Journal of Interdisciplinary History, LIII:3 (Winter, 2023), 439–469.
Asher Colombo and Rocco Molinari
Displacement of Death from Home to Hospital in
Historical Perspective: The Case of Italy, 1883–2013
THE RESEARCH PROBLEM The progressive displacement of the site
of death from home to hospital settings, far from both public and
domestic eyes, has been one of the most important changes in the
experience of death throughout the twentieth century. Histori-
cally, in Europe people died at home (and often, if male, on the
battlefield). Until the beginning of the twentieth century, hospitals
were more shelters for the destitute than institutions for the sick.
These institutions were under the management of religious orders,
not physicians, and their meaning was associated less with the
opportunity to receive treatment and therapies than charity. Hos-
pitals were clearly perceived as places to be avoided. Progress in
medical knowledge and techniques since the eighteenth century
slowly challenged this situation. During the nineteenth century,
hospitals began to play the role of institutions for the sick, firmly
placed under the guide of physicians.
Slowly a shift in the place of death emerged. Due to a lack of
accurate time series, the timing is not completely clear, but in
Scandinavian countries, deaths in hospitals had reached 10 percent
by the first decade of the twentieth century, 30 percent in the
1950s, and 50 percent in the 1960s. In Norway, more than 70 percent
Asher Colombo is Professor of Sociology at the University of Bologna and President of the
Carlo Cattaneo Research Institute in Bologna. He is author of “Why Europe Has Never Been
United (Not Even in the Afterworld): The Fall and Rise of Cremation in the Cities (1876–
1939),” Death Studies, XLI (2017), 22–33; co-author, with Eleonora Vlach, “Why Do We Go
to the Cemetery? Religion, Civicness, and the Cult of the Dead in Twenty-First Century
Italy,” Review of Religious Research, LXIII (2021), 217–243; co-author, with Gianpiero
Dalla-Zuanna, “Immigration Italian Style, 1977–2018,” Population and Development Review,
XLV (2019), 586–615.
Rocco Molinari is Research Fellow in the Department of Political and Social Sciences at
the University of Bologna.
For extensive comments and discussion of previous versions of the content and analysis in
this article, the authors are indebted to Hans M. A. Schadee (1945–2021), Professor of Quan-
titative Methods in Social-Science Research at the University of Milan, a guide and friend.
This work was supported by the Italian Ministero dell’Istruzione, dell’Università e della
Ricerca (MIUR) under Grant 2015FR7MKM in the framework of the PRIN research
project “Death, Dying and Disposal in Italy: Attitudes, Behaviours, Beliefs, Rituals.”
© 2022 by the Massachusetts Institute of Technology and The Journal of Interdisciplinary
History, Inc., https://doi.org/10.1162/jinh_a_01870
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
440
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
of deaths occurred in hospitals during the 1970s. This shift started a
little later in Mediterranean countries and never achieved the level
registered in northern and central Europe or the United States. In
Italy slightly more than 10 percent of deaths occurred in hospitals
during the 1930s and 30 percent was reached only in the 1970s. The
peak was registered in 2010, when 45 percent of all deaths occurred
in hospitals. The pace of Spain and Portugal was even slower.1
The process is at the center of many competing but partially
overlapping concepts in social science, like “medicalization,”
“institutionalization,” or “sequestration.” But while there are many
concepts to define the process, empirical research is lacking as to
the long-term change in the site of death from home to hospital.2
The aim of this Research Note is to investigate further the his-
torical correlates of this emerging hospitalization of death, that is,
the shift in the place of death from home to hospital, in one
country—Italy—over more than a century, so as to cover the entire
relevant period. Four sociological schemas are considered to explain
the change: the “forbidden death” thesis, the civilization process,
institutionalization, and everyday practices.
According to the first explanation, the twentieth century saw
the birth and development of a new attitude toward death,
whereby it was hidden from public places and confined to the pri-
vate sphere. A wide range of changes embodied this shift. People
began to avoid showing grief in public and began to follow certain
rules of bereavement; far more deaths occurred in hospitals than at
home, compared to the past; physicians started to share less
1 These data come from administrative printed sources collected by one of the authors. For
the historical perception of hospitals as places to be avoided, see Glennys Howarth, Death and
Dying: A Sociological Introduction (Cambridge, 2007), 115–131; Roslyn Lindheim, “Birthing
Centers and Hospices: Reclaiming Birth and Death,” Annual Review of Public Health,
II (1981), 1–29.
2 For the interference of medicine on social life, see Howarth, Death and Dying; Lindheim,
“Birthing Centers”; Ivan Illich, Limits to Medicine: Medical Nemesis: The Expropriation of Health
(London, 1976); Michel Foucault, The Birth of the Clinic: An Archaeology of Medical Perception
(London, 1973); Irving K. Zola, “Medicine as an Institution of Social Control,” Sociological
Review, XX (1972), 487–504. For the sequestration of death, see Howarth “Whatever
Happened to Social Class? An Examination of the Neglect of Working Class Cultures in
the Sociology of Death,” Health Sociology Review, XVI (2007), 425–435, 427; Clive Seale, Con-
structing Death: The Sociology of Dying and Bereavement (Cambridge, 1998); Philip A. Mellor and
Chris Shilling, “Modernity: Self-Identity and the Sequestration of Death,” Sociology, XXVII
(1993), 411–431; Anthony Giddens, Modernity and Self-Identity: Self and Society in the Late Mod-
ern Age (Stanford, 1991).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
441
information with their patients on serious illness; rapid changes in
the funeral industry deeply affected rites and the ways people hon-
ored the dead; and in Western Europe and the United States the
number of cremations increased as a way of disposing of the dead
and as a funeral rite, even to the point of exceeding burials, hence
the diminishing of the cult of graves, cemeteries, and the dead. In
short, the main idea underlying this line of reasoning is that any-
thing to do with death became more and more hidden and pri-
vate, a process that Ariés called “forbidden death.”3
Within the context of this general turn, the place of death
moved from home to hospital due to two main processes. First,
dying at home became increasingly harder in twentieth-century
Europe’s big cities, which were devoid of the social networks of
friends, neighbors, and kinship typical of the countryside. Addi-
tionally, growing urbanization had spread the urban condition
beyond the cities. Second, changes in family structure, with the
fading of the extended household and the growth of nuclear
3 Geoffrey Gorer, Death, Grief, and Mourning in Contemporary Britain (London, 1965). For
ethnographic research on the pattern of denial of death, see Marco Marzano, Scene Finali.
Morire di Cancro in Italia (Bologna, 2004); David Sudnow, Passing On: The Social Organization
of Dying (Englewood Cliffs, 1967); Barney G. Glaser and Anselm L. Strauss, Awareness of Dying
(Chicago, 1965). For changes in the awareness of patients, see Marzano, Scene Finali; Robert
Beilin, “Social Functions of Denial of Death,” OMEGA–Journal of Death and Dying, XII
(1982), 25–35; Avery D. Weisman, On Dying and Denying: A Psychiatric Study of Terminality
(New York, 1972); Glaser and Strauss, Time for Dying (Chicago, 1968); idem, Awareness of
Dying; Jessica Mitford, The American Way of Death (New York, 1963). For changes in the
funeral industry, see Brian Parsons, The Evolution of the British Funeral Industry in the 20th Cen-
tury: From Undertaker to Funeral Director (Bingley, 2018); idem, “Change and Development in
the British Funeral Industry during the 20th Century, with Special Reference to the Period
1960–1994” unpub. Ph.D. thesis, (Univ. of Westminster, 1997); Gary Laderman, Rest in Peace:
A Cultural History of Death and the Funeral Home in Twentieth-Century America (Oxford, 2003);
idem, The Sacred Remains: American Attitudes toward Death, 1799–1883 (New Haven, 1996); Peter
L. Berger and Richard Lieban, “Kulturelle Wertstruktur und Bestattungspraktiken in den
Vereinigten Staaten,” Kölner Zeitschrift Für Soziologie und Sozialpsychologie, XII (1960), 224–
236. For changes in disposal practices, see Robert Redeker, L’éclipse de la Mort (Paris,
2018); Marco Breschi, Gabriele Ruiu, and Marco Francini “‘Ashes to Ashes…’: Could the
Recent Evolution of the Cremation Practice in Italy Be Interpreted as an Indication of Secu-
larisation?” Review of Religious Research, LX (2018), 519–533; Breschi and Francini, “Il Lungo
Lento Inesorabile Affermarsi del Rito Crematorio in Italia,” Popolazione e Storia, XVIII (2017),
81–98; Colombo, “Why Europe Has Never Been United (Not Even in the Afterworld): The
Fall and Rise of Cremation in Cities (1876–1939),” Death Studies, XLI (2017), 22–33; Peter C.
Jupp, From Dust to Ashes: Cremation and the British Way of Death (New York, 2006); idem, “The
Development of Cremation in England 1820–1990: A Sociological Analysis” unpub. Ph.D.
thesis, (Univ. of London, 1993); Stephen Protero, Purified by Fire: A History of Cremation in
America (Berkeley, 2001).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
442
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
families, made it harder to give proper care to the elderly and to
accept the lower level of privacy typical of an extended household.
Growing secularization did the rest, pushing the sick out of the
home and into the hospital.4
A different explanation comes from the field of historical
sociology. According to Elias, the rise in the number of deaths in
hospitals is part of a wider, centuries-long historical process. This
process has gradually moved death to the backstage of social life
(the hospital). Elias mentions four preconditions of that process:
(1) increasing average life expectancy; (2) the experience of death
as the final stage in a natural process, mainly due to progress in
medical science; (3) the high degree of internal pacification within
modern society, with the decrease in deaths due to interpersonal
violence and consequent development of a new personality struc-
ture based on “repression of affections,” that is, anti-social emotions
and attitudes; and (4) a high degree of individualization.5
The third main hypothesis comes from sociology. According to
Parsons and colleagues, the shift from home to hospital was to be
considered merely part of the success of a specific, modern, “active”
attitude aimed at gaining more technical control over death. The
search for complete control over death also underlies the classic
analysis of the place of death in traditional and modern society as
developed by Blauner. According to Blauner, modern society is
more able to control death, so the power and status of dying people
decreases, and they are moved from a preferred place, home, to an
unwelcome one, hospital, where the physicians’ power resides.6
4 Michel Vovelle, La Mort et l’Occident: De 1300 à Nos Jours (Paris, 1983); Philippe Ariès,
L’Homme Devant la Mort (Paris, 1977); idem, Western Attitudes Toward Death: From the Middle
Ages to the Present (Baltimore, 1974), 85–87.
5 Norbert Elias, The Loneliness of the Dying (London, 2001; orig. pub. 1979), 43–45; Liz Stan-
ley and Sue Wise, “The Domestication of Death: The Sequestration Thesis and Domestic
Figuration,” Sociology, XLV (2011), 947–962.
6 Talcott Parsons, “Death in the Western World,” in idem (ed.), Action Theory and the Human
Condition (New York, 1978); idem, “Death in American Society—A Brief Working Paper,”
American Behavioral Scientist, VI (1963), 61–65; idem, Renée C. Fox, and Victor M. Lidz, “The
‘Gift’ of Life and Its Reciprocation,” Social Research, XXXIX (1972), 367–415; Talcott Par-
sons and Lidz, “Death in American Society,” in Edwin S. Schneidman (ed.), Essays in Self
Destruction (New York, 1967), 133–170; Robert Blauner, “Death and Social Structure,” Psy-
chiatry, XXIX (1966), 378–394. For the scientific construction of death, see Seale, Construct-
ing Death: The Sociology of Dying and Bereavement (Cambridge, 1998), 54. For science as a
driver of the hospitalization of death, see Howarth, Death and Dying, 117.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
443
Finally, the last explanation argues that the management of
dying people in Europe has historically been performed by
women at home. The growth of women’s participation in the
labor market resulted in a retreat from informal care work and
sometimes in entry into the formal labor market of caregiving,
given that the majority of hospital nurses, hospice personnel,
and caregivers in residential homes are female. This process has
intertwined with long-term changes in household structure and
size. The long demise of the extended household and the spread-
ing of nuclear families in the Western world resulted in a sharp
reduction in the number of elderly persons living with relatives
or with family members from the younger generation. This meant
there were fewer opportunities to keep the sick at home and
strong organizational pressure to move them to hospitals. Reduc-
tion of space in modern dwellings tended toward the same end.7
Place of Death in Empirical Research Empirical studies investi-
gating where people die have generally been driven by two objectives,
describing the location-of-death composition and its changes over
time, and identifying which individual and (less frequently) which
environmental factors are mostly associated with the place of death.
The large prevalence of hospitalized death emerges from these
research studies as a common trait in many different contexts. Fur-
thermore, as the few studies adopting a long-term perspective have
shown, throughout the second half of the twentieth century, many
countries experienced a pattern of growing hospitalization and a
decline in the home as the site of death.8
7 For implications of changes in household structure, see Michael C. Kearl, Endings: A Soci-
ology of Death and Dying (Oxford, 1989), 127–128; Lindheim, “Birthing Centers,” 18. For the
importance of the changing role of women, see Howarth, Death and Dying, 116.
8 Barbara Gomes and Irene J. Higginson, “Where People Die (1974–2030): Past Trends,
Future Projections and Implications for Care,” Palliative Medicine, XXII (2008), 33–41; Limin
Yang, Naoko Sakamoto, and Eiji Marui, “A Study of Home Deaths in Japan from 1951 to
2002,” BMC Palliative Care, V (2006), 1–9; Donna M. Wilson, Herbert C. Northcott, Corrine
D. Truman, Susan L. Smith, Marjorie C. Anderson, Robin L. Fainsinger, and Michael J.
Stingl, “Location of Death in Canada: A Comparison of 20th-Century Hospital and Nonhos-
pital Locations of Death and Corresponding Population Trends,” Evaluation & the Health Pro-
fessions, XXIV (2001), 385–403; Roger W. Hunt, Malcolm J. Bond, Robyn K. Growth, and
Penny M. King, “Place of Death in South Australia: Patterns from 1910 to 1987,” Medical
Journal of Australia, CLV (1991), 549–553. For a cross-country comparison, see Joanna B.
Broad, Merryn Gott, Hongsoo Kim, Michal Boyd, He Chen, and Martin J. Connolly,
“Where Do People Die? An International Comparison of the Percentage of Deaths Occurring
in Hospital and Residential Aged Care Settings in 45 Populations, Using Published and Avail-
able Statistics,” International Journal of Public Health, LVIII (2013), 257–267.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
444
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
Nonetheless, studies that narrowed the analysis to recent years
also noticed a slowdown in the more-than-century-long process of
displacement of death. This downturn was due mainly to the recent
emergence of hospices and nursing homes as replacements for
hospitals in end-of-life welfare management. In some cases, this
trend combines with a small resurgence of the home as the place
of death.9
One strand of empirical research at variance with this descrip-
tive picture has been devoted to understanding the factors associ-
ated with the place of death, typically distinguishing between
home, hospital, and other institutions. One of the most common
findings is that causes of death are relevant to the place of dying.
Terminally ill patients with cancer or other chronic diseases are
generally observed to die in hospitals more frequently. Further-
more, some studies support the idea that a cohesive household
structure and solid family resources affect the place of death. This
has been observed through environmental-level indicators, show-
ing that territories with a larger average household size and fewer
families in which the elderly live alone are more likely to be asso-
ciated with higher home death rates. This finding is also supported
by individual-level indicators. Having a partner, being married, or
living in a multi-person household is indeed associated with higher
probability of dying at home and a lower chance of a hospitalized
death. Moreover, elderly people having a close family member as
first caregiver, as opposed to a social worker, are more likely to die
9 Burkhard Dasch, Klaus Blum, Philipp Gude, and Claudia Bausewein “Place of Death:
Trends Over the Course of a Decade: A Population-Based Study of Death Certificates from
the Years 2001 and 2011,” Deutsches Ärzteblatt, CXII (2015), 496–504; Wei Gao, Yuen K. Ho,
Julia Verne, Emma Gordon, and Higginson, “Geographical and Temporal Understanding in
Place of Death in England (1984–2010): Analysis of Trends and Associated Factors to Improve
End-of-Life Care (GUIDE_Care)—Primary Research,” Health Services and Delivery Research, II
(2014), 1–104; Gomes, Natalia Calanzani, and Higginson, “Reversal of the British Trends in
Place of Death: Time Series Analysis 2004–2010,” Palliative Medicine, XXVI (2012), 102–107;
Dirk Houttekier, Joachim Cohen, Johan Surkyn, and Luc Deliens, “Study of Recent and
Future Trends in Place of Death in Belgium Using Death Certificate Data: A Shift from Hos-
pitals to Care Homes,” BMC Public Health, XI (2011), 1–10; Wilson, Truman, Roger Thomas,
Fainsinger, Kathy Kovacs-Burns, Katherine Froggatt, and Christopher Justice, “The Rapidly
Changing Location of Death in Canada, 1994–2004,” Social Science & Medicine, LXVIII (2009),
1752–1758; James Flory, Yinong Young-Xu, Ipek Gurol, Norman Levinsky, Arlene Ash, and
Ezekiel Emanuel, “Place of Death: U.S. Trends since 1980,” Health Affairs, XXIII (2004),
194–200.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
445
at home than in hospitals or other institutions, which suggests the
relevance of family care.10
Many studies have found that people living in urban areas are
more likely to die in hospitals than are those in rural areas. This
aspect is also associated with the higher availability of medical facil-
ities for those living in cities, generally measured as hospital beds
per person, a factor that is observed positively to affect the chance
of dying in hospitals. Some studies also observe that the recent
decrease in death-in-hospital rates is more marked in urban areas,
where new institutions and practices are more common.11
RESEARCH DESIGN AND METHODOLOGY The aim of this Research
Note is to shift our understanding of the displacement-of-death-
from-home-to-hospital process from a cross-sectional and individual
perspective to a longitudinal framework accounting for the macro
historical forces in play.
First, the process of the hospitalization of death in Italy since
the late nineteenth century is investigated, adopting territorial-
level statistical units, that is, using provinces, as we follow their
dynamics over time.
Second, changes in the rate of deaths in hospitals are located
within the framework of other processes varying through time.
These are demographical forces (mortality reduction, changes in
the causes-of-death structure, aging), socio-structural variables
10 Danang Gu, Guangya Liu, Denese Ashbaugh Vlosky, and Zeng Yi, “Factors Associated
with Place of Death among the Chinese Oldest Old,” Journal of Applied Gerontology, XXVI
(2007), 34–57; Gao et al., “Geographical and Temporal Understanding”; Houttekier, “Place
of Death in Belgium”; Yang, Sakamoto, and Marui, “Home Death in Japan”; Hunt et al.,
“Place of Death in South Australia.” For the association between chronic diseases and place of
death, see Sophie Pennec, Joëlle Gaymu, Alain Monnier, Françoise Riou, Régis Aubry, Silvia
Pontone, and Chantal Cases, “In France, Where Do People Live in Their Last Month of Life
and Where Do They Die?” Population, IV (2013), 503–531; Gao et al., “Geographical and
Temporal Understanding”; Gomes, Calanziani, and Higginson, “Reversal of the British
Trends”; Flory et al., “U.S. Trends since 1980”; Yang, Sakamoto, and Marui “Home Death
in Japan”; Wilson et al. “Location of Death in Canada.” For a review of factors affecting
cancer patients’ location of death, see Gomes and Higginson “Factors Influencing Death at
Home in Terminally Ill Patients with Cancer: Systematic Review,” British Medical Journal,
CCCXXXII (2006), 515–521.
Jyothi Jayaraman and K. S. Joseph, “Determinants of Place of Death: A Population-Based
11
Retrospective Cohort Study,” BMC Palliative Care, XII (2013), 1–9; Dasch et al., “Place of
Death”; Gao et al., “Geographical and Temporal Understanding”; Houttekier, “Place of Death
in Belgium”; Wilson et al., “Location of Death in Canada, 1994–2004”; Gu et al., “Place of
Death Among the Chinese Oldest Old”; Yang, Sakamoto, and Marui, “Home Death in Japan.”
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
446
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
(urbanization, changes in household structure and size), medicaliza-
tion (mostly due to the increasing availability of hospital facilities),
and cultural factors (the spread of the “process of civilization” in
Elias’ meaning, and the growth of secularization, meaning declining
adherence to religious rites and practice in the Western world).
Specifically, considering the importance of demographic forces
and the availability of medical facilities that are supposed to affect the
hospitalization-of-death process and its geographical distribution, we
formulate three hypotheses. First, growing urbanization and changes
in the household structure (with fewer family members at home as
informal caregivers) increase the number of deaths in hospitals over
deaths at home. Second, according to one of the preconditions of
the “civilization process” theory, the lower the level of deaths due
to interpersonal violence (that is, the drop in the homicide ratio),
the higher the rate of deaths in hospitals. Third, the higher the level
of secularization, the higher the degree of hospitalized death.
Finally, the analysis aims to investigate specific territorial
aspects of the process of hospitalization of death by considering
whether the impacts of the aforementioned processes are geogra-
phically differentiated.
Data To explore these issues, registry data at the province
level in post-unification Italy were combined from various admin-
istrative sources, all published by the National Institute of Statistics.
The deaths-in-hospitals count was collected from the Statistics of
Patients Movements and Causes of Death registers, available by prov-
ince for 1883, 1955, 1963, 1974, 1981, 1987, 1997, 2004, and 2013.
This information was subsequently merged with data obtained at
corresponding years from Vital Statistics and Causes of Death.
Finally, further indicators at the provincial level were collected
from the Italian Population Census, which has been conducted
every ten years since 1861 (thus data from this source are slightly
asynchronous with that of the other sources).12
12 The Statistics of Patients’ Movements register collects the number of deaths occurring in
public and private hospitals, and only occasionally provides province-level statistics. Data
come from the tables “Movimento degli infermi curati negli ospedali” and “Movimento
dei ricoverati” (deaths occurring in hospitals) published in various volumes of the “Annuario
statistico italiano.” Since 2004 the same information has been provided from the Causes of
Deaths registers, which also include other places of death. The years considered for census
variables generally anticipate the timing of other indicators. Census years were 1881, 1951,
1961, 1971, 1981, 1986, 1996, 2001, and 2011. Indicators for 1986 and 1996 were estimated
by linear interpolation from the data in the 1981, 1991, and 2001 censuses.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
447
A panel dataset referring to ninety-two Italian provinces over
nine points in time from 1883 to 2013 was the result. Provinces were
standardized in terms of size and shape by aggregating territories and
administrative borders as originally set in 1955. The only exception is
the year 1883 where some provinces are missing because they were
not part of Italy (Trento, Bolzano, Trieste, and Gorizia), belonged
to different and larger provinces, or had different (larger or smaller)
boundaries that are impossible to adjust to 1955. Hence, whereas for
the remaining years there are ninety-two provinces, in 1883 only
sixty-nine are reported. The resulting dataset has an unbalanced panel
structure with 802 observations.13
Measures All variables considered are time-varying indicators
at the provincial level, although they were also measured in larger
aggregates for descriptive purposes. Most of them are proportional
to either the absolute number of deaths in the year-province
(obtained from the vital statistics registers) or the year-province pop-
ulation (measured in the census year). Putting this information
together with that collected from other registers, several indicators
were constructed.
Our dependent variable is the hospitalization of death, mea-
sured as the percentage of deaths in public or private hospitals out
of total deaths, excluding other non-strictly hospitalized welfare
facilities. Since in our data deaths in hospices can only be considered
since 2011 and nursing homes since 2004, focusing only on hospitals
guarantees comparability over time. It must therefore be noted
that this study does not directly address the emergence of other
institutions responsible for the organization of death, though in
Italy these institutions represent relatively recent and locally based
phenomena, involving a small percentage of total deaths, as seen
from descriptive results.
Because a key focus of this research is the implications of
structural factors on the displacement of death to hospital, data on
household structure changes and urbanization processes from popula-
tion censuses were collected first. The average number of household
components, computed with the ratio between the total population
and the number of families was included as an indicator of family
13 Most relevant territorial changes between 1883 and 1955 occurred in the provinces of
Rome, Genoa, and Livorno, but all indicators used in the analysis refer to relative rather than
absolute values, which attenuates the bias of territorial changes.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
448
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
size. Furthermore, to account for changes in the household structure,
three categories following the Laslett classification scheme were con-
sidered: solitaries, nuclear families, and complex families (including
either extended, multiple, indeterminate, and no families). The per-
centage of each of these categories over total families was measured
and a complex/nuclear household index was computed, accounting
for the incidence of complex families on nuclear families (multiplied
by 100). The level of urbanization was measured as a percentage of
people living in cities larger than 20,000 inhabitants. This index was
also divided by ten in the analysis, every one-unit increase meaning a
10 percent increase.14
To account for the epidemiological transition that has occurred
since the late nineteenth century and the growing importance of
long-convalescence diseases as causes of death, the malignant cancer
mortality rate (expressed in units of deaths per 1,000 individuals) and
the percentage of deaths from malignant cancer were measured
from the causes-of-death registers. It is worth noting that the cancer
mortality rate is affected by the age structure of the population, its
dynamics reflecting the process of aging over time. An indicator of
aging—the percentage of people over seventy—was also collected.
To account for the availability of medical facilities, implying the
medicalization of various aspects of social life, including the organi-
zation of death, the rate of beds in hospitals per 1,000 people was
considered. Furthermore, because the emergence of hospitals as sites
of death might be influenced by other changing attitudes associated
with the process of civilization—according to Elias’ hypothesis—
the homicide rate per 100,000 individuals was considered as one
possible indicator of this process, thus accounting for the spread of
violent deaths.15
14 For the Laslett classification scheme, see Peter Laslett and Richard Wall, Household and
Family in Past Time (Cambridge, 1972). Unfortunately, information on the household struc-
ture is only been available from the 1951 population census on, so this variable is missing in
1883. Furthermore, the only possibility of achieving comparability over the years 1951–2011 is
by aggregating extended, multiple, indeterminate, and no families, as these were in pre-1981
censuses.
15 The homicide ratio is able to account for only one component in the whole process of
civilization, leaving other important aspects aside. Causes-of-death statistics were first collected
at the provincial level for the entire Italian territory in 1887, which we used as the first ref-
erence year. The causes-of-death classification has been subjected to many changes since, but
it is possible to reconstruct the time-series of malignant cancer.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
449
Other potential determinants of site-of-death changes were
also measured. As a measure of economic growth, we collected
the added per capita value. One indicator of secularization is the
percentage of civil marriages over total marriages. This is the only
indicator of attitude toward religion available before the introduc-
tion of social surveys. As a control variable for education level, we
considered the rate of illiteracy among the population over six years
old. This is a minimum educational requirement that accounts
adequately for the educational stratification in Italy before World
War II.16
Methods The statistical analysis was designed primarily to
investigate how long-period location-of-death changes are
affected by social processes that change over time. In this frame-
work, we also aimed at observing whether the influence of these
social processes changed in different sub-periods across history. As
a secondary purpose, the analysis explored territorial variations in
the process of hospitalization of death by considering how far the
influence of the aforementioned social processes is geographically
differentiated. Given these purposes, we developed a random
intercept model allowing for different “within” and “between”
effects. The model was run both for the whole period (1883–
2013) and for different sub-periods (1883–1955, 1955–1981, and
1981–2013). For each province i and year t our model was
þ β
ð
yit ¼ α þ ζ
þ uit
2macro–areai þ β3
(cid:1)Xi∙ − xit
Þ þ β4
1yeart
Þ þ β
(cid:1)Xi∙
ð
i
where y is the percentage of deaths in hospitals, α is the constant
term, year is the observed year dummies (from 1883 to 2013) that
account for cluster-invariant time trends, macro_area is a set of
time-constant macro regional dummies, ζi is the random intercept,
uit represents time-varying unobservables, and x is a vector of
time-varying variables indicating availability of medical facilities
(expressed in hospital beds); malignant cancer mortality rate; average
household components (or, alternatively, complex/simple house-
hold index—in this case the model exclusively refers to the period
1955–2013); urbanization index; violent deaths index; seculariza-
tion index; and education index. The aging index and the added
16 According to census information, the illiteracy rate in 1881 Italy was still higher than
67%, while in 1951 it was 13%.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
450
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
per capita value were excluded from the analysis because of collin-
earity (see the Appendix). Each time-varying variable was included
as both a cluster mean and a deviation from the cluster mean to
account for between-provinces and over-time effects respectively.17
Two rationales are offered for a random-effects approach with
this kind of configuration. The first one is cluster confounding.
On one hand, our model allows us to consider to what extent
the percentage of deaths in hospitals changed according to time-
invariant differences among provinces in the observed indicators,
suggesting factors responsible for territorial variation (“between”
effects). On the other hand, it allows us to study, both for the
whole period and for specific sub-periods, how the deaths-in-
hospitals rate curve is affected by processes that change over time
(“within” effects). The two effects can potentially show a different
direction or intensity and separating them improves the substantial
interpretation of our estimates. Furthermore, although random-
effects models assume level-two exogeneity, “within” estimates
are free from bias by construction due to correlation with time-
fixed unobservables.18
The second argument is that random-effects models accom-
modate the inclusion of time-invariant characteristics. This allows
us to investigate territorial differences including macro-area
dummies in the analysis (Northwest, Northeast, Central, South,
and Islands). This aspect was further explored through specifica-
tion of models with interaction terms, designed to show how
much long-term (“within”) effects of urbanization and household
size change according to different macro-areas of Italy.
RESULTS
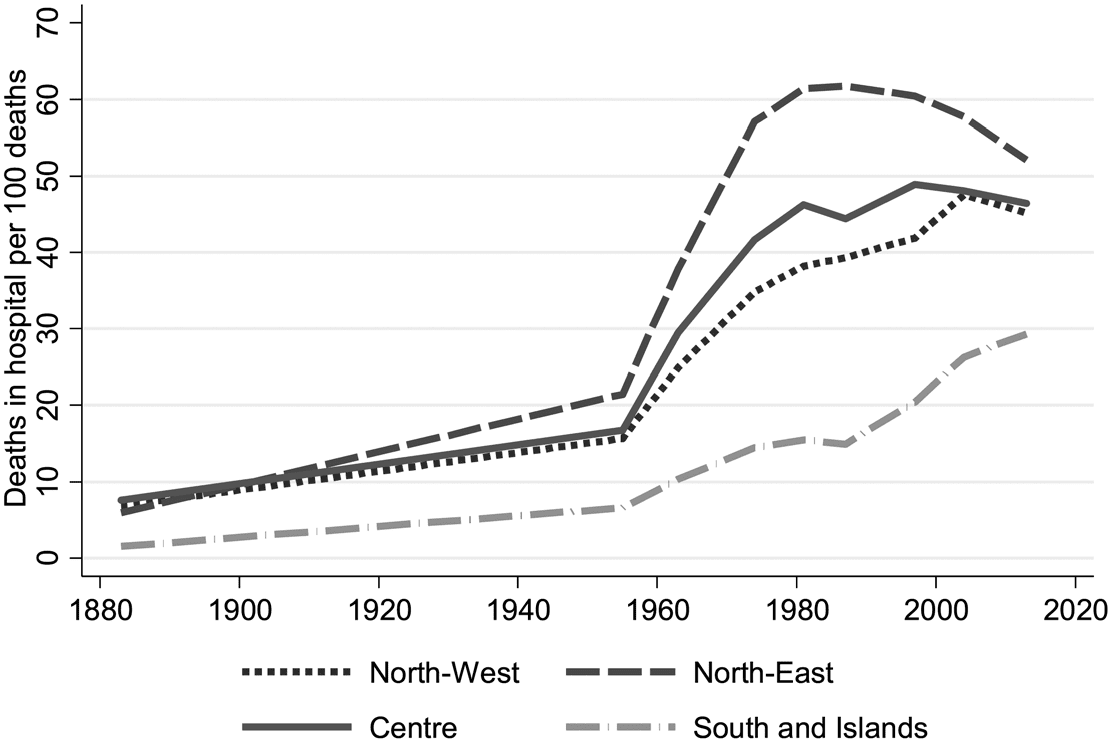
Processes Observed from 1883 to 2013 Changes in the place of
death over time have been characterized in Italy by strong territo-
rial differences (Figure 1). Between 1883 and 1981 the share of
deaths in hospitals grew faster in Northeast Italy than elsewhere
17
Sophia Rabe-Hesketh and Anders Skrondal, Multilevel and Longitudinal Modeling Using
Stata (College Station, 2012), I; John M. Neuhaus and John D. Kalbfleisch, “Between- and
Within-Cluster Covariate Effects in the Analysis of Clustered Data,” International Biometric
Society, LV (1998), 638–645.
18 For cluster confounding, see Brandon L. Bartels, “Beyond Fixed versus Random Effects:
A Framework for Improving the Substantive and Statistical Analysis of Panel, Time-Series
Cross-Sectional, and Multilevel Data,” Society for Political Methodology (2009).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
451
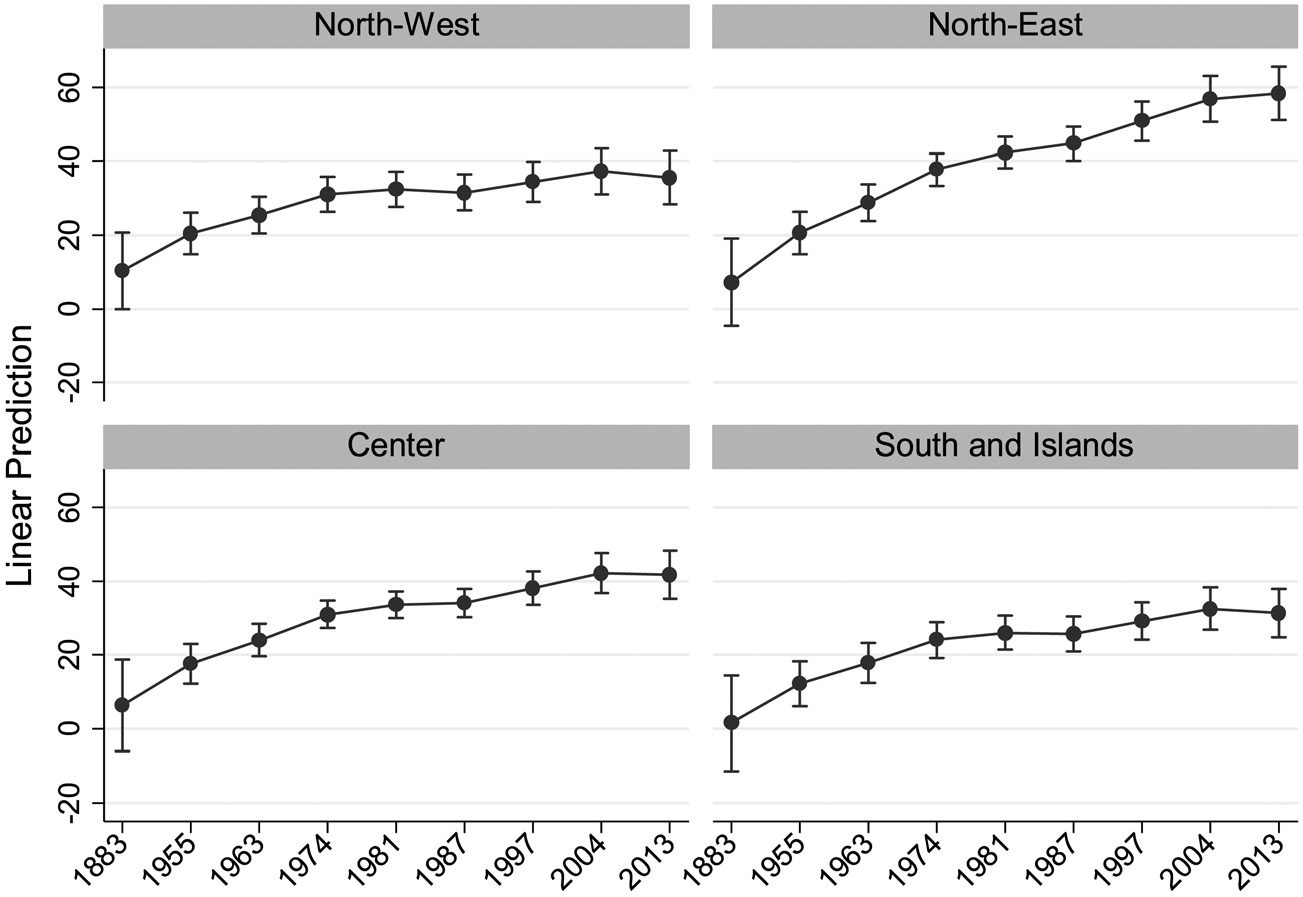
Fig. 1 Percentage of Hospital Deaths Observed for Different Macro-
Areas of Italy, 1883–2013
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
(especially after the 1950s). Since the 1980s it has stabilized and has
even decreased in recent years. The same pattern, at lower growth
rates, is also seen in Northwest and Central Italy. In southern
provinces the percentage of deaths in hospitals had even lower
levels of growth, though the deaths were more homogeneous over
the whole period and only reached 30 percent in 2013.
Importantly, in the last years observed (2004 and 2013), cen-
tral and northern areas show a slightly decreasing trend. This is
partly explained by the growing relative incidence of nursing
homes and hospices as sites of death in the period 2004 to 2013.
The emergence of these institutions was much more marked in
the central and northern regions than in the southern ones, though
only accounting for about 10 percent of deaths in 2013 for the
whole territory.
Table 1 provides a concise descriptive overview of processes
observed throughout the 130-year period considered, showing
values at the national level for all of our collected variables.
Different and interrelated macro-dimensions emerge, potentially
associated with the hospitalization of death. The former entails
demographical and epidemiological change. Crude mortality rates
are observed to decline sharply between 1883 and 1955 due to
major medical innovations and to stabilize from the 1950s on,
1
.
0
4
1
.
7
3
6
.
7
3
3
.
4
3
5
.
3
2
9
.
3
1
6
.
4
3
1
0
2
4
0
0
2
7
9
9
1
7
8
9
1
1
8
9
1
4
7
9
1
3
6
9
1
5
5
9
1
3
8
8
1
3
1
0
2
–
3
8
8
1
,
l
e
v
e
L
l
a
n
o
i
t
a
N
e
h
t
t
a
s
e
u
l
a
V
d
e
v
r
e
s
b
O
1
e
l
b
a
T
3
.
5
2
.
6
8
.
3
6
.
1
4
6
.
2
0
.
0
1
5
.
5
2
5
.
5
1
4
.
2
2
.
1
3
5
.
0
6
4
.
8
9
.
2
4
4
.
4
1
.
4
6
.
9
5
.
2
6
.
6
2
3
.
3
1
6
.
2
9
.
4
2
6
.
6
6
5
.
8
9
.
5
9
.
9
4
.
2
4
.
4
2
7
.
1
1
7
.
2
8
.
2
2
1
.
7
6
1
.
0
1
7
.
7
4
.
9
3
.
2
4
.
9
9
.
2
4
.
4
2
5
.
9
1
0
.
9
6
5
.
1
1
3
.
9
3
.
9
0
.
2
6
.
8
0
.
3
9
.
1
2
3
.
8
1
4
.
0
7
2
.
1
1
9
.
3
1
2
.
2
5
8
.
0
5
.
2
4
1
.
1
3
.
4
4
8
.
2
1
1
.
2
5
9
.
0
6
.
1
3
5
.
1
4
.
6
3
0
.
5
1
0
.
2
5
2
.
1
8
.
0
2
9
.
1
9
.
9
2
7
.
6
1
5
.
2
5
6
.
1
5
.
4
1
8
.
2
7
.
5
1
9
.
5
1
0
.
3
5
9
.
1
7
.
2
1
4
.
3
9
.
7
0
0
1
0
0
1
0
0
1
0
0
1
0
0
1
8
.
0
1
9
.
9
8
.
1
5
.
8
1
1
.
7
4
.
3
5
.
3
1
6
.
9
6
9
.
6
1
3
.
4
2
3
.
2
5
0
0
1
1
.
1
1
.
8
7
.
5
3
.
1
7
.
9
8
.
9
5
.
1
1
.
6
6
.
3
2
.
5
1
5
.
1
1
1
.
9
6
4
.
9
1
0
.
8
2
6
.
7
4
0
0
1
9
.
0
3
.
1
9
.
8
5
.
0
1
.
8
6
.
0
1
2
.
1
5
.
1
1
0
.
5
0
.
4
6
.
0
1
0
.
7
6
4
.
2
2
5
.
3
3
7
.
1
4
5
.
1
2
.
2
2
.
0
5
.
3
1
0
0
1
0
.
2
4
.
7
2
4
.
0
6
.
1
1
.
3
6
.
4
4
.
5
7
.
2
3
.
1
2
4
.
0
0
.
4
6
s
h
t
a
e
d
e
m
o
h
s
h
t
a
e
d
s
h
t
a
e
d
l
a
t
i
p
s
o
h
e
c
i
p
s
o
h
g
n
i
s
r
u
n
f
o
f
o
f
o
e
g
a
t
n
e
c
r
e
P
e
g
a
t
n
e
c
r
e
P
e
g
a
t
n
e
c
r
e
P
e
l
p
o
e
p
0
0
0
,
1
r
e
p
s
d
e
b
l
a
t
i
p
s
o
H
e
t
a
r
y
t
i
l
a
t
r
o
M
s
h
t
a
e
d
r
e
c
n
a
c
t
n
a
n
g
i
l
a
m
s
0
7
–
r
e
v
o
f
o
f
o
e
g
a
t
n
e
c
r
e
P
e
g
a
t
n
e
c
r
e
P
e
t
a
r
y
t
i
l
a
t
r
o
m
r
e
c
n
a
c
t
n
a
n
g
i
l
a
M
f
o
)
s
e
i
l
i
m
a
f
l
a
t
o
t
r
e
v
o
(
e
g
a
t
n
e
c
r
e
P
s
t
n
e
n
o
p
m
o
c
l
d
o
h
e
s
u
o
h
e
g
a
r
e
v
A
s
e
i
l
i
m
a
f
x
e
l
p
m
o
c
s
e
i
l
i
m
a
f
e
l
p
m
i
s
s
e
i
r
a
t
i
l
o
s
l
a
t
o
T
.
b
a
h
n
i
0
0
0
,
0
2
>
s
e
i
t
i
c
n
i
g
n
i
v
i
l
e
g
a
t
n
e
c
r
e
P
x
e
d
n
i
l
d
o
h
e
s
u
o
h
e
l
p
m
i
s
/
x
e
l
p
m
o
C
e
l
p
o
e
p
0
0
0
,
0
0
1
r
e
p
s
r
e
d
r
u
M
)
s
d
n
a
s
u
o
h
t
(
e
u
l
a
v
a
t
i
p
a
c
s
e
g
a
i
r
r
a
m
l
i
v
i
c
a
s
e
t
a
r
e
t
i
l
l
i
f
o
f
o
e
g
a
t
n
e
c
r
e
P
e
g
a
t
n
e
c
r
e
P
r
e
p
d
e
d
d
A
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
.
g
n
i
s
s
i
m
e
r
a
r
o
t
a
c
i
d
n
i
s
i
h
t
r
o
f
s
e
u
l
a
v
l
e
t
u
o
s
b
a
e
r
e
h
w
,
s
e
t
a
m
i
t
s
e
n
a
e
m
l
e
v
e
l
–
e
c
n
i
v
o
r
P
a
D I S PL A C E M E NT O F D E A T H |
453
with few territorial differences. In the meantime, the Italian pop-
ulation has continued to age. These processes imply a changing
causes-of-death composition throughout the period, with the
declining prominence of infectious diseases and observed increas-
ing rates of deaths from malignant cancer (approaching 25 percent
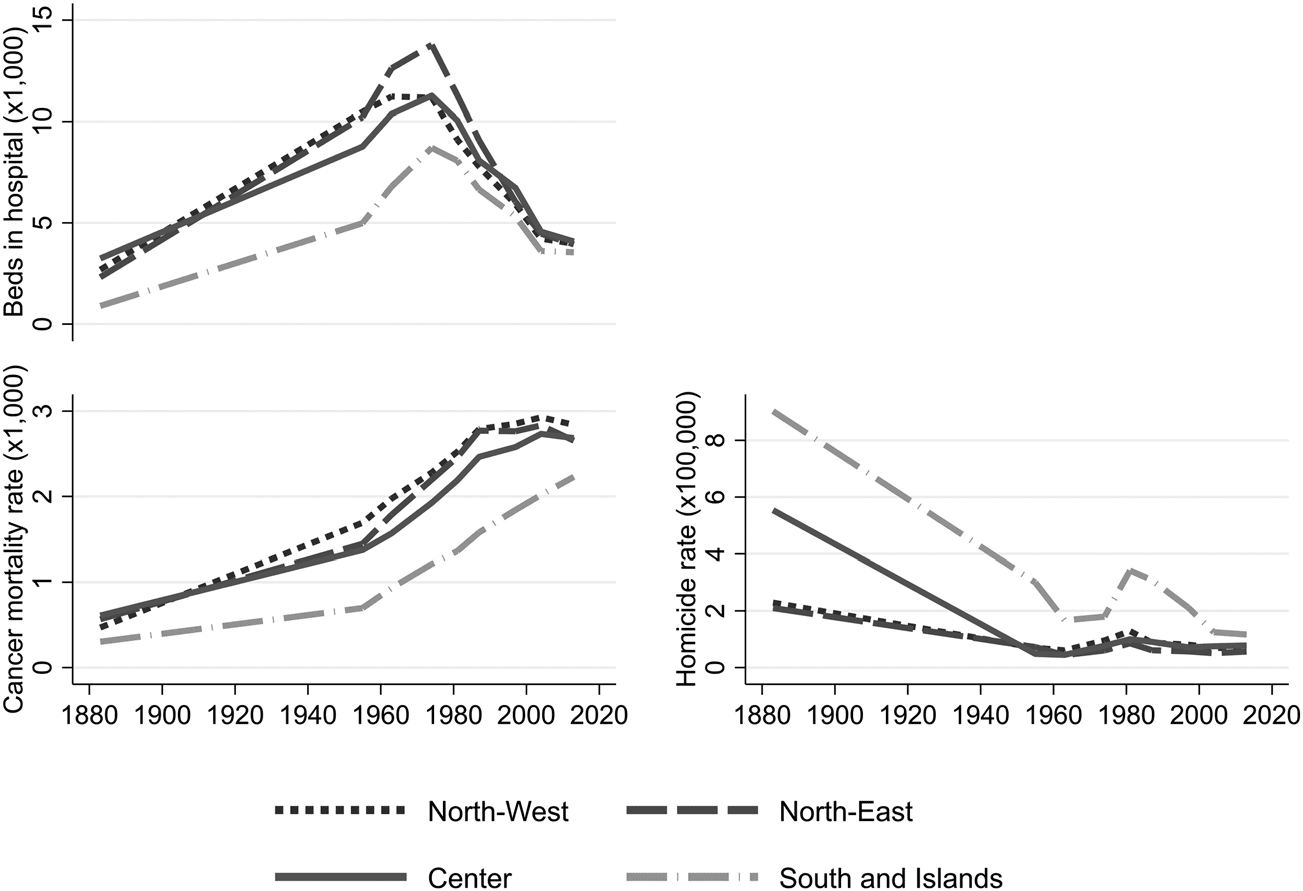
in 2013, and higher in the North). In this context, the availability
of medical facilities has followed a reverse-U-shape trend. The
number of hospital beds, which reflects the reception capacity of
hospitals (always larger in the North), reached its peak in the 1970s
and later decreased.19
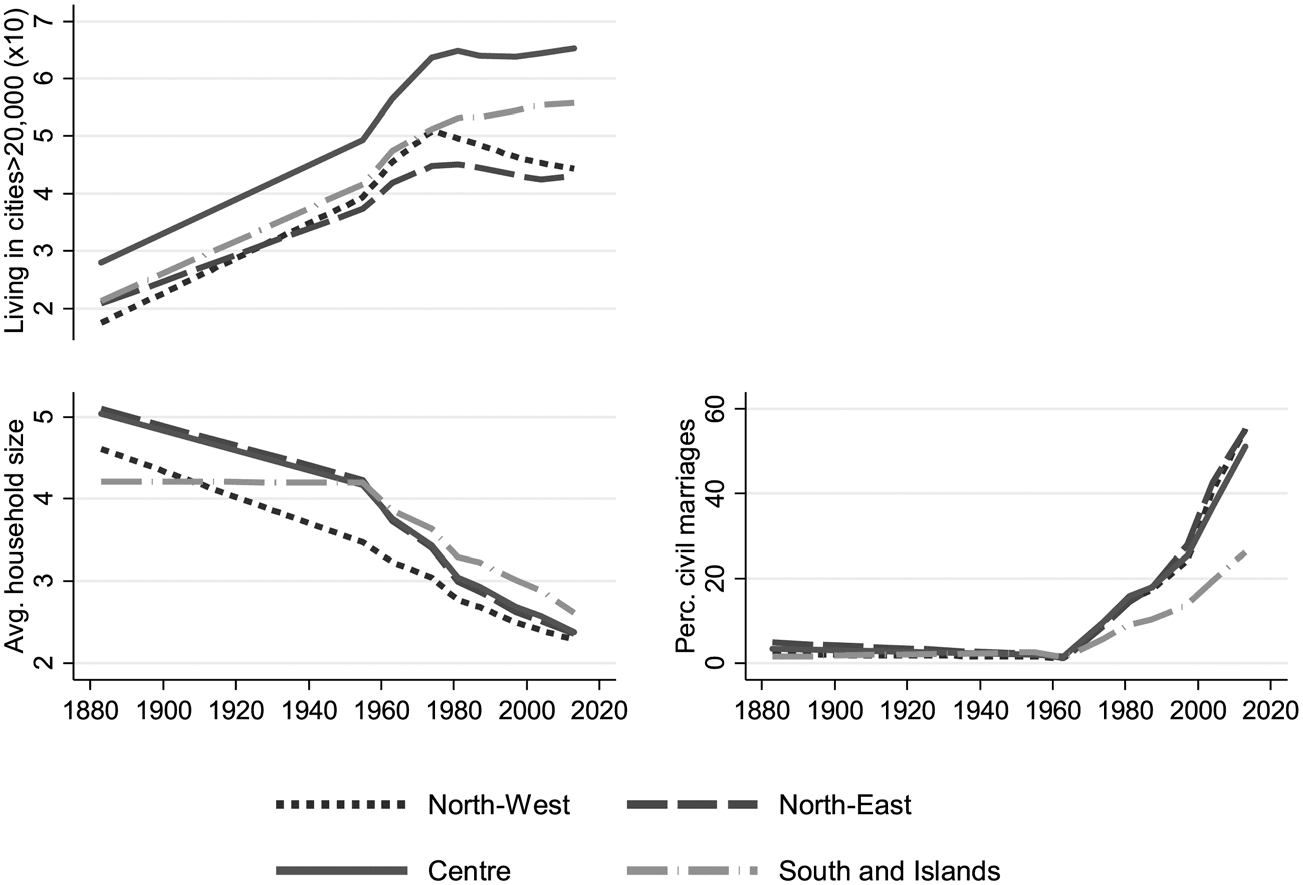
A second aspect regards family dynamics in the demographic
transition. The average household size markedly and continuously
decreased throughout the whole period observed, reaching about
2.5 components in 2013. In 1883 slightly higher average compo-
nents were observed in the north-central regions than in southern
Italy (Figure 4). Other changes in the household structure for the
period 1955–2013 also appear geographically differentiated. Com-
plex households (meaning extended, multiple, and no family) are
observed to lower their incidence rapidly over time (mainly due to
industrialization and urbanization processes). The percentage of
complex households observed in 1955 and 1981 is substantially
higher in north-central Italy than in the South. In particular, var-
iations over time of the complex/nuclear household index by
macro-area show that the central and northeastern regions at the
beginning of the period were characterized by a much larger rela-
tive importance of complex families (Figure 2). In later years, Cen-
tral and Northeast Italy experienced the sharpest decline in family
systems based on multiple and extended households. In fact, in
these areas (and particularly in Northeast Italy) industrialization
implied a radical change in residential patterns of farming house-
holds that had remained much more stable in previous centuries.
By contrast, the Northwest, characterized by great urban centers,
and the South, where salaried workers in agriculture were more
common, in the 1950s appeared much less dominated by complex
19 For causes-of-death changes between the nineteenth and twentieth centuries in Italy, see
Lucia Pozzi, La Lotta per la Vita: Evoluzione e Geografia della Sopravvivenza in Italia fra ‘800 e ‘900
(Udine, 2001); idem, “La Mortalità per Cause nelle Province Italiane dal 1890 al 1950: Differ-
enziazioni Geografiche e Fattori Esplicativi,” unpub. Ph.D. thesis, (Università di Firenze–
Padova–Roma, 1990).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
454
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
Fig. 2 Complex/Nuclear Household Index Observed for Different
Macro-Areas of Italy, 1955–2013
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
household structures than by nuclear ones. Thus, in these areas (and
especially in the South) the relative decrease in multiple and
extended household structures was significantly less pronounced.20
The number of people living in large urban centers grew con-
siderably in number up to the 1980s, especially between the end of
the nineteenth century and the 1950s, with lower levels observed
in the Northeast, where big cities are less common (Figure 4). The
emergence of civil marriages, starting from the 1960s, was partic-
ularly strong in the last years observed, with large differences
between central/northern and southern areas. The homicide rate,
which decreased in the post-war period, grew faster during the
1970s and 1980s, but subsequently declined even in the South
(where the highest levels are observed, Figure 3). Finally, due to
the emergence of mass educational programs, there was a sharp
decrease in the illiteracy rate (Table 1), especially in the first half
of the twentieth century. Thereafter, variations in this indicator are
much less marked.
20 Marzio Barbagli, Sotto lo Stesso Tetto: Mutamenti della Famiglia in Italia dal XV al XX Secolo
(Bologna, 1984); idem and David Kerzer, Storia della Famiglia Italiana (Bologna, 1992).
D I S PL A C E M E NT O F D E A T H |
455
Fig. 3 Beds in Hospitals (per 1,000 Inhabitants), Cancer Death Rate,
and Homicide Rate Observed for Different Macro-Areas of
Italy, 1883–2013
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
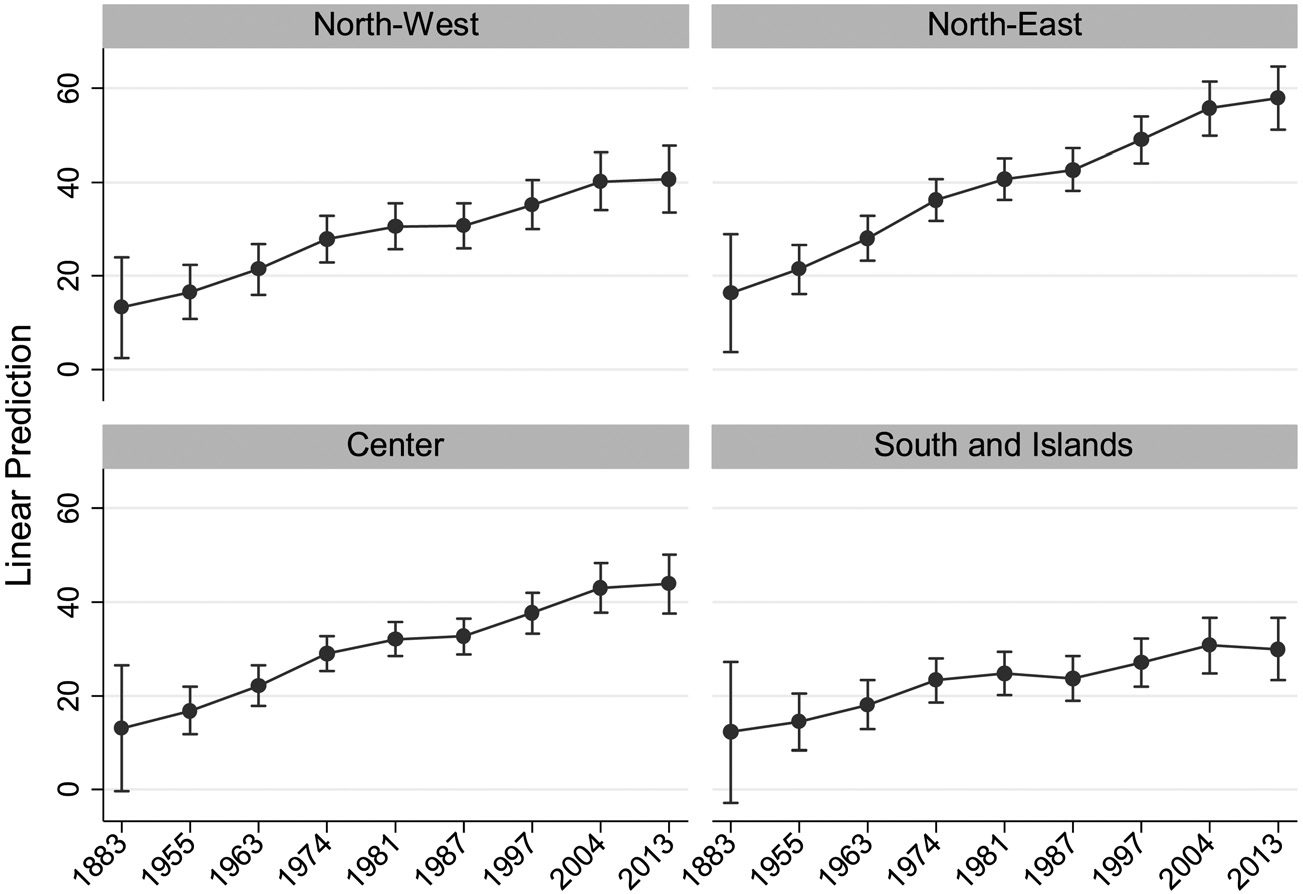
Multivariate Analysis Table 2 shows the results of three models.
Model 1 reports only time trends and macro-area dummies; model 2
considers other additional variables; model 3 includes our indica-
tor of household structure instead of the average household com-
ponents and thus exclusively refers to the period 1955–2013.
Comparing year and macro-area estimates between models 1
and 2 reveals that territorial differences and time-trend variations
reduce considerably when the other variables are included in the
analysis, although they are not completely eliminated. Differences
in the hospitalization rates between Central (reference category),
Northeast, and South Italy persist, as well as time-trend effects.
However, our covariates partially help to explain territorial time
invariant differences and common dynamic changes over time.
Model 2 provides an overview of aspects associated with
place-of-death changes in the period 1883–2013. Figures 1–4
can help the broad interpretation of unitary changes in the indica-
tors included. Only the availability of medical facilities and the sec-
ularization index show significant (and positive) “between” effects
on the hospitalization rate. It means that these two aspects partially
)
3
(
l
e
d
o
M
)
2
(
l
e
d
o
M
)
1
(
l
e
d
o
M
d
n
a
”
n
e
e
w
t
e
B
“
t
n
e
r
e
f
f
i
D
r
o
f
i
g
n
w
o
l
l
A
,
s
h
t
a
e
D
l
a
t
i
p
s
o
H
f
o
e
g
a
t
n
e
c
r
e
P
e
h
t
n
o
s
e
t
a
m
i
t
s
E
l
e
d
o
M
t
p
e
c
r
e
t
n
I
s
t
c
e
f
f
E
”
n
i
h
t
i
W
m
o
d
n
a
R
“
)
8
1
.
1
(
)
9
8
.
1
(
)
8
5
.
2
(
)
4
9
.
2
(
)
3
4
.
3
(
)
6
0
.
4
(
)
5
5
.
4
(
)
7
8
.
2
(
)
0
4
.
2
(
)
1
4
.
3
(
)
1
4
.
0
(
)
3
1
.
0
(
)
0
4
.
3
(
)
2
4
.
1
(
.
f
e
r
c
5
9
.
4
c
0
4
.
1
1
c
1
1
.
2
1
c
2
2
.
3
1
c
8
8
.
8
1
c
4
4
.
4
2
c
2
3
.
6
2
.
f
e
r
4
4
.
1
c
3
0
.
2
1
a
8
0
.
8
−
b
6
1
.
1
c
4
7
.
0
c
7
7
.
7
3
5
.
6
−
)
1
9
.
3
(
)
6
2
.
1
(
)
3
8
.
1
(
)
9
3
.
2
(
)
3
7
.
2
(
)
8
1
.
3
(
)
3
7
.
3
(
)
3
2
.
4
(
)
6
4
.
2
(
)
8
1
.
2
(
)
4
1
.
3
(
)
0
4
.
0
(
)
3
1
.
0
(
)
2
9
.
3
(
)
9
4
.
1
(
)
3
4
.
4
(
)
4
4
.
1
(
a
0
2
.
3
c
5
5
.
7
b
2
2
.
7
a
9
1
.
6
a
0
8
.
7
b
7
6
.
9
.
f
e
r
8
9
.
4
−
7
6
.
6
.
f
e
r
0
9
.
1
−
c
0
5
.
8
a
9
1
.
7
−
a
0
0
.
1
a
2
3
.
0
c
4
6
.
6
1
9
.
1
−
4
6
.
3
c
0
4
.
7
−
)
3
2
.
1
(
)
3
1
.
1
(
)
3
1
.
1
(
)
3
1
.
1
(
)
3
1
.
1
(
)
3
1
.
1
(
)
3
1
.
1
(
)
3
1
.
1
(
)
6
4
.
2
(
)
6
4
.
2
(
)
1
2
.
2
(
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
c
6
6
.
7
−
.
f
e
r
c
3
5
.
8
c
6
3
.
8
1
c
7
8
.
1
2
c
2
6
.
2
2
c
9
1
.
6
2
c
3
9
.
9
2
c
7
9
.
8
2
1
8
.
0
−
c
7
9
.
3
1
c
9
6
.
7
1
−
.
f
e
r
s
e
i
t
i
l
i
c
a
f
l
a
c
i
d
e
m
f
o
y
t
i
l
i
b
a
l
i
a
v
A
s
d
n
a
l
s
I
d
n
a
h
t
u
o
S
a
e
r
a
–
o
r
c
a
M
t
s
e
w
h
t
r
o
N
t
s
a
e
h
t
r
o
N
l
a
r
t
n
e
C
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
e
g
n
a
h
c
s
l
a
t
i
p
s
o
h
s
l
a
t
i
p
s
o
h
n
i
n
i
s
d
e
B
s
d
e
B
l
l
a
c
i
g
o
o
m
e
d
i
i
p
E
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
s
t
n
e
n
o
p
m
o
c
s
t
n
e
n
o
p
m
o
c
e
z
i
s
l
d
o
h
e
s
u
o
H
l
d
o
h
e
s
u
o
h
l
d
o
h
e
s
u
o
h
.
g
v
A
.
g
v
A
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
e
t
a
r
e
t
a
r
h
t
a
e
d
h
t
a
e
d
r
e
c
n
a
C
r
e
c
n
a
C
2
e
l
b
a
T
r
a
e
Y
5
5
9
1
3
8
8
1
3
6
9
1
4
7
9
1
1
8
9
1
7
8
9
1
7
9
9
1
4
0
0
2
3
1
0
2
)
5
1
.
0
(
)
6
0
.
0
(
)
6
4
.
0
(
)
0
7
.
0
(
)
3
7
.
0
(
)
3
2
.
0
(
)
3
2
.
0
(
)
6
0
.
0
(
)
6
2
.
0
(
)
1
1
.
0
(
a
9
2
.
0
c
1
4
.
0
−
c
7
2
.
3
5
6
.
0
5
0
.
0
2
9
.
0
−
c
4
1
.
1
b
8
1
.
0
−
c
3
8
.
0
0
3
.
0
4
2
.
6
0
0
.
6
2
5
.
0
2
9
6
3
7
)
2
4
.
0
(
)
7
5
.
0
(
)
7
6
.
0
(
)
4
2
.
0
(
)
1
2
.
0
(
)
5
0
.
0
(
)
3
2
.
0
(
)
6
0
.
0
(
c
3
1
.
2
0
4
.
0
4
9
.
0
−
8
2
.
0
−
c
7
0
.
1
7
0
.
0
c
4
2
.
0
5
1
.
0
−
1
7
.
5
2
9
.
6
1
4
.
0
2
9
5
0
8
2
3
.
7
0
7
.
7
8
4
.
0
2
9
5
0
8
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
x
e
d
n
i
x
e
d
n
i
.
e
s
u
o
h
.
e
s
u
o
h
.
p
m
i
s
/
x
e
l
p
m
o
C
.
p
m
i
s
/
x
e
l
p
m
o
C
e
r
u
t
c
u
r
t
s
l
d
o
h
e
s
u
o
H
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
0
0
0
,
0
2
>
s
e
i
t
i
c
0
0
0
,
0
2
>
s
e
i
t
i
c
n
i
n
i
g
n
i
v
i
L
g
n
i
v
i
L
s
h
t
a
e
d
t
n
e
l
o
i
v
f
o
d
a
e
r
p
S
x
e
d
n
i
n
o
i
t
a
z
i
n
a
b
r
U
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
s
e
g
a
i
r
r
a
m
s
e
g
a
i
r
r
a
m
l
i
v
i
C
l
i
v
i
C
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
s
r
e
d
r
u
M
s
r
e
d
r
u
M
x
e
d
n
i
n
o
i
t
a
z
i
r
a
l
u
c
e
S
)
n
e
e
w
t
e
b
(
i
)
n
h
t
i
w
(
s
e
t
a
r
e
t
i
l
l
I
s
e
t
a
r
e
t
i
l
l
I
n
o
i
t
a
c
u
d
E
s
n
o
i
t
a
v
r
e
s
b
O
s
r
e
t
s
u
l
c
f
o
N
u
_
a
m
g
i
s
e
_
a
m
g
i
s
o
h
r
.
s
e
s
e
h
t
n
e
r
a
p
n
i
s
r
o
r
r
e
d
r
a
d
n
a
t
S
.
5
0
.
0
<
p
a
.
1
0
.
0
<
p
b
.
1
0
0
.
0
<
p
c
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
458
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
explain territorial differences, even when standardized by macro-
area fixed effects; provinces (within macro-areas) with higher
availability of beds in hospitals and higher levels of secularization
also experience higher levels of hospitalized deaths.21
Conversely, many aspects are associated with changes in the
percentage of deaths in hospitals (“within” effects). First, a growth
in the availability of medical facilities increases the number of
deaths in hospitals. Second, changes in the prevalence of deaths
from cancer (an outcome associated with aging) positively and siz-
ably affect the hospitalization rate curve.
Controlling for these aspects, the indicators of household size
and urbanization have a substantial impact. The decrease in aver-
age family components over time (observed in this period) implies
a marked growth in the hospitalization of death, amounting to 7.4
percent per component. Over the years 1883–2013 the household
size reduced by 2.6 members in the north-central regions and by
1.6 in the southern ones (Figure 4). Furthermore, the increasing
urbanization, which changed by about three points over the
period, positively affects the percentage of deaths in hospitals.
Finally, there are small “within” effects of other variables.
Changes in the number of murders are not significant, whereas
the secularization index has no effects as a long-term process, since,
in comparing model 2 to model 3, these numbers turn out to be
negative. The fact is that the growth of civil marriages is concen-
trated in the last year observed, when the hospitalization rate had
already declined in some provinces.
The results of model 3 mostly confirm the findings for the
period 1955–2013. Additionally, a marked household structure
effect emerges. As complex household structures decrease through
time compared to simple ones, a growth in the percentage of
deaths in hospitals becomes evident. Note that the complex/
simple household index is smaller in the period by about thirty-
five points in the Northeast and ten points in the South and Islands
(Figure 2). These changes imply a +14.4 and +4.1 variation
respectively on the percentage of deaths in hospitals, keeping all
21 We also ran models without macro-area fixed effects. Results confirmed that beds in
hospitals and civil marriages exclusively have significant “between” effects, although estimates
are even larger (results are not shown, but available upon request). They confirm that these
aspects are party responsible for territorial differences, including north-south variation.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
459
Fig. 4 Urbanization Index (per 10 inhabitants), Average Household
Components, and Percentage of Civil Marriages Observed for
Different Macro-Areas of Italy, 1883–2013
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
the other variables fixed. Furthermore, this indicator shows
diverging “between” and “within” effects. On average over the
whole period, higher levels of complex families are observed
among provinces with the largest percentage of deaths in hospitals,
which subsequently experienced the sharpest decrease in such
facilities.
To observe differentiated influences of covariates over time,
we estimated our model for three sub-periods, 1883–1955,
1955–1981, and 1981–2013. Results, shown only for “within”
estimates (Table 3), suggest several insights. First, the increase of
beds in hospitals has continuously contributed to increasing the
rate of death in hospitals. Among the other aspects, between
1883 and 1955, only radical changes in urbanization, which in this
period have grown more strongly than ever, have affected the slow
increase of the death-in-hospital rate curve. Although statistically
significant, the effect of secularization in this period is substantially
limited. Subsequently, the largest increase of deaths in hospitals
occurred between 1955 and 1981, while other factors, such as
460
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
Table 3
“Within” Effects Estimates of Random Intercept Models on the
Percentage of Hospital Deaths for Different Periods
1883–1955
1955–1981
1981–2013
0.45c
Beds in hospitals
−1.96
Cancer death rate
Avg. household components −2.04
Complex/simp. house. index
Living in cities>20,000
Murders
Civil marriages
Illiterates
1.25b
−0.34
−0.46a
0.00
Standard errors in parentheses.
ap<0.05.
bp<0.01.
cp<0.001.
1.07c
(0.14)
(2.44) −4.21
(1.72)
−0.72c
0.9
0.45
0.31b
0.93c
(0.45)
(0.27)
(0.19)
(0.06)
(0.18)
(2.18)
0.72b
6.67b
(0.24)
(2.41)
(0.09) −0.41b
2.23
(0.83)
(0.36)
0.07
(0.12) −0.04
(0.13) −1.88c
(0.15)
(1.47)
(0.28)
(0.09)
(0.51)
the decrease of complex households and the emergence of civil
marriages were affecting the rate of growth. Whereas changes in
the household structure between 1981 and 2013 have maintained
their influence, variation in the cancer death rate affected the per-
centage of deaths in hospitals. It is likely that this aspect is mostly
responsible for the growth observed in southern provinces,
whereas the growth of cancer deaths stabilized in the north-central
regions (as observed for the hospitalization-of-death curve).
In the models presented, all the variables express mean effects
derived from the population of the whole province. The follow-
ing analysis aims to study whether changes in some variables over
time are clustered within different macro-areas of Italy.
Specifically, we included interaction terms between macro-area
dummies and the “within” coefficient of household size and
urbanization index respectively (for complete estimates see the
Appendix, Table A.4).
Predicted rates of deaths in hospitals in different years were
estimated from models with interactions, keeping other variables
at their mean values (Figures 5 and 6). We assumed a constant
decrease in the average household components over time, ranging
from 1.2 household size mean deviation in 1883 to −1.2 in 2013,
while also assuming that the urbanization index would vary by a
yearly increase from 1.6 to −1.6. Though arbitrary, these figures
reflect observed ranges of the household size and urbanization
index over the whole period.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
461
Fig. 5 Predictions of Hospitalization Rates in Different Macro-Areas of
Italy, Considering a Constant Yearly Decrease in Household
Size Mean Deviation, Ranging from 1.2 to −1.2, 1883–2013
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Sizable territorial differences emerge in our estimates (Figure 5).
In the first years of the process, assuming a positive mean deviation
in household size (hence an effect above the mean for the whole
period), few differences are observable among macro-areas. How-
ever, as time marches on and the household sizes reduce in later
years, the percentage of deaths in hospitals grows at a faster rate in
northeastern provinces than anywhere else, reaching the highest
levels. The same decrease in household size is less marked in the
northwestern and central provinces, producing lower hospitaliza-
tion rates. In the South the decrease in family size has no effect and
the small growth in the percentage of deaths in hospitals is due
only to a gradual increase over time.
Similar aspects emerge from estimates that assume changes in
the urbanization index (Figure 6). Dynamics are comparable in
Northwest, Central, South Italy, and the Islands. However, in the
Northeast the change in urbanization produces significantly higher
hospitalization rates.
These results confirm the peculiarity of the Northeast, which is
observed to experience a pattern of household structure simplification
462
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
Fig. 6 Predictions of Hospitalization Rates in Different Macro-Areas of
Italy, Considering a Constant Yearly Increase in the Urbanization
Index Mean Deviation, Ranging from −1.6 to 1.6, 1883–2013
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
unlike any other territory. There the reduction in household com-
ponents and the process of urbanization (strictly affected by indus-
trialization) implies an additional effect on the dynamics beyond
the hospitalization of death.
In the nineteenth century, in Italy and around the world, people
commonly died at home. This pattern underwent a radical change
in the 1950s. The percentage of deaths in hospitals rose from less
than 10 percent at the end of the nineteenth century to 30 percent
in 2013 in the South and Islands, and before the turn of the
twenty-first century reached around 50 percent in the Northwest
and Central Italy and more than 60 percent in the Northeast.
Changes in the use of hospitals, in the organization of health facil-
ities, in medicine, and in the causes of death have driven and
shaped the rise of the number of deaths in hospitals. The institu-
tionalization hypothesis developed in the 1960s and 1970s by
Parsons and his colleagues, and later by Blauner, accounts for all
of these factors. The availability of beds in hospitals is also observed
to affect territorial differences in Italy. This aspect also lies at the
D I S PL A C E M E NT O F D E A T H |
463
core of the recent wave of cross-sectional studies. But, even con-
sidering all these changes, there remain some unexplained varia-
tions. The multivariate analysis suggests that the two factors mostly
at work were changes in household structure and the rising level of
urbanization.
On one hand, nuclear households span no more than two
generations, typically a couple with children. As lives progress
within this kind of structure, younger generations are less likely
to take care of elderly family members. On the other hand, com-
plex families are characterized by the coexistence of two genera-
tions with relatives, or three generations, under the same roof. It is
more common in this situation for elderly people to receive care
from adult sons and daughters (or sons- and daughters-in-law), or
even grandchildren. Patrilocal practices bring together both elderly
people and adult caregivers. Hence, if the ratio of nuclear families
over complex families rises or the average household size shrinks
over time, the quota of deaths in hospitals will rise, other factors
being equal.
Furthermore, social networks (including families) are not
evenly distributed among different geographical areas. The possi-
bility of receiving help from friends, neighbors, and relatives is
higher in the countryside than in towns, and in towns more likely
than in cities. According to Putnam, city size is one of the most
important variables in social capital distribution. All forms of
altruism are more common in small towns than in big cities.
The analysis shows that, other things being equal, growth in
the level of urbanization increases the proportion of people dying
in hospitals rather than at home. The literature relates this corre-
lation to two mechanisms. First, the number of people working far
from home is higher in urban than in rural settings, where more
people work in the primary sector. Second, female participation in
the labor market increases with the move from rural to urban
settings.22
The “forbidden death” theory claims that the rise of a new
attitude toward death—including the hospitalization of death—is
the effect of three independent processes, namely changes in
household structure, urbanization, and secularization. While the
22 For the territorial distribution of social capital, see Robert D. Putnam, Bowling Alone: The
Collapse and Revival of American Community (New York, 2000).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
464
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
first two factors are certainly at work, there is no evidence of
effects by the third. We only found a relatively small “between”
effect by secularization, whereas no long-term changes were found
regarding this process.
We found no evidence of the factors considered by Elias’ the-
ory of the “civilization process.” It may well be that violent deaths
had mostly declined before the historical period that we consid-
ered and caused other attitudes toward death, but we observed
no implications on the process of hospitalization.
Analysis of the Italian case suggests that the effects of urbani-
zation and family change on the rate of displacement of death from
home to hospital vary within the country. The shift is most easily
seen in Northeast Italy. This area was historically characterized by a
higher percentage of couples following the patrilocal practice after
marriage, by a larger presence of multiple and extended families,
and by bigger household sizes. Household structures changed more
rapidly, falling faster than in any other part of the country. Some
other factor triggered by this process, and connected with the speed
and depth of change, must be at work.23
This study is limited due to the characteristics of administra-
tive data and the discontinuity of the time series, but the results
achieved suggest that more research would be welcome, especially
on other countries where data are available. But it also suggests
that we need to refine the theoretical framework in order better
to understand a centuries-old historical process that owes much to
technological and scientific progress, but which is also based on
long-term social and cultural changes.
23 Arnaldo Bagnasco, Tre Italie: La Problematica Territoriale dello Sviluppo Italiano (Bologna,
1977), 198–199; Barbagli and Chiara Saraceno, Lo Stato delle Famiglie in Italia (Bologna, 1997).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
465
APPENDIX: DIAGNOSTICS & ESTIMATES OF
INTERACTION TERMS
DIAGNOSTICS To check for the assumption of no perfect collinearity, the
variance-inflation factor (VIF) was computed for all our independent variables.
Results are shown in Table A1. The tolerance for the variable “percentage of
over-70 people” (our indicator of aging) is below 0.1, and for the “added per
capita value,” it is borderline. Hence, these variables were removed from the
analysis, to avoid multicollinearity problems. As already mentioned, the
“malignant cancer mortality rate” variable, which likewise reflects the aging
structure of the population, can produce collinearity. Estimates for regression
models that include the “added per capita value” were not statistically signif-
icant (results not shown, but available upon request). Results of the VIF
values for only the variables included in the models are shown in Table A2.
Notice that the assumption of no multicollinearity holds.
To test for the normal distribution of the residuals, the standardized
residuals for the first level are plotted in Figure A1 and for the second
level in Figure A2. The plots appear normal and without outliers (std.
res.<4). Therefore, the homoskedasticity assumption holds.
A TEST ON DIFFERENT BETWEEN–WITHIN ESTIMATES
Since random
intercept models presented in the multivariate analysis allow for different
“between” and “within” effects, we performed a statistical test on equal
“between” and “within” estimates. The global test on jointly equal coef-
ficients can be considered as equivalent to the Hausman test. See Sophia
Rabe-Hesketh and Anders Skrondal, Multilevel and Longitudinal Modeling
Using Stata. I. Continuous Responses (College Station, 2012).
Table A1
VIF for All Independent Variables
VARIABLE
Hospital beds
Malignant-cancer death rate
Average household size
Percentage of over-70s
Living in cities >20,000
Murders per 100,000
Percentage of civil marriages
Percentage of illiterates
Added per capita value
Mean VIF
VIF
2.39
7.18
7.00
10.51
1.25
1.17
7.27
3.01
9.58
5.48
VIF-SQRT
TOLERANCE
1.54
2.68
2.65
3.24
1.12
1.08
2.7
1.73
3.09
0.419
0.139
0.143
0.095
0.803
0.856
0.138
0.332
0.104
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
466
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
Table A2
VIF Values for the Variables Included in the Models
VARIABLE
Hospital beds
Malignant-cancer death rate
Average household size
Living in cities >20,000
Murders per 100,000
Percentage of civil marriages
Percentage of illiterates
Mean VIF
VIF
1.89
5.84
5.52
1.16
1.16
3.10
2.92
3.08
VIF-SQRT
TOLERANCE
1.38
2.42
2.35
1.08
1.08
1.76
1.71
0.528
0.171
0.181
0.860
0.862
0.323
0.342
In Table A3, we can reject the hypothesis that “between” and
“within” estimates may be jointly equal at the 1 percent level.
Furthermore, statistically significant differences are observed for “average
household size” and “percentage of civil marriages.” We can interpret the
diverging “between” and “within” estimates of our indicator of household
size in substantive terms. Provinces with larger average-household sizes
throughout the period observed (especially northeastern ones)—those
associated with higher death rates in hospitals—also experienced a sharp
decrease in household components over time, due to substantive changes
Figure A1
Standardized Residuals for the First Level
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
467
Figure A2
Standardized Residuals for the Second Level
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
in household structure. This decrease is more effective by virtue of the
higher average levels, with implications for deaths-in-hospitals changes.
By contrast, the test statistical value observed for “percentage of
civil marriages” suggests that this variable tends to be endogenous. Thus,
the “within estimate,” which is free from bias due to level-1 endogeneity
and refers to changes over time, is non-significant. Hence, interpretation
of this indicator’s effects must be cautious; it may also be affected by
other time-invariant characteristics of provinces that are not included
in the analysis.
Table A3 Test Statistics on Equal Between–Within Coefficients
Hospital beds
Malignant-cancer death rate
Average household size
Living in cities >20,000
Murders per 100,000
Percentage of civil marriages
Percentage of illiterates
Global test
CHI-SQ
0.40
0.97
7.85
1.85
0.82
33.57
0.04
45.81
p-VALUE
0.528
0.325
0.005
0.173
0.365
0.000
0.850
0.000
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
468
| ASH E R CO LOM BO A ND R OC CO MOL I NA RI
Table A4 Models with Interaction Terms
Year
1955
1883
1963
1974
1981
1987
1997
2004
2013
Macro-area
Northwest
Northeast
Center
South and the islands
Household size
Avg. family components (between)
Avg. family components (within)
Urbanization index
Living in cities>20,000 (between)
Living in cities>20,000 (within)
Macro-areaXFamily size
Northwest*family size (within)
Northeast*family size (within)
Center*family size (within)
South and the islands*family
size (within)
Macro-areaXUrbanization index
Northwest*urb index (within)
Northeast*urb index (within)
Center*urb index (within)
South and the islands*urb
index (within)
Constant
Observations
N of clusters
sigma_u
sigma_e
rho
MODEL (7)
MODEL (8)
ref.
−3.01
4.56***
10.66***
13.03***
12.87***
17.09***
21.70***
21.85***
ref.
10.17***
1.53
−5.84
3.98
−1.03
0.41
2.74***
ref.
−5.95***
−1.46
4.01
ref.
(5.55) −10.18*
(1.31)
(1.97)
(2.65)
(3.00)
(3.55)
(4.19)
(4.81)
5.06***
10.79***
12.20***
11.42***
14.32***
17.15***
15.47***
ref.
9.90***
1.12
−6.47
4.36
−2.53
0.43
−0.12
(2.35)
(2.47)
(3.79)
(4.39)
(2.26)
(0.42)
(0.56)
(1.34)
(1.53)
(2.07)
(4.49)
(1.24)
(1.84)
(2.45)
(2.78)
(3.28)
(3.84)
(4.36)
(2.40)
(2.51)
(3.85)
(4.50)
(1.56)
(0.43)
(0.97)
ref.
8.06***
3.17**
1.44
(1.09)
(1.09)
(1.22)
(19.32) −14.40
(19.72)
805
92
5.88
6.59
0.44
−14.92
805
92
5.68
6.63
0.42
*p<0.05.
**p<0.01.
***p<0.001.
NOTES Models also control for availability of medical facilities, epidemiological change,
spread of violent deaths, secularization index, and education index. All indicators include both
between and within effects. Standard errors in parentheses.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
D I S PL A C E M E NT O F D E A T H |
469
MODELS WITH INTERACTION TERMS This section presents estimates
from models with interaction terms that can be formalized as
yit ¼ α þ ζ
Þ þ β
ð
(cid:1)Zi∙ − zit
ð
þ β
5
þ β
2macro areai þ β3
1yeart
Þ (cid:2) macro areai þ uit;
i
(cid:1)Xi∙ − xit
ð
Þ þ β4
(cid:1)Xi∙
where z represents either the average household size or the percentage of
people living in cities with more than 20,000 inhabitants (urbanization
index). Models are designed to show the extent to which the impact
of the “within” component of these variables changes according to dif-
ferent macro-areas of Italy—northwest, northeast, center, south and the
islands (see Table A4).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
5
3
3
4
3
9
2
0
6
5
6
5
5
/
j
i
n
h
_
a
_
0
1
8
7
0
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3