Prevention [Ministeriet for Sundhed og For-
byggelse], “Health Care in Denmark” (2008).
Daysal, N. Meltem, Mircea Trandafir, and Reyn van Ewijk, “Saving Lives at
Birth: The Impact of Home Births on Infant Outcomes,” American
Economic Journal: Applied Economics 7 (2015), 1–24. 10.1257/
app.20120359
——— “Low-Risk Isn’t No-Risk: Perinatal Treatments and the Health of
Low-Income Newborns,” Journal of Health Economics 64 (2019),
55–67. 10.1016/j.jhealeco.2019.01.006, PubMed: 30797113
Deshpande, Manasi, “Does Welfare Inhibit Success? The Long-Term Ef-
fects of Removing Low-Income Youth from the Disability Rolls,”
American Economic Review 106 (2016), 3300–3330. 10.1257/
aer.20151129
Dong, Yingying, “Regression Discontinuity Applications with Rounding
Errors in the Running Variable,” Journal of Applied Econometrics
30 (2015), 422–446. 10.1002/jae.2369
Duncan, Greg J., and Aaron J. Sojourner, “Can Intensive Early Child-
hood Intervention Programs Eliminate Income-Based Cognitive and
Achievement Gaps?” Journal of Human Resources 48:4 (2003),
945–968.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3
16
THE REVIEW OF ECONOMICS AND STATISTICS
Field, Erica, Omar Robles, and Maximo Torero, “Iodine Deficiency and
Schooling Attainment in Tanzania,” American Economic Journal:
Applied Economics 1 (2009), 140–169. 10.1257/app.1.4.140
Figlio, David, Jonathan Guryan, Krzysztof Karbownik, and Jeffrey Roth,
“The Effects of Poor Neonatal Health on Children’s Cognitive De-
velopment,” American Economic Review 104 (2014), 3921–3955.
10.1257/aer.104.12.3921
Frandsen, Brigham R., Markus Frölich, and Blaise Melly, “Quan-
tile Treatment Effects in the Regression Discontinuity De-
sign,” Journal of Econometrics 168 (2012), 382–395. 10.1016/
j.jeconom.2012.02.004
Greisen, G., M. B. Petersen, S. A. Pedersen, and P. Bekgaard, “Sta-
tus at Two Years in 121 Very Low Birth Weight Survivors Re-
lated to Neonatal lntraventricular Haemorrhage and Mode of De-
livery,” Acta Paediatrica Scandinavica 75 (1986), 24–30. 10.1111/
j.1651-2227.1986.tb10152.x
Gunnsteinsson, Snaebjorn, and Herdis Steingrimsdottir, “The Long-Term
Impact of Children’s Disabilities on Families,” Copenhagen Busi-
ness School mimeograph (2019).
Heissel, Jennifer A., “Teen Fertility and Siblings’ Outcomes: Evidence of
Family Spillovers Using Matched Samples.” Journal of Human Re-
sources (forthcoming).
Hertz, Birgitte, Eva-Bettina Holm, and Jørgen Haahr, “Prognosen for børn
med meget lav fødselsvægt i Viborg Amt,” Ugeskrift for læger 156
(1994), 6865−6868.
Hjort, Jonas, Mikkel Sølvsten, and Miriam Wüst, “Universal Investment
in Infants and Long-Run Health: Evidence from Denmark’s 1937
Home Visiting Program,” American Economic Journal: Applied
Economics 9 (2017), 78–104. 10.1257/app.20150087
Jacobsen, Thorkild, John Grønvall, Sten Petersen, and Gunnar Eg An-
dersen, “‘Minitouch’ Treatment of Very Low-Birth-Weight In-
fants,” Acta Paediatrica Scandinavica 82 (1993), 934–938. 10.1111/
j.1651-2227.1993.tb12603.x
Joensen, Juanna, and Helena Skyt Nielsen, “Spillovers in Educational
Choice,” Journal of Public Economics 157 (2018), 158–183.
10.1016/j.jpubeco.2017.10.006
Johnson, T. J., A. L. Patel, B. J. Jegier, J. L. Engstrom, and P. Meier, “Cost of
Morbidities in Very Low Birth Weight Infants,” Journal of Pediatrics
162 (2013), 243–249e1. 10.1016/j.jpeds.2012.07.013
Jürges, Hendrik, and Juliane Köberlein, “What Explains DRG Upcoding in
Neonatology? The Roles of Financial Incentives and Infant Health,”
Journal of Health Economics 43 (2015), 13–26.
Kvist, Anette Primdal, Helena Skyt Nielsen, and Marianne Simonsen, “The
Importance of Children’s ADHD for Parents’ Relationship Stability
and Labor Supply,” Social Science and Medicine 88 (2013), 30–38.
10.1016/j.socscimed.2013.04.001, PubMed: 23702207
Landersø, Rasmus, Helena Skyt Nielsen, and Marianne Simonsen, “School
Starting Age and the Crime-Age Profile,” Economic Journal 127
(2017), 1096–1111.
Mathiasen, René, Bo M. Hansen, Anne Løkke, and Gorm Greisen, “Behan-
dling af tidligt fødte børn på Rigshospitalet i perioden 1955–2007”
(Treatment of preterm children at Rigshospitalet during the period
1955–2007), Bibliotek for Læger 200 (2008), 528–546.
McCrary, Justin, “Manipulation of the Running Variable in the Regression
Discontinuity Design: A Density Test,” Journal of Econometrics 142
(2008), 698–714. 10.1016/j.jeconom.2007.05.005
Naeye, Richard L., Leslie S. Burt, David L. Wright, William A. Blanc,
and Dorothy Tatter, “Neonatal Mortality, the Male Disadvantage,”
Pediatrics 48 (1971), 902–906.5129451
Newhouse, Joseph P., “Medical Care Costs: How Much Welfare Loss?”
Journal of Economic Perspectives 6 (1992), 3–21. 10.1257/
jep.6.3.3, PubMed: 10128078
Nicoletti, Cheti, and Birgitta Rabe, “Sibling Spillover Effects in School
Achievement,” Journal of Applied Econometrics 34 (2019), 482–
501. 10.1002/jae.2674
Oreopoulos, Philip, “Estimating Average and Local Average Treatment
Effects of Education When Compulsory Schooling Laws Really
Matter,” American Economic Review 96 (2006), 152–175. 10.1257/
000282806776157641
Peitersen, Birgit, and Mette Arrøe, Neonatologi—Det raske og det syge
nyfødte barn (Copenhagen: Nyt Nordisk Forlag Arnold Busck,
1991).
Powers, Elizabeth T., “Children’s Health and Maternal Work Activity,”
Journal of Human Resources 38 (2003), 522–556. 10.2307/1558767
Schieve, Laura A., Lin H. Tian, Kristin Rankin, Michael D. Kogan,
Marshalyn Yeargin-Allsopp, Susanna Visser, and Deborah Rosen-
berg, “Population Impact of Preterm Birth and Low Birth Weight
on Developmental Disabilities in US Children,” Annals of Epi-
demiology 26 (2016), 267–274. 10.1016/j.annepidem.2016.02.012,
PubMed: 27085382
Schiøtz, Peter Oluf, and Skovby, Flemming, Praktisk pædiatri (Copen-
hagen: Munksgaard Danmark, 2001).
Shigeoka, Hitoshi, and Kiyohide Fushimi, “Supplier-Induced Demand
for Newborn Treatment: Evidence from Japan,” Journal of Health
Economics 35 (2014), 162–178. 10.1016/j.jhealeco.2014.03.003,
PubMed: 24709038
Thomsen, Ketty Dahl, Helle Hansen, Finn Ebbesen, and Vibeke Jacobsen,
“Neonatal mortalitet hos børn med meget lav fødselsvægt i Nord-
jyllands Amt: en retrospektiv opgørelse,” Ugeskrift for læger 153
(1991), 3310−3313.
Topp, Monica, Peter Uldall, and Gorm Greisen, “Cerebral Palsy Births in
Eastern Denmark, 1987–90: Implications for Neonatal Care,” Pae-
diatric and Perinatal Epidemiology 15 (2001), 271–277. 10.1046/
j.1365-3016.2001.00354.x, PubMed: 11489156
Verder, Henrik, “Nasal CPAP Has Become an Indispensable Part of the Pri-
mary Treatment of Newborns with Respiratory Distress Syndrome,”
Acta Pædiatrica 96 (2007), 482–484.
Verder, Henrik, Bengt Robertson, Gorm Greisen, Finn Ebbesen, Per Albert-
sen, Kaare Lundstrøm, and Thorkild Jacobsen, “Surfactant Therapy
and Nasal Continuous Positive Airway Pressure for Newborns with
Respiratory Distress Syndrome,” New England Journal of Medicine
331 (1994), 1051–1055. 10.1056/NEJM199410203311603
Yi, Junjian, James Heckman, Junsen Zhang, and Gabriella Conti, “Early
Health Shocks, Intra-Household Resource Allocation and Child
Outcomes,” Economic Journal 125 (2015), F347–F371. 10.1111/
ecoj.12291
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
r
e
s
t
/
l
a
r
t
i
c
e
-
p
d
f
/
/
/
/
1
0
4
1
1
1
9
8
0
1
6
1
/
r
e
s
t
_
a
_
0
0
9
8
2
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
8
S
e
p
e
m
b
e
r
2
0
2
3