Journal of Interdisciplinary History, LII:2 (Autumn, 2021), 155–176.
Valerie Shrimplin and Channa N. Jayasena
Was Henry VIII Infertile? Miscarriages and Male
Infertility in Tudor England Societies throughout the
world have traditionally viewed the production of healthy chil-
dren as the responsibility of women. Such was evidently the view
of King Henry VIII (1491–1547, Figure 1) who clearly blamed his
wives for his lack of a healthy male heir. Henry is well-known for
having married six times in his desperate quest for a son, disposing
of wives who did not fulfill their royal and marital duty. Henry
fathered three legitimate children—Mary I, Edward VI, and
Elizabeth I—but what is less well-known is the significant number
of unsuccessful pregnancies with which he was associated. Henry’s
first two wives, Catherine of Aragon and Anne Boleyn, had ten
pregnancies between them from 1509 to 1519 and from 1533 to
1536, respectively, but six resulted in miscarriage. Henry’s first son,
Prince Henry, who was born in 1511, lived less than two months
(see Table 1). Only two surviving daughters (Mary and Elizabeth)
reached maturity; his son Edward died at age fifteen.
Henry, naturally for a monarch of this era, accused his wives. He
also clung to the idea that his problems derived from his marriage to
the widow of his brother Arthur, which contravened Leviticus 20:21—
“If a man shall take his brother’s wife they shall be childless.” As a re-
sult, Henry disposed of Catherine and Anne accordingly, without
considering that his own fertility (or lack of it) may have played a role.
Valerie Shrimplin is Senior Research Associate, Gresham College. She is the author of Anne
Boleyn (London, 2019).
Channa N. Jayasena is Reader in Reproductive Endocrinology, Section of Investigative
Medicine, Imperial College London, Hammersmith Hospital, and Consultant in Reproduc-
tive Endocrinology & Andrology, Hammersmith & St. Mary’s Hospitals, Imperial College
Healthcare NHS Trust, London. He is the author of, with Richard Quinton, “Male Hypo-
gonadism and General Practitioners in the UK: How to Increase Case Recognition, without
Compromising Diagnostic Accuracy?” Clinical Endocrinology, available at https://doi.org/10
.1111/cen.14432.
The authors thank an anonymous referee for historical suggestions and references. Chan-
na N Jayasena is funded by an NIHR Post-Doctoral Fellowship. The views expressed herein are
the authors’, not necessarily those of the National Health Service, the National Institute for
Health Research, or the UK Department of Health.
© 2021 by the Massachusetts Institute of Technology and The Journal of Interdisciplinary
History, Inc., https://doi.org/10.1162/jinh_a_01695
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
156
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
Fig. 1 Portrait of Henry after Holbein, c 1530 (Wikimedia Commons)
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
The understanding at this time that men as well as women
could suffer from problems of infertility was tentative and unlikely
to have been countenanced by a Tudor monarch. Space does not
allow a complete survey of the late medieval/early modern med-
ical literature that included a mention of male infertility. Suffice it
to say that it was usually, but not always, confined to an inability to
perform. Yet, notwithstanding Rider’s observation that scholars
have tended to neglect males’ reproductive disorders in the Middle
Ages compared with females’, early references to male infertility
are available. Witness, for example, the late fourteenth-century
treatise by John of Mirfield, St. Bartholomew’s Hospital London,
which warned, “When sterility happens between married people,
the males are accused by many people of not having suitable seed.”
Similarly, Evans pointed out that the historical focus on female
.
n
o
i
t
a
m
m
u
s
n
o
c
–
n
o
n
f
o
s
d
n
u
o
r
g
e
h
t
n
o
e
u
s
s
i
,
0
4
5
1
t
u
o
h
t
i
w
5
1
d
e
g
a
d
e
i
d
d
r
a
w
d
E
y
l
u
J
9
n
o
d
e
l
l
u
n
n
a
s
a
w
e
g
a
i
r
r
a
m
d
e
d
r
o
c
e
r
s
e
i
c
n
a
n
g
e
r
p
o
N
)
e
v
i
t
c
a
y
l
l
a
u
x
e
s
t
o
n
d
e
m
u
s
s
a
;
d
e
i
r
r
a
m
n
u
(
n
o
t
h
g
u
o
r
b
(
h
t
n
o
m
h
t
4
n
r
o
b
l
l
i
t
s
r
o
n
i
e
g
a
i
r
r
a
c
s
i
e
g
a
i
r
r
a
c
s
i
M
M
.
h
t
r
i
b
g
n
i
v
i
g
r
e
t
f
a
s
k
e
e
w
o
w
t
d
e
i
d
e
n
a
J
)
?
k
c
o
h
s
y
b
9
6
d
e
g
a
e
u
s
s
i
t
u
o
h
t
i
w
d
e
i
d
,
I
h
t
e
b
a
z
i
l
E
)
s
h
t
n
o
m
8
(
s
r
u
o
h
/
s
y
a
d
w
e
f
a
d
e
v
i
l
r
o
n
r
o
b
l
l
i
t
S
)
5
5
5
1
n
i
a
p
S
f
o
I
I
)
d
e
fi
i
r
e
v
n
u
(
p
i
l
i
h
P
o
t
d
e
i
r
r
a
m
(
e
g
a
i
r
r
a
c
s
i
M
2
4
d
e
g
a
e
u
s
s
i
t
u
o
h
t
i
w
d
e
i
d
r
o
d
u
T
y
r
a
M
h
t
r
i
b
r
e
t
f
a
n
o
o
s
d
e
i
d
r
o
s
k
e
e
w
7
d
e
g
a
d
e
i
d
y
r
n
e
H
e
c
n
i
r
P
n
r
o
b
l
l
i
t
s
r
o
e
g
a
i
r
r
a
c
s
i
M
n
r
o
b
n
r
o
b
l
l
i
t
S
l
l
i
t
S
s
e
Y
o
N
s
e
Y
s
e
Y
o
N
s
e
Y
s
e
Y
o
N
s
e
Y
s
e
Y
o
N
3
1
5
1
0
1
5
1
1
1
5
1
y
r
a
u
n
a
J
1
3
y
r
a
u
n
a
J
1
5
1
5
1
y
r
a
u
n
a
J
8
r
e
b
m
e
t
p
e
S
7
1
6
1
5
1
y
r
a
u
r
b
e
F
8
1
)
y
r
n
e
H
(
e
l
a
m
e
F
e
l
a
e
l
a
e
l
a
M
M
M
)
y
r
a
M
(
e
l
a
m
e
F
4
3
5
1
r
e
b
m
e
t
p
e
S
/
t
s
u
g
u
A
6
3
5
1
y
r
a
u
n
a
J
9
2
e
l
a
e
l
a
M
M
7
3
5
1
r
e
b
o
t
c
O
2
1
)
d
r
a
w
d
E
(
e
l
a
M
8
1
5
1
r
e
b
m
e
v
o
N
0
1
7
1
5
1
n
w
o
n
k
n
U
e
l
a
m
e
F
3
3
5
1
r
e
b
m
e
t
p
e
S
7
)
h
t
e
b
a
z
i
l
E
(
e
l
a
m
e
F
I
N
O
T
A
M
R
O
F
N
I
I
L
A
N
O
T
D
D
A
I
I
E
G
A
R
R
A
C
S
I
M
?
H
T
R
I
B
L
L
I
T
S
R
O
I
G
N
R
P
S
F
F
O
F
O
E
T
A
D
)
N
W
O
N
K
F
I
(
H
T
R
I
B
D
E
D
R
O
C
E
R
I
G
N
R
P
S
F
F
O
F
O
X
E
S
.
7
1
r
o
6
1
c
s
a
w
e
g
a
i
r
r
a
m
e
u
s
s
i
o
N
t
a
e
g
A
y
b
a
b
d
a
h
t
u
b
,
y
r
n
e
H
h
t
i
w
e
u
s
s
i
o
N
d
n
a
b
s
u
h
t
n
e
u
q
e
s
b
u
s
h
t
i
w
e
u
s
s
i
o
N
.
9
4
s
a
w
y
r
n
e
H
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
d
e
d
r
o
c
e
r
s
e
i
c
n
a
n
g
e
r
p
o
N
d
e
d
r
o
c
e
r
s
e
i
c
n
a
n
g
e
r
p
o
N
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
.
c
i
l
a
t
i
n
i
d
e
t
a
c
i
d
n
i
e
r
a
n
e
r
d
l
i
h
c
g
n
i
v
i
v
r
u
s
f
o
s
e
m
N
a
E
T
O
N
y
r
n
e
H
o
t
d
e
i
r
r
a
m
3
3
5
1
–
9
0
5
1
n
o
g
a
r
A
f
o
e
n
i
r
e
h
t
a
C
E
F
I
W
6
3
5
1
–
3
3
5
1
y
r
n
e
H
o
t
d
e
i
r
r
a
m
n
y
e
l
o
B
e
n
n
A
7
3
5
1
–
6
3
5
1
y
r
n
e
H
o
t
d
e
i
r
r
a
m
r
u
o
m
y
e
S
e
n
a
J
s
e
v
e
l
C
f
o
e
n
n
A
y
r
n
e
H
o
t
d
e
i
r
r
a
m
0
4
5
1
y
l
u
J
–
y
r
a
u
n
a
J
d
r
a
w
o
H
e
n
i
r
e
h
t
a
K
d
e
i
r
r
a
m
r
r
a
P
2
4
5
1
–
0
4
5
1
y
r
n
e
H
e
n
i
r
e
h
t
a
C
7
4
–
3
4
5
1
y
r
n
e
H
o
t
o
t
d
e
i
r
r
a
m
s
e
s
s
o
L
y
c
n
a
n
g
e
r
P
d
n
a
n
e
r
d
l
i
h
C
,
s
e
v
i
W
:
I
I
I
V
y
r
n
e
H
f
o
y
r
o
t
s
i
H
e
v
i
t
c
u
d
o
r
p
e
R
1
e
l
b
a
T
158
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
infertility has largely relegated male reproductive failure to sexual
performance and impotence. Male infertility was not recognized as
a significant issue until the early modern period, roughly around
the turn of the seventeenth century.1
Undeterred by the small number of late medieval medical texts
that did not entirely discount the male role, Henry’s practice of
disposing of his wives unmistakeably demonstrates whom he
considered to blame for infertility. Unfortunately for his wives,
Henry was blissfully unaware that, as demonstrated by recent
research, some men, particularly those with sperm deficiencies,
may not only have a significant effect on pregnancy but also poten-
tially be the cause of miscarriage and stillbirth.2
Identifiable reasons for miscarriage are not always easy or even
possible to determine, but increasingly moving attention from women
to men has recently led to investigations into male chromosomes,
DNA, and lifestyle choices, such as diet and exercise. The traditional
focus on women regarding recurrent miscarriage was also due to
the fact that, although females normally produce single eggs, millions
of male sperm are automatically subject to “natural selection,” only
the fittest among them able to reach and fertilize an egg. Male infer-
tility (reduced sperm function) currently affects half of all couples
seeking fertility treatment, and global sperm counts are reported to
have halved since the 1970s. Furthermore, a growing body of research
suggests that deficient sperm function in a male partner can predispose
1 Catherine Rider, “Men and Infertility in Late Medieval English Medicine,” Social History
of Medicine, XXIX (2016), 245–266; idem, “Men’s Responses to Infertility in Late Medieval
England,” in Gale Davis and Tracey Loughran (eds.), A Handbook of Infertility in History:
Approaches, Contexts and Perspectives (London, 2017); idem and Daphna Oren-Magidor, “Intro-
duction to Infertility and Medicine in Medieval and Early Modern Medicine,” Social History of
Medicine, XXIX (2016), 211–223; Jennifer Evans, Aphrodisiacs, Fertility and Medicine in Early
Modern England ( Woodbridge, 2014), 192–193. Oren-Magidor—in Infertility in Early Modern
England (London, 2017)—provides further evidence but also states that “while early modern
medicine recognized the existence of male infertility, in practice women were usually
‘blamed’ for childlessness and treated for it” (6). For comparisons with continental Europe,
see Danielle Jacquart and Claude Tommasset (trans. Matthew Adamson), Sexuality and
Medicine in the Middle Ages (New York, 1988).
2 Guidance in female medicine circulated via the twelfth-century Latin Trotula texts. The
earliest English text for midwives dates from 1540. For the practical handbook on midwifery
produced in 1554 by Jacob Rueff (1500–1558) of Zurich, see Audrey Eccles, Obstetrics and
Gynaecology in Tudor and Stuart England (London, 2019; orig. pub. 1982), esp. 11–22. The
possible male role in infertility and miscarriage was not seriously recognized, however, until
the early modern period (1550–1780), postdating the current case study of Henry VIII and
demonstrating the need for its consideration.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
M I S C A R R I A G E S A N D MA L E I N F E R T I L I T Y
| 159
couples to recurrent pregnancy loss (RPL) or miscarriage, which is
commonly defined as three or more consecutive pregnancy losses
prior to twenty weeks’ gestation, affecting 1 to 2 percent of couples.
Recent studies highlight that damaged sperm from men may be
the reason why women suffer repeated miscarriages.3
Factors impairing male fertility, such as semen oxidative stress
and sperm DNA fragmentation, are normally elevated in male
partners of women with RPL when compared with other men.
Currently, the only approved therapy for affected couples with
male infertility is assisted reproductive technology (ART), such as
in-vitro fertilization therapy (IVF) or intracytoplasmic sperm injec-
tion (ICSI). However, only a minority of health-care systems and
couples worldwide can afford the high costs of ART, and only lim-
ited research has been performed in recent decades on the devel-
opment of novel therapies for couples with male infertility. Due to
the historical idea that producing healthy children is the exclusive
responsibility of women, male infertility remains an emasculating
condition carrying a powerful social stigma, which often impairs
the ability of men and their partners to seek appropriate support.
An exploration of the historical background of male infertility
helps to challenge the image of male infertility as a condition of
weakness in affected men.4
3 Hagai Levine et al., “Temporal Trends in Sperm Count: A Systematic Review and Meta-
Regression Analysis,” Human Reproduction Update, XXIII (2017), 646–659; Royal College of
Obstetrics and Gynaecology, “Recurrent Miscarriage, Investigation and Treatment of Cou-
ples” (Green-top Guideline No. 17), available at https://www.rcog.org.uk/en/guidelines
-research-services/guidelines/gtg17/; Holly B. Ford and Danny J. Schust, “Recurrent Preg-
nancy Loss: Etiology, Diagnosis, and Therapy,” Reviews in Obstetrics & Gynecology, II (2009),
76–83. See also https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC2709325/.
Syed N. Imam et al., “Idiopathic Recurrent Pregnancy Loss: Role of Paternal Factors: A
4
Pilot Study,” Journal of Reproductive Infertility, XII (2011), 267–276; Ralf Henkel, “Leukocytes
and Oxidative Stress: Dilemma for Sperm Function and Male Fertility,” Asian Journal of
Andrology, XIII (2011), 43–52; idem et al., “Influence of Deoxyribonucleic Acid Damage on
Fertilization and Pregnancy,” Fertility and Sterility, LXXXI (2004), 965–972; Jordi Ribas-
Maynou et al., “Alkaline and Neutral Comet Assay Profiles of Sperm DNA Damage in Clin-
ical Groups,” Human Reproduction, XXVII (2012), 652–658; Luke Simon et al., “Sperm DNA
Damage Measured by the Alkaline Comet Assay as an Independent Predictor of Male Infer-
tility and in Vitro Fertilization Success,” Fertility and Sterility, XCV (2011), 652–657; Jayasena
et al., “Reduced Testicular Steroidogenesis and Increased Semen Oxidative Stress in Male
Partners as Novel Markers of Recurrent Miscarriage,” Clinical Chemistry, LXV (2019), 161–
169; “Fertility Problems: Assessment and Treatment,” Clinical guideline [CG156], February
2013, Updated September 2017, National Institute of Clinical Excellence, available at https://
www.nice.org.uk/guidance/cg156; Shafali Talisa Arya and Bridget Dibb, “The Experience of
Infertility Treatment: The Male Perspective,” Human Fertility, XIX (2016), 242–248.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
160
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
This interdisciplinary article provides the first detailed investi-
gation of miscarriage rates before the modern era that centers on
males. It uses historical records to document miscarriage rates among
a sample of noblemen, including Henry VIII, and their wives in
Tudor England during the late fifteenth and early sixteenth century.
Evidence suggests that at least part of the cause for the multiple
miscarriages of Henry’s wives may have been male infertility.
METHODOLOGY Details of Henry VIII’s marriages and progeny
derive from primary and secondary historical sources and are further
evaluated via extensive twenty-first-century medical research into
male infertility. Scrutiny focused first on Henry’s known progeny
before turning to his antecedents and possible genetic traits.
Information about Henry’s medical records is widely available
in the literature, including his known diseases, physical injuries, and
psychological inclinations. Most importantly, the records of the
Tudor Royal household for banquets, kitchens, and dining provide
information about his diet. We compared the backgrounds of
his wives’ families with those of his contemporaries, specifically
thirty-one noblemen with extant marriage and birth documenta-
tion whose wealth and social standing were similar to Henry’s.
Records of pregnancies and births permit the calculation of miscar-
riage rates for individual couples and further analysis of the descrip-
tive statistics.
HENRY VIII’S MARITAL AND REPRODUCTIVE HISTORY Having be-
come just the second monarch of a shaky new dynasty at the
age of seventeen in 1509, Henry VIII was obsessed with producing
a healthy male heir. Table 1 lists his wives, children, and failed
pregnancies, so far as known. Henry married his brother’s widow
Catherine of Aragon (born 1485), who was six years his senior,
almost immediately on becoming king. Catherine fell pregnant
regularly within the first ten years of the marriage; the announce-
ment of her first pregnancy occurred just two months after the
wedding (when she was twenty-four). As detailed in Table 1,
her first miscarriage/still birth in 1510 was followed by further
miscarriages and the loss of an infant son. As Starkey noted, rumors
had circulated since 1514 that “the King of England meant to
repudiate his present wife . . . since he is unable to have children
by her,” thus ascribing blame to Catherine. A healthy child (Mary)
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
M I S C A R R I A G E S A N D MA L E I N F E R T I L I T Y
| 161
was not produced until 1516, seven years after the marriage, at a
time when Henry was emphasizing his sexual prowess (epitomized
by the size of his codpieces) and trying to produce a male heir. In
1519, King Francis I bluntly stated that Henry “had an old de-
formed wife.” By the 1520s, Catherine was in her mid-thirties
and probably menopausal since she had become overweight and
had not fallen pregnant since 1518. Henry later stated, as cited
by Weir, that by early 1525, when Catherine’s periods had ceased,
he had stopped having sexual relations with her. He banished her
from court and annulled the marriage in 1533.5
Henry’s evidence that his wife was at fault for the absence of a
male heir was the son that he had fathered with another woman,
Bessie Blount, his acknowledged mistress from roughly 1514 to
1522. He bragged heartily about his illegitimate son (Henry Fitzroy,
1519–1536), showering him with titles and honors from the age of
six. Blount had six more children with two husbands after Henry, all
of whom lived to maturity. Henry may have had other illegitimate
children—following his affairs with Anne Boleyn’s older sister
Mary, Madge Shelton, and other mistresses—but since he did not
acknowledge any others (to assert his own fertility), any putative
ones are excluded from this study. Mary Boleyn became pregnant
when she married after the affair ended, as did Catherine Parr,
Henry’s sixth wife, when she married after Henry died. In spite of
the birth of his daughter Mary and that of an illegitimate son, Henry
never questioned his own fertility, apparently to save face and pro-
tect a conviction about his own virility, and he could always fall back
on the curse of Leviticus dating to his marriage with Catherine.
Anne Boleyn seems to have come to Henry’s attention in 1525.
He proposed to her in 1527, but the couple seems to have abstained
from intercourse until their marriage in 1532/3, as verified by
Henry’s letters to her (which also confirm his passion for intimate
relations), probably to ensure that any child would be legitimate.
5 David Starkey, Six Wives: The Queens of Henry VIII (New York, 2004), 24–26, 161, 197–
198. For the need to produce dynastic heirs, the raison d’être of medieval and Renaissance
royalty, see also Robert Bartlett, Blood Royal: Dynastic Policies in Medieval Europe (New York,
2020), 2–88 (esp. 69), 89–108. Eric Ives, The Life and Death of Anne Boleyn: The Most Happy
(Oxford, 2005), 83; Alison Weir, Henry VIII: King and Court (New York, 2008; orig. pub.
2001), 247. For further information about women, aging, and the cessation of fertility at men-
opause in the sixteenth century, see Lynn Botelho and Pat Thane (eds.), Women and Ageing in
British Society since 1500 (London, 2001); Sara Read, Menstruation and the Female Body in Early
Modern England: Genders and Sexualities in History (New York, 2013), 171–180.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
162
Henry’s letters refer to multiple mistresses; most likely they were not
with women of noble birth thus to avoid complicating the succes-
sion if any of them were to bear a son while he waited to marry
Anne. After marriage, Anne, like Catherine, became pregnant
annually, as would have been the couple’s aim. The birth of a girl,
Elizabeth, in September 1533 was a disappointment, but at least it
proved Anne to be fertile. Miscarriages followed in 1534 and 1536.
Anne’s story repeated Catherine’s; Henry (now in his mid-forties)
still had no male heir. Rumors about Anne’s incapacity to bear
children emerged, and her last miscarriage was the final blow.6
During about fourteen years of “active” marriage, Henry’s
first two wives experienced ten pregnancies and seven miscarriages/
neonatal deaths and no surviving sons. The reasons for the king’s lack
of success were never fully explained, notwithstanding his allocation
of blame to the women. During Anne Boleyn’s treason trial, in
which she was accused of having affairs with as many as seven other
men, allegations about Henry’s impotence surfaced. Anne’s brother
George suggested that Henry was incapable of sexual intercourse
(“was no good in bed with women, and that he had neither potency
nor force”). Anne Boleyn, her brother, and four others were executed
a few days later in May 1536.7
Henry married Jane Seymour in the same month as Anne
Boleyn’s execution (May 1536). She swiftly became pregnant
but died in 1537 of complications following the birth of Edward
VI on October 12, 1537. Henry married Anne of Cleves in 1540
but claimed that they did not consummate their marriage, citing
his lack “of the will and power to consummate the same.”
Katherine Howard, Henry’s fifth wife, aged about sixteen, was
married to Henry for just two years before she, too, was executed.
She and Catherine Parr, Henry’s last wife, also failed to become
pregnant by Henry.8
6 The couple had two marriage ceremonies, on November 14, 1532, and January 25, 1533.
See Starkey, Six Wives, 463, 474; Ives, Life and Death of Anne Boleyn, 162. Starkey, Six Wives,
553–554.
Starkey, Six Wives, 580; Ives, Life and Death of Anne Boleyn, 191. Considering Anne’s
7
machinations to gain Henry as a husband, the idea that she had affairs with five to seven
men, including her brother (possibly to fall pregnant if Henry failed), seems ludicrous. See
Shrimplin, Anne Boleyn (London, 2019), 23.
8
Ives, Life and Death of Anne Boleyn, 191, 393 n. Incidentally, no record of Henry having
been treated for syphilis (unlike his contemporary Francis I King of France) appears to exist.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
M I S C A R R I A G E S A N D MA L E I N F E R T I L I T Y
| 163
Could it be mere coincidence that, although Henry’s first three
wives became pregnant easily and regularly, so high an incidence of
fertility problems (70 percent failure rate) occurred and that none of
Henry’s last three wives was even able to conceive? Can the finger
point to Henry as the common factor and cause of his own misfor-
tune? The fact that Henry was responsible for at least eleven known
pregnancies (including the birth of Henry Fitzroy) from 1509 to 1519
and from 1532 to 1536) might bode well for his fertility and fitness.
But, in fact, his many failures with different partners could well sug-
gest otherwise. The loss of five sons must have weighed heavily.9
POSSIBLE REASONS FOR HENRY’S PLIGHT Regardless of the extent or
efficacy of Henry’s sexual performance in his last years (1540–1547),
the evidence from earlier in his life cannot rule out some liability on
Henry’s part. As he lamented, why could he not produce a child
when the least of his subjects could? In 1533, he exclaimed to
Eustace Chapuys, the Spanish ambassador, “Am I not a man like
any other?” In sixteenth-century terms, sexual potency was associ-
ated with having children—something that would not be the case if
sperm were impaired. The fact that none of Henry’s surviving chil-
dren had any issue is further evidence that the problem lay with him
rather than (or at least as much as) with his wives.10
Hence, Henry’s medical records, genetic disposition, and life-
style merit investigation, in comparison with those of men of a sim-
ilar class and standing during the same era. Old age undoubtedly
contributes to infertility. Other risk factors contributing to it, of
which Henry and his physicians would not have been aware, are
stress, lack of exercise, obesity, and illness. Lifestyle choices linked
to weight, diet, nutrition, alcohol intake, medication, and drug use
9
If, as has been suggested, Henry carried the Kell antiogen, and his wives were Kell-negative,
miscarriages could have been the result. The McLeod syndrome, related to Kell blood-group
disorders, is also a cause of psychosis, perhaps explaining Henry’s transformation in his later years.
Brain damage from a serious fall while jousting in 1536 is another possible explanation for it. See
Peter Stride and Kylie Lopes Floro, “Henry VIII, McLeod Syndrome and Jacquetta’s Curse,”
Journal of the Royal College of Physicians of Edinburgh, XLIII (2013), 353–360. See also Miles F.
Shore, “Henry VIII and the Crisis of Generativity,” Journal of Interdisciplinary History, II
(1972), 359–390, for further discussion of Henry’s psychology.
Starkey, Six Wives, 503; Ives, Life and Death of Anne Boleyn, 191–192. Henry’s line
10
stopped with his children, who all died childless. The members of the British royal family
have included no descendants from Henry VIII, only from his father Henry VII via his sister
Margaret (mother of Mary Queen of Scots, grandmother to James I).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
164
affect sperm viability and thus have a significant effect on the health
of a pregnancy. Like a complete lack of exercise, highly intense,
competitive-level training may also decrease sperm health. As a
young man, Henry favored hunting, jousting, and other high-
impact sports of his era. On many occasions, he suffered severe
wounds, and in 1524 and 1536, he narrowly escaped being killed.
The assumption in Henry’s time that men remain fertile while
women lose fertility dramatically with age is not entirely accurate.
Apart from the inability to “perform” (erectile dysfunction), the
fertility of men also declines as they get older, and the risk of mis-
carriage may sometimes increase, even with young female partners.
This finding could be pertinent to Henry, as well as to many mod-
ern couples who start families later in life, although today’s pres-
sures probably cannot compare with the stresses on medieval and
early modern kings and queens.11
HENRY’S MEDICAL RECORDS AND GENETIC HISTORY Henry’s ante-
cedents on his mother’s side appeared to have been exceptionally
fertile. Edward IV, his maternal grandfather, had fifteen children,
ten legitimate and five illegitimate. Only one died in infancy
(other than the “Princes in the Tower,” who were murdered).
Richard Plantagent, Edward IV’s father, had twelve legitimate
children with Cecily Neville, of whom eight lived to maturity.
Henry’s paternal antecedents, however, were less fertile. Henry
VII and Elizabeth of York (daughter of Edward IV), Henry’s
Sarah Toulalan, “‘Elderly Years Cause a Total Dispaire of Conception’: Old Age, Sex
11
and Infertility in Early Modern England,” Social History of Medicine, XXIX (2016), 333–359;
James Wall and Jayasena, “Diagnosing Male Infertility,” British Medical Journal, October 4,
2018, 363, available at https://doi.org/10.1136/ bmj.k3202. Imperial College, which conducted
a study of men whose partners miscarried multiple times, found sperm problems that could
be linked to age, weight, and diet, concluding that sperm health can have a significant effect
on pregnancy. Smoking, which is now also included as a major risk, would not have been
applicable to the early sixteenth century. Pawel Jóźków and Marco Rossato, “The Impact of
Intense Exercise on Semen Quality,” American Journal of Men’s Health, XI (2017), 654–662;
Rakesh Sharma et al., “Effects of Increased Paternal Age on Sperm Quality, Reproductive
Outcome, and Associated Epigenetic Risks to Offspring,” Reproductive Biology and Endocrinology,
XIII (2015), 35, available at doi: 10.1186/s12958-015-0028-x. According to the Office for
National Statistics, for marriages of opposite-sex couples in the United Kingdom, the average
(mean) age for men marrying in 2015 was 37.5 years; for women, it was 35.1 years. See
https://www.ons.gov.uk/peoplepopulationandcommunity/ birthsdeathsandmarriages
/marriagecohabitationandcivilpartnerships/bulletins/marriagesinenglandandwalesprovisional
/2015#the-average-age-at-marriage-continued-to-rise.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
M I S C A R R I A G E S A N D MA L E I N F E R T I L I T Y
| 165
parents, had six children, one of whom died young, and his older
brother Arthur lived only to age fifteen. Henry VII was an only
child, since his father died when he was twenty-six, leaving a preg-
nant thirteen-year-old widow, Margaret Beaufort, who had no
further children from subsequent marriages. That Henry VIII’s
paternal great-grandfather was also an only child was unlikely to
have been by choice. The survival rate was admittedly lower,
and childbirth riskier, in that era than in modern times, but (as
shown by Henry VIII’s maternal lineage) many families of all clas-
ses and strata of society successfully produced multiple offspring.12
The fertility of Catherine of Aragon’s family was by no means
impaired. Catherine was one of eight siblings, six of whom
reached maturity, and her father also had many confirmed illegit-
imate children. One of Catherine’s sisters died young in childbirth,
but the other two produced sixteen children between them, only
two of whom did not survive to maturity. Likewise, Anne Boleyn
was one of five siblings. Her paternal grandfather had ten children;
all but one lived to maturity. Her mother was one of seventeen
siblings and step-siblings.
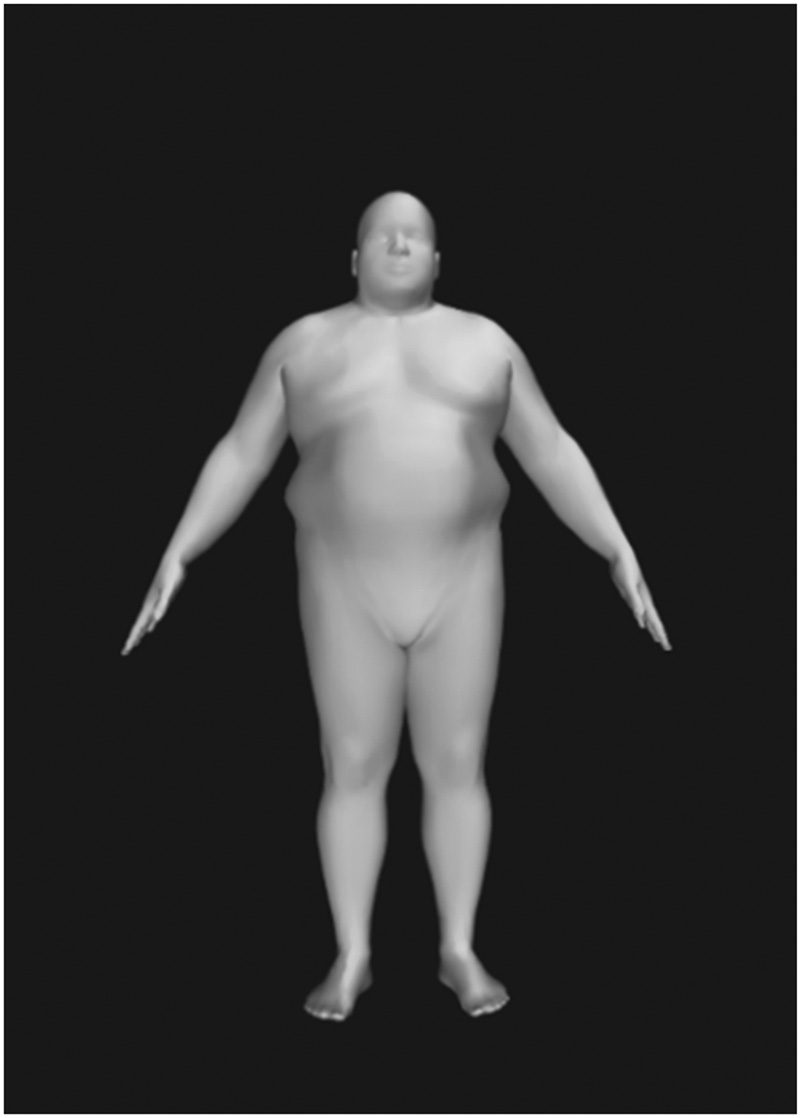
Henry’s Health, Medical Condition, and Lifestyle The potential
causes of Henry’s male infertility could have been related to any of
the risk factors outlined earlier. In his youth, he was a strapping
sport enthusiast with a muscular build and a forty-two-inch chest.
By his thirties, however, Henry had become grossly overweight.
Estimates gleaned from his clothing and armor indicate that he
eventually attained a height of 6’, 1” (185 cm), a waist of fifty-four
inches (137 cm), a chest of fifty-eight inches, and a weight of 400 lb
(28 stone or 180 kilos) (see Figure 2). A recent meta-analysis iden-
tified obesity as strongly associated with poor sperm quality in men;
Henry VIII was almost certainly morbidly obese with a body mass
index (BMI) of 51.9 kg/m2.13
Henry’s court was notorious for its continuous celebrations,
lavish parties, and banquets, during which alcohol flowed freely.
12 Cecily Neville’s father had an amazing twenty-two children, eight with his first wife and
fourteen with his second. Only four died in the year of birth. Information relating to Henry’s
antecedents comes from accessible online sources for ease of reference.
13 Wall and Jayasena, “Diagnosing Male Infertility.” For the estimate of Henry’s measure-
ments, see, for example, software at https://bodyvisualizer.com/ (accessed February 2019).
Sermondade et al., “BMI in Relation to Sperm Count: An Updated Systematic Review
and Collaborative Meta-Analysis,” Human Reproduction Update, XIX (2013), 221–231.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
166
Fig. 2 Visualization of Henry VIII’s Body
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
SOURCE https://bodyvisualizer.com/ (accessed February 17, 2019.)
Although, as king, Henry would have had access to the best food,
medical care, and sanitation, he would also have suffered from
poor nutrition. His diet was excessively rich in meat/protein,
comprised of game (lamb, venison, and swan), along with much
bread and other carbohydrates. It was almost bereft of the vegeta-
bles and pulses (beans, peas, and lentils, which were considered to
be peasant food) that supply vitamins and fiber. Fruit was included
on menus but normally cooked or crystallized with sugar; fresh
fruit was thought to cause fever. According to Historic Royal
Palaces, “Meals were not just about eating. They were a display of
the monarch’s power. . . . Exotic foods demonstrated wealth. . . .
Poorer families would have rarely enjoyed meat, eating a diet of
stewed vegetables and pulses. But the luxury of the court was fresh
meat. Tudor courtiers enjoyed a wide variety of food, with freshly
slaughtered, roasted meat every day. . . . Courtiers were served a
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
M I S C A R R I A G E S A N D MA L E I N F E R T I L I T Y
| 167
menu of dishes containing around 5000 calories a day! . . . The
Oxford scholar, Thomas Starkey noted [around 1529] that ‘if they
do not have 20 varied meat dishes at supper they consider them-
selves slighted.’”14
Figure 3 displays a typical menu, as recorded in the Ordi-
nances for Eltham Palace. At Hampton Court, about 600 meals
were prepared twice a day. No meal was without roasted meat,
and wine “fountains” were common. Even when he ate alone
in his chamber, as he often did, Henry chose from a huge buffet
of meats (roasted or served in pies), followed by sweet preserves.
Not surprisingly, even in his youth but increasingly as he aged,
Henry had a seriously compromised diet, over-rich in protein
and almost completely lacking in vitamins. He possibly suffered
from scurvy, caused by lack of vitamin C, due to the absence of
fresh fruit and vegetables (not unlike modern meat/bread and
fast-food diets). His poor nutrition must have contributed to his
medical problems of constipation, gout, diabetes, massive open
sores/ulcers on his legs, and high blood pressure—not to mention
his fertility/sperm quality. Given his probable genetic heritage,
his increasingly unhealthy diet, and possible injuries from his ac-
tive years, Henry seems likely to have suffered from damage to
sperm (DNA fragmentation). Hence, the consistent problems with
miscarriage and stillbirth probably originated with him.15
14 Robert Hutchinson, The Last Days of Henry VIII: Conspiracy, Treason and Heresy at the
Court of the Dying Tyrant (London, 2005), 139. For the information about meals, see
https://www.hrp.org.uk/hampton-court-palace/ history-and-stories/tudor-food-and-eating/
#gs.f1uTqlPH; David Gentilcore, Food and Health in Early Modern Europe: Diet, Medicine and
Society 1450–1800 (New York, 2016), 9–26, 54; Alison Sim, Food and Feast in Tudor England
(Stroud, 2011; orig. pub. 1997), 6–11, 41–42, 74; for Henry’s gluttony, Joan Thirsk, Food in
Early Modern England: Phases, Fads, Fashions, 1500–1760 (New York, 2006), 18–19.
See Ordinances for the Household made at Eltham in the XVIIth year of King Henry VIII, 1526 A.
15
D. (174), available at https:// books.google.co.uk/ books?id=WcU_AAAAcAAJ&pg=RA2
-PA174&lpg=RA2-PA174&dq=pestells+of+reed+deere&source=bl&ots=2VXr-_9sz0&sig
= A C f U 3 U 3 x i G s J – 6 C V e y H u n h k v w c Z F f u _ Z E Q & h l = e n & s a = X & v e d
=2ahUKEwjuu4Xb0rjgAhWDSRUIHeSWCgEQ6AEwDXoECAcQAQ#v=onepage&q
=pestells%20of%20reed%20deere&f=false. Krissi Danielsson, “Sperm Quality Issues and Mis-
carriage,” available at https://www.verywellfamily.com/can-problems-in-sperm-cause
-miscarriage-2371837. A recent study at the University of Reading, in association with Historic
Royal Places, created a simulated model of Henry’s gut, concluding that Henry probably con-
sumed about 226 gm of protein per day, around four times the current recommended daily
allowance. See https://www.futurelearn.com/courses/royal-food/0/steps/17046.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
168
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
Fig. 3 Typical Menu Served at a Banquet Held by Henry VIII
(Ordinances for Eltham Palace)
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
REPRODUCTIVE HISTORY OF HENRY’S NOBLE CONTEMPORARIES The
extent to which the fertility problems experienced by Henry and
his wives were abnormal for his era is evident in an investigation
of other contemporary couples with social backgrounds similar
to those of Henry and his wives. Table 2 provides details of the
pregnancy/fertility success rate of Henry’s antecedents and peers
(noble courtiers and favorites) based on their verified legitimate
children. Data about miscarriages and neonatal deaths for nobles
)
e
t
a
m
i
t
i
g
e
l
l
i
1
+
(
r
e
h
t
a
f
d
n
a
r
g
–
t
a
e
r
g
l
a
n
r
e
t
a
p
I
I
I
V
y
r
n
e
H
e
n
o
e
f
i
w
s
i
h
(
r
e
h
t
a
f
d
n
a
r
g
–
t
a
e
r
g
)
s
g
n
i
l
b
i
s
p
e
t
s
/
s
g
n
i
l
b
i
s
2
2
f
o
r
e
h
t
a
f
d
n
a
r
g
l
a
n
r
e
t
a
p
I
I
I
V
y
r
n
e
H
r
e
h
t
a
f
d
n
a
r
g
l
a
n
r
e
t
a
m
I
I
I
V
y
r
n
e
H
)
6
2
e
g
a
e
u
g
a
l
p
f
o
d
e
i
d
(
l
a
n
r
e
t
a
m
I
I
I
V
y
r
n
e
H
;
l
a
n
i
d
r
a
c
a
s
a
w
(
e
t
a
m
i
t
i
g
e
l
l
i
h
t
o
B
)
e
t
a
m
i
t
i
g
e
l
l
i
5
s
u
p
(
l
r
e
h
t
a
f
I
I
I
V
y
r
n
e
H
%
0
%
3
3
%
0
%
0
2
%
0
%
3
4
f
o
e
n
O
.
l
a
i
r
t
r
e
h
t
a
d
e
d
i
s
e
r
p
o
h
w
s
g
n
i
l
b
i
s
p
e
t
s
/
s
g
n
i
l
b
i
s
6
1
e
l
c
n
u
s
’
)
t
e
i
d
h
c
i
r
e
n
n
A
l
.
k
o
f
r
o
N
f
o
e
k
u
d
d
r
3
%
5
.
2
1
d
a
h
n
o
s
s
i
h
;
r
e
h
t
a
f
e
n
i
r
e
h
t
a
C
(
s
’
e
t
a
m
i
t
i
g
e
l
l
i
2
.
)
e
l
t
t
a
b
a
e
s
.
d
(
l
a
v
a
n
l
,
k
o
f
r
o
N
e
k
u
D
n
o
s
d
n
2
I
I
I
V
y
r
n
e
H
f
o
g
n
i
r
r
e
n
n
I
r
u
o
m
y
e
S
e
n
a
J
f
o
r
e
h
t
a
F
)
e
f
i
w
h
t
4
s
’
y
r
n
e
H
(
e
t
a
m
i
t
n
i
d
n
a
,
e
l
c
r
i
c
I
I
I
V
y
r
n
e
H
%
0
3
a
/
n
%
0
%
0
4
3
/
0
2
1
/
4
1
/
0
0
1
/
2
7
/
3
2
/
0
8
/
?
1
0
1
/
3
a
/
n
5
/
2
3
/
0
3
8
1
8
4
2
4
7
0
3
3
1
1
1
1
1
0
2
1
2
1
1
S
E
T
O
N
S
S
O
L
H
T
R
I
B
L
L
I
T
S
R
O
I
D
E
V
V
R
U
S
S
E
V
W
I
F
O
E
T
A
R
S
E
I
C
N
A
N
G
E
R
P
N
I
I
G
N
T
L
U
S
E
R
Y
C
N
A
N
G
E
R
P
I
E
G
A
R
R
A
C
S
I
M
S
E
I
B
A
B
S
E
T
A
D
I
L
A
C
G
O
L
O
N
O
R
H
C
(
)
R
E
D
R
O
S
E
M
A
N
1
6
–
0
0
4
1
c
r
o
d
u
T
n
i
a
w
O
0
6
–
1
1
4
1
e
k
u
d
d
r
3
d
r
a
h
c
i
R
k
r
o
Y
f
o
6
5
–
0
3
4
1
r
o
d
u
T
d
n
u
m
d
E
3
8
4
1
–
2
4
4
1
9
0
5
1
–
7
5
4
1
0
3
5
1
–
3
7
4
1
4
5
5
1
–
3
7
4
1
y
e
s
l
o
W
s
a
m
o
h
T
I
I
V
y
r
n
e
H
d
r
a
w
o
H
s
a
m
o
h
T
V
I
d
r
a
w
d
E
3
1
5
1
–
7
/
6
7
4
1
d
r
a
w
o
H
d
r
a
w
d
E
6
3
5
1
–
4
7
4
1
r
u
o
m
y
e
S
n
h
o
J
9
3
5
1
–
6
7
4
1
7
1
5
1
–
3
8
4
1
n
y
e
l
o
B
r
r
a
P
s
a
m
o
h
T
s
a
m
o
h
T
)
e
u
s
s
i
o
n
,
s
e
v
i
w
3
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
I
I
I
V
y
r
n
e
H
f
o
s
e
i
r
a
r
o
p
m
e
t
n
o
C
n
e
m
e
l
b
o
N
f
o
s
e
i
r
o
t
s
i
H
e
v
i
t
c
u
d
o
r
p
e
R
2
e
l
b
a
T
d
e
i
d
e
m
o
S
.
y
r
a
M
,
r
e
t
s
i
s
d
e
i
r
r
a
m
,
I
I
I
V
y
r
n
e
H
o
t
s
’
y
r
n
e
H
e
s
o
l
c
y
r
e
V
s
r
e
t
h
g
u
a
d
2
(
I
I
I
V
y
r
n
e
H
f
o
r
e
t
s
i
n
M
i
+
6
d
n
u
o
r
a
d
e
g
a
n
e
r
d
l
i
h
c
s
a
;
s
e
i
b
a
b
s
a
t
o
n
t
u
b
g
n
u
o
y
)
e
t
a
m
i
t
i
g
e
l
l
i
e
n
o
d
e
i
d
s
u
p
l
e
l
t
t
a
b
n
i
d
e
i
d
,
r
e
i
d
o
s
l
,
e
t
i
r
o
v
a
F
.
I
I
I
V
y
r
n
e
H
d
n
e
i
r
f
e
s
o
C
l
l
.
d
o
h
e
s
u
o
h
l
a
y
o
r
f
o
r
e
l
l
o
r
t
p
m
o
C
)
t
h
g
i
e
w
r
e
v
o
s
a
w
(
e
u
s
s
i
o
N
r
e
i
d
o
s
l
,
e
t
i
r
o
v
a
f
g
n
i
k
e
h
t
o
t
l
a
y
o
R
e
s
o
C
l
%
0
%
0
%
0
%
0
5
/
0
4
/
0
8
/
0
3
/
0
%
0
a
/
n
e
u
s
s
i
5
/
0
o
N
,
s
u
o
u
c
s
i
m
o
r
P
.
I
I
I
V
y
r
n
e
H
f
o
e
t
i
r
o
v
a
F
a
/
n
e
u
s
s
I
o
N
)
s
n
o
s
e
r
e
w
3
(
l
i
c
e
C
m
a
i
l
l
i
W
f
o
r
e
h
t
a
F
I
I
I
V
y
r
n
e
H
f
o
d
n
e
i
r
f
e
s
o
C
l
.
)
n
e
r
d
l
i
h
c
e
t
a
m
i
t
i
g
e
l
l
i
(
e
k
a
r
)
8
4
5
1
(
8
5
e
g
a
t
a
d
e
i
r
r
a
M
l
;
d
o
h
e
s
u
o
h
f
o
r
e
r
u
s
a
e
r
t
,
r
e
i
t
r
u
o
C
r
e
t
h
g
u
a
d
e
n
o
s
n
o
s
5
%
0
%
0
%
0
2
5
/
0
4
/
0
5
/
1
5
4
8
3
5
0
0
5
4
4
1
2
4
1
1
2
1
1
1
1
S
E
T
O
N
S
S
O
L
H
T
R
I
B
L
L
I
T
S
R
O
I
D
E
V
V
R
U
S
S
E
V
W
I
F
O
E
T
A
R
S
E
I
C
N
A
N
G
E
R
P
N
I
I
G
N
T
L
U
S
E
R
Y
C
N
A
N
G
E
R
P
I
E
G
A
R
R
A
C
S
I
M
S
E
I
B
A
B
S
E
T
A
D
I
L
A
C
G
O
L
O
N
O
R
H
C
(
)
R
E
D
R
O
7
4
5
1
–
3
8
4
1
8
2
5
1
–
2
8
4
1
5
4
5
1
–
4
8
4
1
n
o
t
p
m
o
C
m
a
i
l
l
i
W
n
o
d
n
a
r
B
s
e
l
r
a
h
C
r
r
a
P
m
a
i
l
l
i
W
S
E
M
A
N
0
4
5
1
–
5
8
4
1
l
l
e
w
m
o
r
C
s
a
m
o
h
T
2
1
5
1
–
5
8
4
1
2
3
5
1
–
9
8
4
1
t
t
e
v
y
n
K
s
a
m
o
h
T
d
r
o
f
d
l
i
u
G
y
r
n
e
H
)
x
e
(
3
5
5
1
–
5
9
4
1
9
3
5
1
–
6
9
4
1
w
e
r
a
C
s
a
l
o
h
c
i
N
l
i
c
e
C
d
r
a
h
c
i
R
9
4
5
1
–
3
9
4
1
w
e
r
a
C
d
n
o
m
y
W
0
5
5
1
–
0
9
4
1
c
n
a
y
r
B
s
i
c
n
a
r
F
)
d
e
u
n
i
t
n
o
C
(
2
e
l
b
a
T
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
o
n
;
d
n
2
y
a
m
y
r
n
e
H
(
n
y
e
l
o
B
y
r
a
M
o
t
d
e
i
r
r
a
M
d
a
h
s
n
o
s
s
i
h
(
t
e
s
r
e
m
o
S
f
o
e
k
u
d
t
s
1
)
g
n
i
r
p
s
f
f
o
w
e
f
y
r
e
v
o
n
t
u
b
m
e
h
t
d
e
r
e
h
t
a
f
e
v
a
h
8
2
e
g
a
d
e
i
D
.
)
e
c
n
e
d
i
v
e
n
y
e
l
o
B
e
n
n
A
h
t
i
w
e
v
o
l
n
i
(
t
e
o
P
)
s
0
2
5
1
n
i
)
t
i
a
r
t
r
o
p
n
i
e
b
o
H
l
(
r
e
i
t
r
u
o
c
i
t
n
e
n
m
o
r
P
I
I
I
V
y
r
n
e
H
y
b
s
r
o
n
a
m
l
a
r
e
v
e
s
d
e
t
n
a
r
G
t
t
a
y
W
o
t
d
e
t
a
l
e
R
.
P
J
,
P
M
,
r
e
i
t
r
u
o
C
)
h
t
e
b
a
z
i
l
E
r
e
d
n
u
r
e
h
t
r
u
f
e
s
o
r
(
n
a
i
c
i
t
i
l
o
p
d
n
a
r
e
i
t
r
u
o
C
P
M
.
s
r
e
h
t
o
d
n
a
I
I
I
V
y
r
n
e
H
o
t
r
e
i
t
r
u
o
C
.
c
t
e
r
e
i
t
r
u
o
C
%
8
%
0
%
0
%
0
%
0
%
0
%
0
%
0
%
0
r
e
h
(
n
y
e
l
o
B
y
r
a
M
e
f
i
w
t
s
1
%
7
1
)
e
u
s
s
i
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
2
1
/
1
2
/
0
4
/
0
1
1
/
0
8
/
0
9
/
0
5
1
/
0
0
1
/
0
6
/
1
4
/
0
1
1
2
4
9
1
1
8
+
4
3
1
0
1
5
2
1
1
1
2
2
1
2
1
2
)
x
e
(
2
5
–
0
0
5
1
r
u
o
m
y
e
S
d
r
a
w
d
E
8
2
–
0
0
5
1
y
e
r
a
C
m
a
i
l
l
i
W
2
4
5
1
–
3
0
5
1
t
t
a
y
W
s
a
m
o
h
T
7
6
5
1
–
0
1
5
1
9
4
5
1
–
0
1
5
1
9
7
–
0
1
5
1
6
9
5
1
–
4
/
1
1
5
1
9
3
5
1
–
6
7
4
1
6
5
5
1
–
0
0
5
1
0
2
5
1
–
?
z
t
n
y
o
P
n
o
c
a
B
e
e
L
s
a
l
o
h
c
i
N
y
n
o
h
t
n
A
s
a
l
o
h
c
i
N
y
n
n
e
D
d
n
u
m
d
E
s
y
l
l
o
n
K
s
i
c
n
a
r
F
n
o
t
l
e
h
S
n
h
o
J
d
r
o
f
f
a
t
S
m
a
i
l
l
i
W
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
172
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
may not have been as carefully recorded as those for royals, but
the success rates (the survival of children past the age of about
two) are capable of reasonable estimation. The study is restricted
to children born within marriage due to the lack of consistent data
about illegitimate pregnancies; early methods of contraception are
irrelevant in these cases since the production of heirs in both royal
and noble families was paramount.16
The eminent Howard and Seymour families (which both sup-
plied Henry with a wife) serve as prime examples, as can other known
courtiers and colleagues of Henry for whom detailed information is
available. Results show that among thirty-one noblemen closely as-
sociated with Henry, the mean number of children fathered was 5.6;
only 18 of 179 documented pregnancies (10.05 percent) resulted in
either miscarriage or stillbirth. Thomas Howard, third duke of Nor-
folk (1473–1554), uncle and judge of Anne Boleyn, who was one of
sixteen siblings and step-siblings, produced eight children from two
wives. Edward Seymour, first duke of Somerset (1500–1552) had
twelve children by two wives (one baby died in infancy). Staying
at Wolf Hall, the Seymour country seat, Henry commented that
Seymour’s ability to father so many children was unfair, given that
he, the king, had so little success.
Tables 1 and 2 show that Henry had significantly fewer surviving
children than his married and “active” courtiers and colleagues,
with a success rate of only 30 percent (three survivors among his
ten legitimate pregnancies). According to column 4 of Table 2,
even if the records of the miscarriages and stillbirths of courtiers
are incomplete, and their illegitimate births unrecorded, Henry un-
deniably produced far fewer offspring than did his contemporaries,
in spite of his multiple partners. The pregnancy/fertility success
rates (as reasonably estimated in column 7) are generally much higher
for others than for him. All members of the royal court would
have had a generally similar lifestyle, with or without Henry’s
16 Bartlett, Blood Royal, 52–88. Rudimentary contraception was available at the time but
unlikely to have been deployed in families that desired large families with male heirs (and
females to clinch family alliances). For discussion of herbal medications, leather/gut condoms,
lemon cups as “caps,” etc. (all contrary to Catholic and Protestant dogma), see Lesley Smith,
“Contraception in the 16th Century,” Journal of Family Planning and Reproductive Health Care,
XXXII (2006), available at https://srh.bmj.com/content/32/1/59; Angus McLaren, History of
Contraception: From Antiquity to the Present Day: Family, Sexuality & Social Relations in Past Times
(Oxford, 1992).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
M I S C A R R I A G E S A N D MA L E I N F E R T I L I T Y
| 173
well-known excesses. Furthermore, early death or late marriage are
ready explanations for why some of his contemporaries had few
documented children; infertility was not the issue for them.17
MALE FERTILITY FROM PLATO TO THE SEVENTEENTH CENTURY As
already mentioned, male reproductive failure throughout history
has usually been attributed to a lack of sexual prowess or impo-
tence; the ridicule that affected men feared that they might receive
for sexual inadequacy resulted in a taboo on any discussion of the
subject. Plato, in the Republic (Book III, 415B ff ) drew attention to
how “the best men must cohabit with the best women in as many
cases as possible and the worst with the worst in the fewest.” The
need for “young men who excel” to “beget as many children as
possible” (Republic, Book V, 460B) indicated a recognition that
some males reproduced more effectively than others. In the medi-
eval period, the idea that a man might be sexually inadequate sur-
faced in the “fops” that Geoffrey Chaucer and, later, William
Shakespeare described, indicating men with impaired sexual per-
formance, with no consideration of male infertility. The ability of
a man to perform removed any doubt about his fertility, leaving
reproductive failure exclusively as the fault of women.18
Rider’s work on male/female fertility and infertility in the
Middle Ages provides some evidence that the male role attracted
little more consideration beyond mere performance. In the six-
teenth century, dramatic medical progress ensued after the legali-
zation of human dissection for anatomical purposes, the revival of
work by the Roman physician Galen, and the new ideas of Vesa-
lius. But as Evans highlights, not until the seventeenth century did
the first detailed discussions and descriptions of male infertility
emerge in England, particularly by the surgeon John Tanner in
his The Hidden Treasures of the Art of Physick (1659). Tanner still
regarded the role of women in pregnancy failure as dominant,
but he addressed male infertility as distinct from erectile function,
17 Edmund Tudor, Edward Howard, and William Carey, for example, all died relatively
young (around the age of thirty) and thus were not sexually active for long. Francis Bryan,
although known as a promiscuous “rake,” did not marry until age fifty-eight. Judging from
portraits, only one courtier (Henry Guildford) looks significantly overweight; Cromwell just
looks heavy.
18 Olwen Hufton, The Prospect Before Her: A History of Women in Western Europe 1500–1800
(New York, 1995), 177.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
174
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
thus initiating the recognition of male infertility as a condition
requiring identification and treatment. The present study comple-
ments these historical descriptions by analyzing Henry’s predica-
ment in the context of contemporary noblemen with similar
lifestyles.19
Henry’s marital and reproductive history had a pivotal effect
on English history and the Reformation, the repercussions of
which persist to this day. By using multiple sources of historical
data, with the observations about the miscarriages and/or stillbirths
that plagued Henry’s multiple female partners, the evidence points
to Henry unknowingly suffering from male infertility. The risk of
poor nutrition in matters of fertility is no secret nowadays, whether
in several developing countries (with some conditions not unlike
those of sixteenth-century England) or anywhere else where people
indulge in excessive meat and carbohydrate intake and avoid fruits,
legumes, and vegetables.
Obesity, physical infirmity, diabetes, and sexually transmitted
infections can reduce the quality of sperm, either blocking preg-
nancy or auto-aborting it; malnutrition, poor sanitation, and infec-
tions can lead to foetal or neonatal death. Poor sperm quality is an
especially under-appreciated cause of miscarriage in contemporary
times.
MEDICAL RESEARCH Despite the evidence, the limitations of this
study make it impossible to prove conclusively that Henry was in-
fertile. Chance or the highly unlikely coincidence that Henry mar-
ried six women with fertility problems are not outside the realm of
possibility. The unusual preponderance of bad pregnancy out-
comes, or no pregnancy at all, involving multiple female partners,
however, strongly implicates Henry as the source of the problem,
regardless of the numerous pregnancies for which he was also partly
19 Evans, “‘They Are Called Imperfect Men’: Male Infertility and Sexual Health in Early
Modern England,” Social History of Medicine, XXIX (2014), 311–332; John Tanner, The Hidden
Treasures of the Art of Physick (1659), 346, as cited by Evans, “‘They Are Called Imperfect
Men,’” 311. For miscarriage and the demographics of stillbirth and childlessness in the early
modern period, see Evans and Read, “‘Before Midnight She Had Miscarried’: Women, Men
and Miscarriage in Early Modern England,” Journal of Family History, XL (2015), 3–23; Helen
Berry and Elizabeth Foyster, “Childless Men in Early Modern England,” in idem (eds.), The
Family in Early Modern England (New York, 2007), 158–183; Chris Galley, “The Stillbirth
Rate in Early Modern England,” Local Population Studies, LXXXI (2008), 75–83, the
seventeenth-century focus of which shows the importance of further research on the Tudor period.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
M I S C A R R I A G E S A N D MA L E I N F E R T I L I T Y
| 175
responsible. Not until the modern era has research been able to dis-
cover that sperm health plays a significant role in miscarriage and
that the causes of miscarriage, stillbirth, and neonatal death do
not lie with women alone. The results of this study demonstrate
for the first time that Henry’s peers and their wives were far less
affected by infertility and pregnancy loss, strongly indicating,
ironically, that Henry’s infertility led to his wives’ difficulties with
pregnancy.
Paternally imprinted genes contribute heavily to the regula-
tion of the placentation that is critical to embryo viability. Further-
more, adverse sperm characteristics such as reduced sperm count,
low percentage of amotile and progressively motile sperm, elevated
sperm DNA fragmentation, and semen reactive oxidative species
(ROS) are known to be associated with male infertility and RPL.
Clinical risk factors such as obesity and diabetes mellitus increase
the risk of male infertility. Because no pharmacological therapies
are available to improve sperm quality, the customary treatment
of male infertility is to provide IVF or ICSI to the female partners
of affected men. A recent qualitative study found that men with
infertility problems often fall prey to a social stigma of being “less
of a man” while engaging in treatment. Participants also sometimes
complain of a lack of support from professionals and family
members, leading to further adverse emotional reactions. Al-
though male infertility affects 10 percent of the male population,
it has no major public role models and still carries an aura of social
exclusion.20
This interdisciplinary study raises issues that are relevant for the
public—patients and medical professionals alike. Henry VIII by
all accounts suffered from male infertility, but no such diagnosis
existed at the time. Although male infertility has now acquired a
distinct etiology, it remains a taboo subject. Health-care and re-
search programs targeting male infertility remain underdeveloped
when compared with those oriented toward female fertility, which
Jan Tesarik, Ermanno Greco, and Carmen Mendoza, “Late, but Not Early, Paternal Ef-
20
fect on Human Embryo Development Is Related to Sperm DNA Fragmentation,” Human
Reproduction, XIX (2004), 611–615; Imam et al., “Idiopathic Recurrent Pregnancy Loss”;
Henkel et al., “Influence of Deoxyribonucleic Acid Damage”; Jayasena et al., “Reduced Tes-
ticular Steroidogenesis and Increased Semen Oxidative Stress in Male Partners”; Arya and
Dibb, “Experience of Infertility Treatment.”
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
176
| V A L E RI E SH R I M P LI N AND C H A N N A N . J A Y A S E N A
have led to such breakthroughs as IVF therapy. Increased recogni-
tion of the importance of male infertility to human health deserves
increased recognition, diagnosis, and treatment to ensure that af-
fected couples receive proper support. Furthermore, maybe the
knowledge that Henry VIII, one of the most powerful rulers in
European history, was almost certainly affected by this condition,
will alleviate the emasculation and social stigma that is still attached
to male infertility.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
e
d
u
/
j
i
/
n
h
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
5
2
2
1
5
5
1
9
5
9
9
3
0
/
j
i
n
h
_
a
_
0
1
6
9
5
p
d
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3