Gautam Ivatury, Jesse Moore, and Alison Bloch
A Doctor in Your Pocket
Health Hotlines in Developing Countries
Afiya lives in the rural Sylhet region of Bangladesh. For two days, her youngest
daughter, Rubina, has been complaining of fatigue and has felt warm to the touch.
Taking the child to the nearest clinic would cost Afiya a day’s lost wages, round-trip
bus fare, and clinic fees of Taka 200 (U.S. $3). Instead, Afiya and her husband use the family’s mobile phone to dial “7-8-9,” the Healthline hotline service set up by TRCL, Ltd., a telemedicine firm, and GrameenPhone, the country’s largest mobile network operator. The family quickly reaches Dr. Quadri at Healthline’s call center in Dhaka. After asking a few questions, Dr. Quadri tells her to give Rubina small regular doses of paracetamol, available at neighborhood shops. For the three- minute call, Afiya pays only Taka 15 (U.S. $0.21) from her family’s GrameenPhone
prepaid talk-time balance.
Afiya is not the only person seeking basic medical advice and information by
calling a health hotline. Telephone-based nurse triage, primary care, and health
information have been offered in developed countries since the late 1990’s, and
Gautam Ivatury is a founder of Signal Point Partners, an investment and advisory
company for mobile services in emerging markets, and a Strategic Advisor to CGAP,
the global microfinance resource center housed at the World Bank. Between 2003 and
2008, Gautam led CGAP’s work in microfinance and technology, including a flagship
program co-funded by the Bill and Melinda Gates Foundation.
Jesse Moore is Director of the GSM Association’s Development Fund, with a specific
focus on mServices. Previously, Jesse worked with Vodafone on M-PESA, a mobile
payment service targeting Kenya’s un-banked population. From 2002 to 2006, he
founded and directed CARE Enterprise Partners, the division of the large NGO CARE
that provides venture capital to businesses in the developing world.
Alison Bloch is the mHealth Advisor at the GSM Association’s Development Fund,
where her focus is to accelerate the market for commercially and socially viable mobile
health solutions. She recently graduated from the University of California, Berkeley
with an MBA and a Masters in Public Health, with a concentration in technology.
Alison has received a fellowship through the Blum Center for Developing Economies
to work on health care based ICT initiatives in the developing world, and most recent-
ly worked on mHealth projects in East Africa and Haiti.
© 2009 Gautam Ivatury, Jesse Moore, and Alison Bloch
innovations / winter 2009
119
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
today are available to about 150 million people in the United States, Britain,
Australia, Canada, New Zealand, and elsewhere.1 More recently, health hotlines like
Healthline have emerged in developing countries, and have already been used by
more than 10 million people in Mexico, India, Pakistan, and Bangladesh.2 New
hotlines are being set up in the Middle East, the Caribbean, Latin America, and
Southeast Asia.
Health hotlines are medical call centers that provide health-related informa-
tion, advice, referrals, and sometimes prescriptions to individual callers over a
phone line. Callers are connected to health professionals (nurses, paramedics, or
physicians), who usually follow standard protocols to assess medical situations and
provide information and advice.
Now that there are more than four billion mobile connections3—most in
developing countries—health hotlines accessible to mobile phone subscribers can
bring basic health information and care even to people in sparsely-populated or
low-income areas where there are few health care facilities and doctors. Fifty-five
percent of calls to Healthline in Bangladesh are from rural areas, and 77 percent of
callers are women. Of rural callers, 81 percent are women, of whom two-thirds are
calling about their children’s health.4
The GSM Association—the global trade association for mobile network oper-
ators—and its Development Fund believe that health hotlines can transform
health care for poor people just as mobile phones are revolutionizing financial
services (“mobile money”). Health hotlines are simple to understand (“call a doc-
tor”), provide immediate assistance, and are available to anyone with a mobile
phone. The reach and branding of a mobile network operator (MNO), and the
scalability of call-center technology may mean that health hotlines serve vast num-
bers of people in the coming years.
As a first scan of the approach, this report tracks hotlines operating in devel-
oping countries, assesses their social and commercial success to date, and offers
industry bodies, and development agencies to
suggestions for governments,
advance this approach.
In the next section we define the health hotline model and present a brief land-
scape of health hotlines in operation today. Section 3 spotlights four of the most
prominent health hotlines in developing countries and compares their business
approaches. In Section 4 we assess their commercial viability and potential for
growth, and in Section 5 we evaluate their potential for social impact. Finally,
Section 6 offers thoughts on how development agencies and governments can sup-
port the health hotline phenomenon.
Our findings are largely based on visits to and interviews with four health hot-
lines in developing countries, as well as on secondary research and phone inter-
views with academics and technology vendors. The four health hotlines we stud-
ied in depth are:
• Healthline (Bangladesh)
• Teledoctor (Pakistan)
• HMRI (India)
120
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
Figure 1. A doctor answering calls at MedicallHome in Mexico.
• MedicallHome (Mexico)
These hotlines, three of them private and for-profit services, and the fourth a
public not-for-profit service, emerged from the health care, call center, technology,
and mobile phone industries. Each provider has partnered with health care com-
panies or professionals, government agencies, and fixed-line or mobile network
operators to develop its service.
THE HEALTH HOTLINE MODEL: PHONE-BASED PRIMARY CARE
Defining Health Hotlines
We define a health hotline as a service whose main goal is to provide medical
advice and information over the telephone, and which has the following four char-
acteristics:
• It primarily gives information to callers who are individual patients, but may
also serve medical personnel or health workers.5
• It delivers information to callers mainly through a voice call, over the caller’s
wireless or land line telephone connection.
• It is primarily inbound, meaning that the service receives many more calls than
it makes; the limited number of outbound calls may be for follow-up or
reminders.
• Callers may be anywhere, and need not be at a specific location, such as a
innovations / winter 2009
121
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
telemedicine center, a health clinic, or with a health worker.
Health hotlines provide some or all of the following information and services
to callers:
Medical information, including the location and availability of nearby hospi-
tals, clinics, laboratories, or other facilities;
Triage: identifying whether the caller should be directed to emergency, admin-
istration, or medical consultation services;
Consultation: discussing the caller’s condition with him/her as a first line of
care ;
Diagnosis: determining the caller’s health issue based on information gathered;
Referral: “pushing” the caller to the next level or type of health service, such as
an in-person consultation at a clinic;
Treatment: recommending the next step in terms of care, such as prescribing
medications, prescribing care by another health care provider, or prescribing a
plan of action for the caller or the caller’s caregiver;
Counseling: providing support and encouragement to callers with specific
mental or physical ailments;
In some instances, discount purchasing, or access to special pricing for private
medical care or prescriptions.
Our definition draws clear boundaries between health hotlines and other
health services that make use of a mobile phone. Because anyone is eligible to call
the health hotline, we exclude medical call centers that are dedicated to specific
employers or that offer after-hours triage for patients of a specific physician’s prac-
tice. Because callers can be anywhere, we exclude telemedicine programs that
require callers to visit rural kiosks where they are connected to doctors via video
and/or voice. And by including only services that are predominantly inbound (that
receive more calls than they initiate), we exclude public health data collection and
health awareness initiatives that use mobile phones to gather information or to
push public health messages with textmessaging and voice calls.
The Health Hotline Landscape
For over a decade, call centers have been used for telemarketing, customer support
and other business functions, although the practice is on average six to eight years
old in the developing world.6 But staffing call centers with doctors or other med-
ical personnel to create health hotlines is a relatively more recent phenomenon in
these markets.
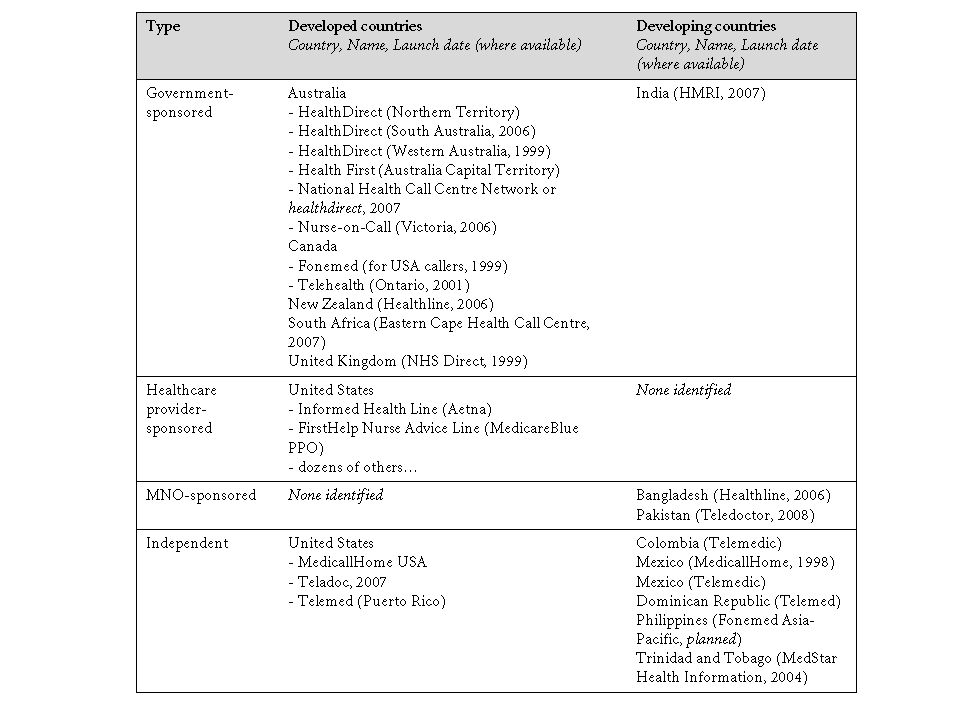
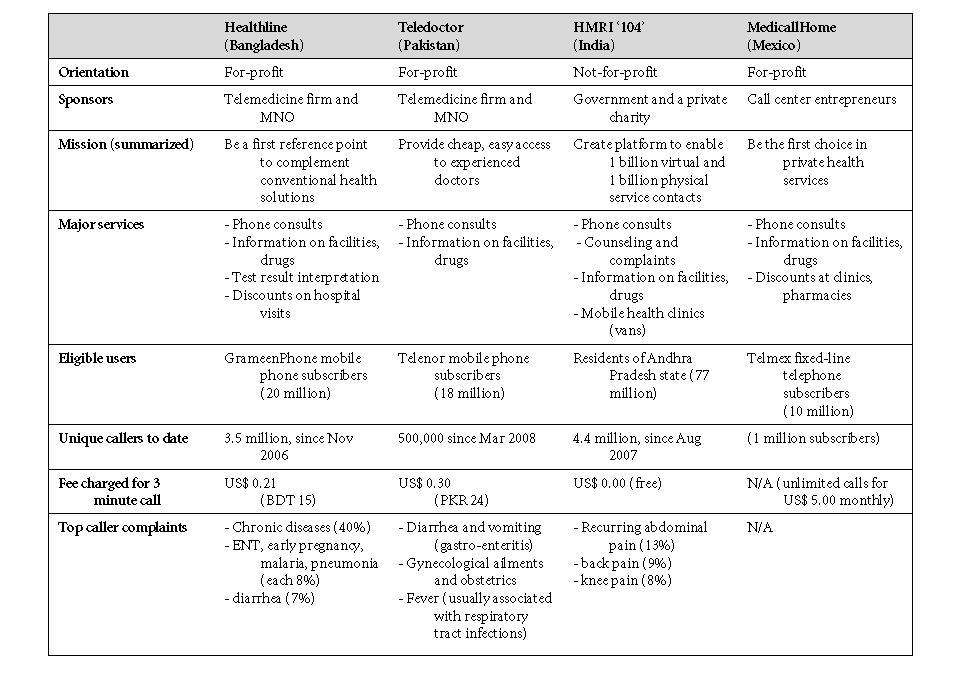
As Table 1 shows, health hotlines may be sponsored by a government, a health-
care provider, or an MNO, and some are independent.7 Sponsoring does not imply
that the MNO or government is putting up all the funding, is operating the serv-
ice, or is even the lead partner in it. Rather, by sponsoring we mean acting as the
“public face” of the initiative.
Government-sponsored hotlines. In general, these are designed to supplement
existing public health facilities and reduce the total cost of care to the public health
system. HMRI in India was set up as a public-private partnership between the state
122
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
.
8
0
0
2
r
e
b
m
e
c
e
D
,
s
e
n
i
l
t
o
H
h
t
l
a
e
H
n
w
o
n
K
.
1
e
l
b
a
T
innovations / winter 2009
123
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
government of Andhra Pradesh and the Satyam Foundation. Although it is not a
government agency, its services are promoted publicly as initiatives of the state
government, under the Rajiv Arogyasri scheme of the central government. The
state government covers 95 percent of direct ongoing costs, and Satyam
Foundation covers 5 percent.
Healthcare provider-sponsored hotline. In developed countries, after-hours
nurse triage services or pediatric nurse hotlines are set up by hospitals, private
physician practices, health maintenance organizations, and insurance companies
to supplement in-person care, reduce unneeded visits, and lower costs.
Mobile Network Operator (MNO) sponsored hotlines. Although Healthline in
Bangladesh and Teledoctor in Pakistan are managed independently by telemedi-
cine companies, these firms promote their health hotlines jointly with MNOs to
gain retail access to individual consumers, collect payments, and leverage the
MNOs’ consumer brand recognition.
Independent hotlines. These hotlines are not affiliated with a specific health care
provider, MNO, or other group. All of the independent health hotlines listed in
Table 1, including MedicallHome in Mexico, were set up in conjunction with
Fonemed, a U.S.-based provider of software and triage protocols to medical call
centers globally. MedicallHome acquired a competitor in Mexico in 2008, elimi-
nating the one independent hotline not affiliated with Fonemed.
All hotlines we identified in developing countries, except HMRI in India, are
MNO-sponsored or independent, while those in developed countries tend to be
sponsored by governments or health care providers. As a result, health hotlines in
developing countries tend to have three characteristics:
• They are for-profit, instead of not-for-profit.
• They market their services directly to individual consumers and charge them,
instead of charging governments, health insurance companies or employers.
• They partner with MNOs or other telecom firms that have a wide retail pres-
ence, brand recognition, and substantial billing and revenue collection systems.
HEALTH HOTLINES IN DEVELOPED COUNTRIES
Health hotlines have a longer operating record in Australia, Canada, and Britain
than in developing countries, although most offer telephone triage by nurses
rather than consultations with physicians. Studies that track the dominant govern-
ment and health care provider sponsored hotlines in developed countries seem to
offer several main findings:
• Health hotlines receive large numbers of calls. Western Australia’s HealthDirect
health hotline, launched in May 1999 as the first in the country, had over 1.4
million calls a year by December 2006. This is an impressive figure considering
that the state’s population is only 2.1 million.8 Furthermore, about 10 percent
to 15 percent of all calls received were from rural parts of the state in the first
12 months that the service was available there.9 In the UK, NHS Direct took
five million calls in 2007.10
124
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
• Most callers are women and mothers. Between 2001 and 2006, 40 percenr of
callers to Ontario’s Telehealth service were mothers asking about their children’s
symptoms.11 In the UK, 60 percent of callers to NHS Direct are women.12
• A significant percentage of calls result in self-care. According to Ontario’s
Ministry of Health and Long-Term Care website, 43 percent of callers received
advice on self-care, 35 percent were advised to visit a physician, and only 16
percent were considered urgent.13
• Most callers report being satisfied with the service. In New Zealand, 97 percent of
callers surveyed in an independent evaluation said they were very satisfied or
satisfied with their Healthline contact, and 98 percent said they would call
again.14 In the UK, 95 percent of callers to NHS Direct rated the care and serv-
ice as “excellent,” according to the service’s customer satisfaction surveys.15
• Evidence of cost savings to general practitioners (GPs) and public health services is
mixed. In a rural New Zealand pilot, two-thirds of calls to Healthline were
made after hours, and two-thirds of these were triaged to a low level of care
that did not require calling the rural clinic’s on-duty doctor.16 Similarly, a three-
year study in Australia found that use of telephone triage seemed to have
reduced GP claims for after-hours service.17 But the UK’s NHS Direct faces con-
sistent criticism that its cost per call (estimated at £16.54 at the end of March
2008) is too high relative to the cost to the National Health Service of a GP visit
(£20 to £25).18
• Employers and insurers in the U.S. seem to save with health hotlines. Between
them, Fonemed and Intellicare—the two major U.S.-based medical call center
providers—have more than a thousand healthcare facilities and insurers as
clients.
• Callers generally accept and follow the advice given. A study of a telephone triage
service among several hundred uninsured people in Kansas found that 98 per-
cent of callers agreed with the advice given, and 90 percent reported following
up on the advice given.19 In France, 70 percent of callers to the Grenoble uni-
versity hospital hotline complied with the medical advice given. Compliance
was 61% among patients who were advised to treat themselves, 84 percent
among patients who were advised to consult a general practitioner during busi-
ness hours, and 64 percent among patients who were advised to go to the
emergency department.20
Health hotline providers also contend that proper information, provided at the
right times, can dramatically reduce the overall cost associated with health care.
Informed individuals can prevent adverse health outcomes, treat some conditions
themselves, and make the right decisions during medical emergencies. Health pro-
fessionals, with the right information, can make better decisions on triage and
diagnosis and give patients a better understanding of their conditions. All of these
actions can reduce the cost of health care and improve its quality.
Still, the health hotline delivery model is not a full substitute for traditional, in-
person modes of health information delivery. Several factors also limit the ability
innovations / winter 2009
125
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
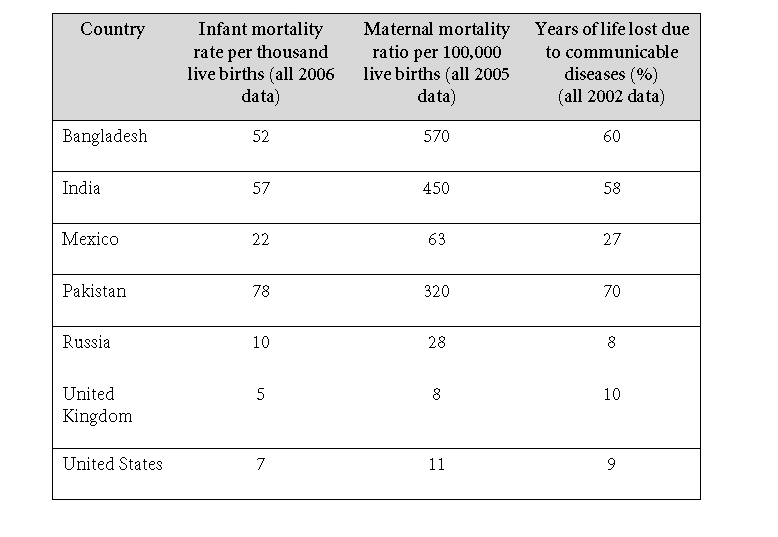
Table 2. Sample Health Indicators, Selected Countries.
Source: World Health Organization Statistical Information System (WHOSIS),
The three indicators are often used to monitor progress against the health-related
Millennium Development Goals established by the United Nations. Goal 4 is to
reduce child mortality, Goal 5 is to improve maternal health, and Goal 6 is to com-
bat HIV and AIDS, malaria, and other diseases.
of health hotlines to provide information and advice to callers. First, some callers
require in-person consultations, prescription drugs, or other treatments that may
not be affordable even if they are available nearby. In these cases, having diagnosed
the patient’s ailment, the hotline can do little else.
Second, health hotlines have limited ability to follow up with callers to under-
stand the results of their information and advice. Patients do not regularly call to
report the results after they complete a course of treatment or act on the hotline’s
advice. This makes it difficult for hotlines to judge how successful their interven-
tions have been and how to adapt their protocols or recommendations. If any-
thing, the patient is more likely to call back if the advice or prescription has not
worked.
Rationale for Health Hotlines in Developing Countries
The poor state of health care systems and outcomes in developing countries is
widely documented (Table 2).
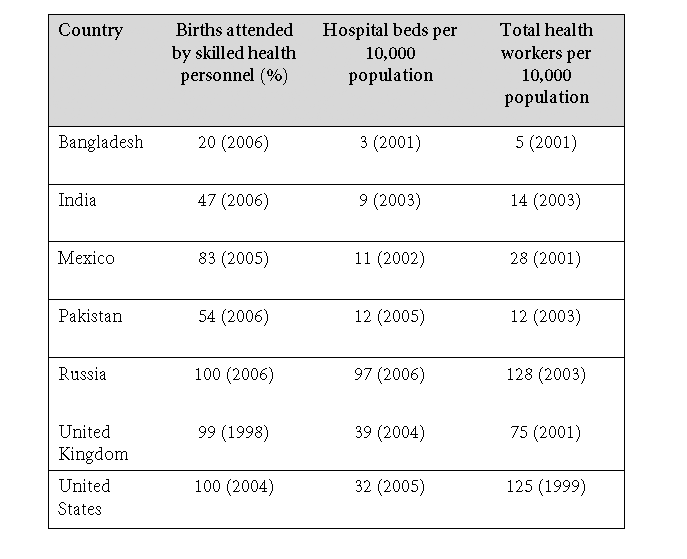
The poor state of the health care infrastructure in developing countries is at
the root of these disparities; Table 3 provides some examples. Seven characteristics
apply to the health care delivery systems in these countries.
126
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
Table 3. Sample Health System Indicators, Selected Countries.
1. They lack primary care physicians or other health professionals. Developing
nations continue to face a shortage of health care workers, particularly in remote
and rural areas. Individuals and governments do not have the resources, either
financial or academic, to properly train and develop health professionals.
2. People lack the financial resources to consult better quality providers.
Physicians, especially specialists, are often located in urban areas and tend to be
quite costly because of the high demand for their time and services. Increasingly,
higher-level health practitioners are migrating to wealthier regions because they
can earn more for their work, creating a brain drain. This raises the cost of access-
ing a physician or specialist for people in poor and rural communities.
3. Going to a health facility has a high effective cost. “A recent study conducted
by the Indian Institute of Public Opinion found that 89% of rural Indian patients
have to travel about 8km to access basic medical treatment and the rest have to
travel even farther.” 21
4. Primary health care facilities are of low quality and personnel are often not
highly skilled. The lack of infrastructure in rural health care facilities makes it dif-
ficult to attract and retain qualified professionals. A quality assessment of 44 ran-
domly selected rural private practitioners in Maharashtra, India, found that only
20 percent of the practitioners recorded the patient’s blood pressure, only 30 per-
cent recorded their temperature, and none recorded a provisional diagnosis. Only
innovations / winter 2009
127
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
Table 4. Health Hotline Solutions to Information Constraints.
20 percent explained the prescription to patients.22
5. People lack basic information about the location and availability of pharma-
cies, clinics, and laboratories, and about prescription medicines. No formalized dis-
tribution or supply-chain systems lead to pharmacies stocking key medicines and
medical supplies. In addition, few if any drug regulatory agencies or protocols are
in place to guarantee that drugs are accurately compounded or that they actually
are produced.
6. People widely consult with informal, sometimes traditional, health care
providers who may not be trained or ethical (e.g. quacks). India boasts top specialty
clinics and hospitals, yet is also plagued by practitioners who falsely claim expert-
ise. “Quacks” provide health consultations and medications in lieu of public
providers, but are notorious for misdiagnosing illnesses and prescribing the wrong
and potentially harmful medication to patients.
128
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
.
s
r
e
d
i
v
o
r
P
e
n
i
l
t
o
H
h
t
l
a
e
H
.
5
e
l
b
a
T
129
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
7. People perceive that they cannot have privacy if they attend a neighborhood
clinic or physician. This perception varies, depending on the culture of a given
region, but it is often an issue for those dealing with issues of sexual health and dis-
eases that have social stigmas attached to them, such as HIV/AIDS.
Even where providers make a special effort to extend public health services to
underserved communities, the poor often continue to prefer to visit more expen-
sive private facilities. The All India Institute of Medical Services (AIIMS) offers a
mobile health clinic in the slums of New Delhi; an evaluation found that more
than two-thirds of respondents (70.5%) to a community survey preferred private
practitioners or private hospitals, and far fewer (12.9%) preferred the mobile clin-
ic. Reasons for this preference included more faith in private practitioners, the clin-
ic’s inconvenient schedule, and long wait times at public facilities and the mobile
clinic.23
Poor information also leads to poor health care outcomes. Individuals spend
time and money to go to the doctor because they don’t know that the condition
doesn’t warrant it, or they travel long distances only to find that a health care
provider is unavailable. Public clinics triage a large number of patients who didn’t
know that a visit was unnecessary, sometimes making people with more serious
ailments wait. In addition, health workers and caregivers in rural areas do not have
the depth of knowledge to address many complaints, but they have no backup or
peer from whom they can get advice.
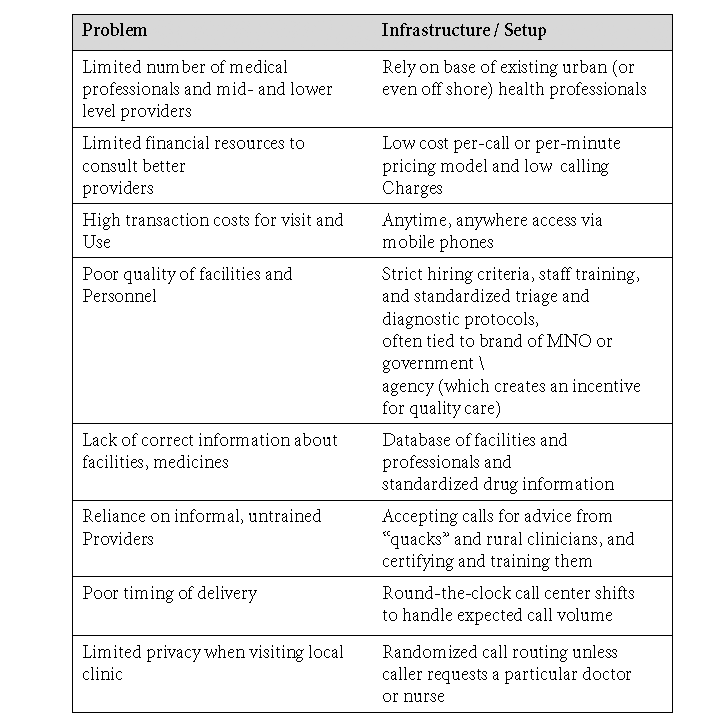
How health hotlines can help
By making each telephone a possible “touchpoint” where people can access quali-
ty health information, a health hotline creates a low-cost, widespread infrastruc-
ture model for the delivery of health information and solves several of the con-
straints described above. We have summarized these solutions in Table 4.
Mobile network operators, which have played a key role in developing health
hotlines in Pakistan and Bangladesh, provide key functions in developing this
infrastructure. In many markets, MNOs have the largest retail penetration of any
private enterprise. They also rank highest in brand recognition, and can deploy
tremendous financial resources to setup new services. More than four billion
mobile phone connections are now active, making it possible for even the very
poor (many of whom use mobile phones today) to access health hotlines.
Perhaps most important, MNOs have established mechanisms for billing and
collecting revenue in tiny increments. For health hotlines that wish to reach the
broadest possible customer base, simple ways of collecting revenue are essential.
Virtually nothing is more commonly traded in developing countries, though in
small amounts, than the prepaid airtime distributed by MNOs. In India, for exam-
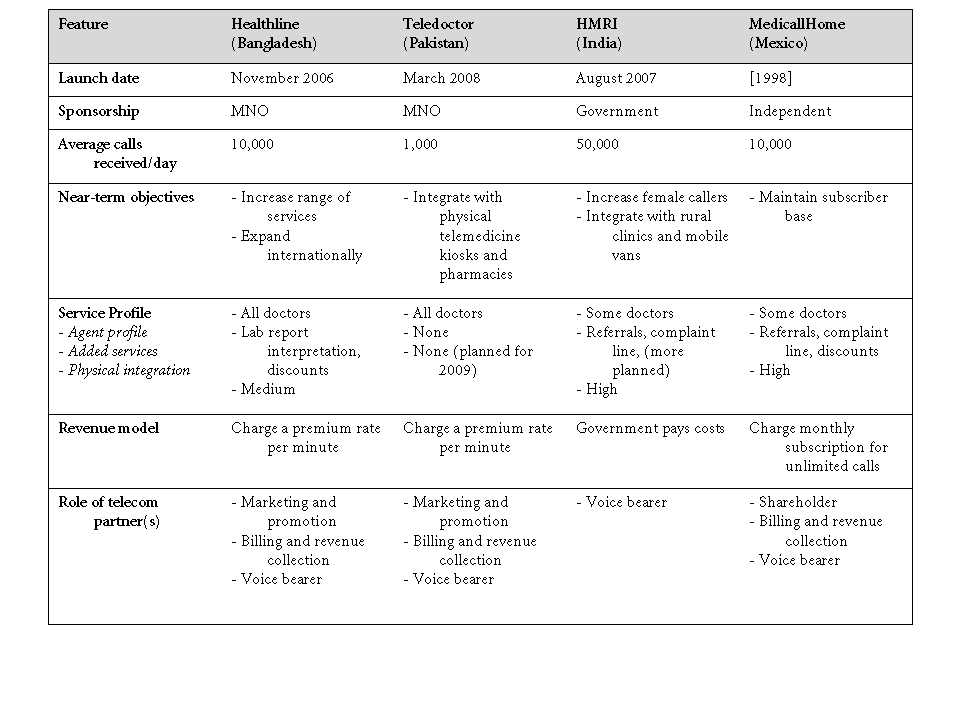
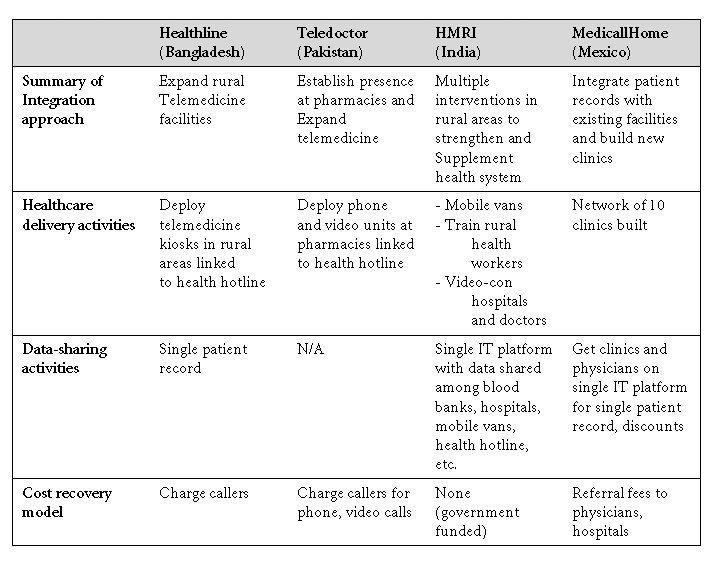
ple, a Rs. 10 (U.S. $0.20) talk-time top-up is widely available at corner stores and market vendors. By piggybacking on the MNO’s prepaid billing and account man- agement systems to charge people for using their services, health hotlines gain immediate access to millions of potential customers. The transformative power of mobile networks has been demonstrated in 130 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket . s e n i l t o H h t l a e H r u o F , s n o i s i c e D c i g e t a r t S y e K . 6 e l b a T 131 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 Gautam Ivatury, Jesse Moore, and Alison Bloch Kenya, where Safaricom (a leading MNO) has been able to attract nearly five mil- lion subscribers to its mobile money transfer service, M-PESA, in only two years. In comparison, only about five million Kenyans have bank accounts. FOUR HEALTH HOTLINE CASES To better understand the commercial viability and social impact of the health hot- line model in developing countries, we studied four hotlines in depth: Healthline (Bangladesh), HMRI (India), MedicallHome (Mexico), and Teledoctor (Pakistan) (see Table 5). In this section, we review the business approach of each hotline, and how they manage operational challenges. Business approach Understanding the business approach of each hotline can yield insights about its likely impact on social development, and its viability in the long run. In this con- text, categorizing hotlines by their type of sponsorship is useful because the spon- sor’s identity suggests the business approach of the service. It appears that three key business decisions lie at the heart of each hotline’s overall business approach: • What services will be offered to customers? • How will revenue be generated? • What partnerships with telecommunications firm(s) will be set up? How each provider makes these decisions flows from the provider’s mission, the context of its health system, and its commercial requirements—at a minimum, the need to cover costs. These questions also reflect a close parallel between the health hotline business and other mobile phone-delivered services, such as mobile phone banking. All of these businesses involve five elements: • Per-unit pricing. MNO-sponsored health hotlines charge customers per minute (as premium rate calls) or per call (for calls under three minutes, for example). • Significant costs of system setup and maintenance. Providers must invest in telecommunications and networking hardware infrastructure, and software that tracks and routes calls and/or automates triage and initial diagnosis via standard- ized protocols. • Channel partnerships. Health hotlines rely on MNOs or land line telephone companies to carry their voice and data traffic and handle billing and revenue collection. • Content partnerships. Doctors and other medical professionals are employed to give callers health information, or “premium content.” • Marketing partnerships. Hotlines co-brand their offering with mobile operators to achieve quick recognition and credibility; operators may market services as a differentiator to retain customers or promote the company’s social responsibility. Like mobile banking providers, health hotlines face the challenge of generating enough revenue to cover the ongoing costs of paying content and their channel partners and the amortized fixed costs of the technology and systems. 132 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket Table 7. Approaches to Integration with Physical Health Facilities. Table 6 summarizes the key business decisions of each of the four hotlines studied. In summary, the four hotlines seem to have made the key business decisions listed above very differently, depending on whether they are sponsored by an MNO or the government, or are independent. What is strikingly similar is the common ambition to integrate their virtual (or phone-based) service with the physical health care delivery system. All indicated that the health information service is only one piece of a larger strategy to facilitate physical health care—via telemedicine kiosks, mobile health vans, enhanced emergency transport services, or improved rural clinics. Otherwise, the revenue model and relationships with telephone companies are structured a certain way for the MNO-sponsored hotlines, and quite differently for the government-sponsored and independent hotlines (HMRI and MedicallHome, respectively). This fact seems to validate the basic typology of the hotlines pro- posed. But as health hotlines are still in an infant stage, and because they can change type, future studies may yield very different conclusions. Decision 1: What services to offer? As shown in Table 6 above, this question really has three dimensions: who, what, innovations / winter 2009 133 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 Gautam Ivatury, Jesse Moore, and Alison Bloch and how much? That is, who should be hired to answer calls: doctors, nurses, para- medics, or non-medical personnel? What services beyond basic health information should be provided? And how much integration with brick-and-mortar health facilities should be sought? The answers to these questions are remarkably similar across the four health hotlines we studied. All hotlines employ different types of “call agents”—including doctors but also nurses, paramedics, and non-medical personnel—or expect to do so in the near future. Although the founders of Healthline and Teledoctor have argued that employing doctors early in their existence has been useful in generating market trust and establishing quality service, commercial realities are coming to the fore. Both of these hotlines expect to employ non-doctors as call agents shortly, as they are more available and less costly. Call-agent salaries are the major ongoing cost that health hotlines incur. Providers must ensure that each shift at the call center has enough agents on hand, but not so many that their time is not used well. In some countries, such as Bangladesh, enough doctors are available at low enough salaries that Healthline has been able to cover costs, employing 50 doctors in shifts to handle 6,000 to 10,000 calls per day. On average, ten doctors answer calls during shifts of six or seven hours each, and are each paid about 18,000 taka (U.S. $300) monthly. In
Mexico, on the other hand, although MedicallHome pays about U.S. $1,000 a month24 to each doctor for half-time work, it keeps only 15 doctors on hand per shift as opposed to 100 non-medical call agents. Three-quarters of its calls are purely for information and not for consultation. The health hotlines are also similar in the services offered beyond health infor- mation. All of the health hotlines studied, except Teledoctor in Pakistan (the newest), offer physician referral services, discounts at hospitals and pharmacies, and interpretation of lab tests. MedicallHome in Mexico issues customers a “med- ical card” that brings discounts from five percent to 50 percent at selected clinics, hospitals, opticians, labs, and other health facilities. Healthline is now exploring the potential to generate revenue from its referral service, by developing a mobile phone based system for issuing electronic prescrip- tions and referring patients. The company envisions charging callers for the abili- ty to refer them automatically to clinics and physicians, and for issuing prescrip- tions via SMS. Finally, all of the sponsors we interviewed argued that it is imperative to inte- grate with physical health service points and facilities; phone-based information services alone are insufficient to meet all of their objectives of improving health care, especially for under-served communities. To distinguish how each hotline is approaching this task, we looked at their overall approach, their activities in healthcare delivery and data-sharing, and their cost recovery model. This analysis is summarized in Table 7. HMRI in India is perhaps the most integrated; it operates more than 100 mobile vans with diagnostic equipment that travel through rural areas each 134 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket month. It also trains and certifies rural medical practitioners and ‘quacks’ to pro- vide better in-person care, offers an emergency toll-free number and ambulance service, and maintains a customer complaint system for all public and private hos- pitals in the state. Since all of these services share a common database and technol- ogy platform, the health hotline can serve as patients’ single contact point to get information or schedule services. Decision 2: What revenue model? On a first glance at our four health hotline examples, the choice seems quite sim- ple. As described earlier, because MNOs make it possible to collect small amounts of revenue, health hotlines can charge per minute. This makes the price per call rel- atively low, and expands the potential user base for the service—including the poor. The two MNO-sponsored hotlines use exactly this revenue model to cover their costs: most callers to Healthline and Teledoctor are using their prepaid GrameenPhone or Telenor mobile subscriptions, and are therefore charged a per- minute rate. MedicallHome in Mexico proposed a similar arrangement to a leading mobile carrier, but found the price of this arrangement too high—the MNO sought 50 percent of all revenue in return for making this billing and collection system pos- sible. As a result, MedicallHome serves only those customers with land line phones, and charges a monthly subscription fee rather than a per-call amount. This arrangement is more affordable and the costs are in line with what Teledoctor and Healthline are charged by their MNOs. Because MedicallHome bills through its customers’ TelMex accounts, it inherently serves people who are middle-class or affluent. It also packages discounts at a network of pharmacies, hospitals, and clin- ics along with its health hotline services. As a result, its customers can afford to pay a monthly subscription instead of paying per call or per minute. But these are not the only two revenue models available to health hotline providers. Charging insurance companies and governments for the benefit of avoided emergency room and doctor visits may be more attractive to health hot- line providers, as it aggregates volume quickly, costs less in marketing and promo- tion, and ensures a more reliable revenue stream. Decision 3: How to partner with network operators? All four of the hotlines have relationships with mobile or land line network oper- ators—from co-owning the business to simply contracting an MNO to carry voice traffic. In general, telephone network operators (whether fixed or mobile) can offer five assets to health hotline providers: • Bearer channel(s), in this case the voice channel, for the interaction between the caller and the health hotline. All health hotlines rely on telecoms for the bearer channel—most often voice, but sometimes also text messaging for registration confirmation, sending test results, or other services. • Shortcode, an abbreviated phone number (such as 7-8-9 or 9-1-1) that cus- innovations / winter 2009 135 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 Gautam Ivatury, Jesse Moore, and Alison Bloch tomers can call instead of dialing a number that is nine or ten digits or longer. Shortcodes must be negotiated individually with each telecom so that subscribers to any telecom can dial the same number to reach the service. • Billing and revenue collection. Hotline operators find it extremely valuable to use a telecom’s billing and revenue collection system, as that lets them avoid cre- ating such a system themselves. Customers need only pay their telephone bill or have sufficient prepaid talk time to be able to call the health hotline. • Marketing and promotion. MNO-sponsored health hotlines rely on telecom companies for marketing and promotion. Teledoctor and Healthline are both branded by their MNO partners, which helps in public awareness and credibility on a national scale. • Capital. In only one case have we seen a telecom operator take an equity own- ership stake in the health hotline business. In Mexico, TelMex owns a large minority share of the MedicallHome business. In return, operators get non-financial and financial benefits from partnering with health hotline providers. From a purely financial standpoint, operators can expect incremental revenue from each subscriber, since callers to Healthline or Teledoctor must be subscribers to the network. Although it is probably too soon to judge the magnitude of returns for either Telenor in Pakistan or GrameenPhone in Bangladesh, GrameenPhone has reported being satisfied with the commercial results from its Healthline partnership. In Mexico, MedicallHome reports that its fixed-line operator partner, TelMex, is pleased with its share of the hotline’s sub- scription revenue (in return for which it only handles billing and collection). The greatest short-term returns to operators seem to have come from a non- financial standpoint: helping to bring reliable health advice to unserved areas can boost brand value. GrameenPhone in Bangladesh won the “Best Use of Mobile for Social & Economic Development” category of the GSM Association’s 3GSM Global Mobile Award in 2007. Telenor in Pakistan and GrameenPhone also adver- tise health hotlines as value-added services to set themselves apart from compet- ing MNOs and to build brand loyalty with subscribers. Both of these MNOs value the health hotline services for enhancing brand value and winning public recogni- tion that they are good “corporate citizens.” In the medium and long term, an improved corporate social responsibility image may also reduce customer turnover and lower the cost of acquiring new cus- tomers. But it is too early to attempt to quantify these financial benefits, even if this were a simple task. Managing Operational Challenges Health hotline providers must tackle three key operational challenges: • Medical liability and negative public relations. • Non-standard information or advice. • High turnover among call agents. 136 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket Limiting medical liability and negative public relations Because they provide callers with health and medical information that callers then use as the basis for self-treatment or doctor visits, health hotlines may find them- selves accused of providing the wrong information or suggesting the wrong course of action. None of the health hotline operators interviewed stressed this as a major risk, in part because they do not perceive the health systems in India, Mexico, Bangladesh, and Pakistan to have a high level of litigation for medical malpractice. And at least one study in the United States suggests that inappropriate telephone triage in primary care results mainly in temporary and minimal harm to patients.25 Still, the four hotline operators we interviewed recognize the need to standard- ize information and advice (as discussed in the next section) as one way to avoid such an outcome. MedicallHome is seeking multiple certifications as a call center, including certification from ISO (the International Standards Organization); it also maintains a dedicated complaints line to resolve complaints and disputes rap- idly. On the other hand, partners of these health hotlines, particularly the MNOs in Bangladesh and Pakistan, saw the potential for considerable public relations risk from complaints and potential litigation for incorrect advice or information. In Pakistan, eHealth Services, the Teledoctor hotline manager, specifically sought and received an endorsement from the Ministry of Health in Sindh province, at the request of Telenor. Telenor also maintains the following disclaimer on its Teledoctor webpage: Telenor neither gives secondary medical advice directly nor engages in the practice of medicine. In all cases Telenor is not accountable for the malpractices, genuineness or authenticity of the advice/information given through this service or for the credentials of the medical experts giving the information/advice and Telenor shall not be liable for any loss or damage caused to any subscriber or any other party as a result there- of.26 Interestingly, Healthline in Bangladesh faces the opposite problem. On occasion, one of the call center doctors will diagnose an ailment that requires a certain pre- scription medicine to treat. However, due to the absence of law on providing pre- scription and non-prescription drug formularies over phone, Healthline’s man- agement does not permit its doctors to give a prescription over the phone. Callers often plead with doctors to prescribe something for their illness or pain, but the doctors can only respond by asking the caller to visit a clinic or physician for an in- person consultation. Ensuring standardization of information Health hotline providers take several steps to standardize the information they provide to callers. First, some use software with built-in protocols that guide call agents through a series of questions. As the caller gives responses to the questions, innovations / winter 2009 137 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 Gautam Ivatury, Jesse Moore, and Alison Bloch the protocol narrows down the possible causes of the ailment and the recommend- ed treatments. Fonemed, a U.S.-based company, has deployed this software inter- nationally at a number of existing and soon-to-be-launched health hotlines (including MedicallHome in Mexico). In the Philippines, for example, Telemed Asia-Pacific plans to launch a new health hotline staffed by nurses who will use the Fonemed software to diagnose patients and recommend treatment. The software walks the nurse through standard protocols developed in the United States for adults and children.27 Taking this approach can ensure a standardized service at a lower cost than employing doctors to answer all calls. HMRI in India took a similar approach by building an automated diagnosis Decision Support System in-house to allow paramedics to diagnose minor ail- ments. Doctors at the hotline are only consulted on complex cases. The system includes 175 algorithms developed internally to diagnose ailments and 570 disease summaries—standard scripts that call agents read aloud to callers to explain their condition and recommended treatment. A key performance indicator for the hot- line is the percentage of callers who can be diagnosed through its 175 custom algo- rithms. In Bangladesh, Healthline decided that because it uses licensed doctors to answer calls, it does not need standard protocols to arrive at a diagnosis of the patient’s condition and to deliver standard treatment (as these protocols are focused on guiding nurses, according to Healthline). For the doctor, following the protocol would restrict flexibility in the line of questioning, and prevent the doc- tor from quickly reaching to complaints or ailments common in Bangladesh (but not included in standard protocols built into off-the-shelf software). Instead, Healthline relies on training its doctors and documenting a history of patient records to yield standardization and common responses from the team. Teledoctor in Pakistan also found that standard protocol-based software was costly and time-consuming for doctors. Instead, it relies on a quality control team that randomly monitors calls to ensure a proper standard of information and advice. The team reviews individual patient health records that the doctors main- tain through Teledoctor’s software to ensure that doctors have been maintaining a high quality of service. Retaining doctors and nurses Though these operators provide competitive compensation and supplement the income their staff members earn at hospitals and in private practice, all the oper- ators concede that managing the turnover in call agents is a challenge. HMRI in India expects its annual turnover to settle within the 15 percent to 30 percent range. The main reasons for agent turnover include a lack of in-person interaction with patients and the sense of boredom that comes from repeatedly providing sim- ilar, standardized information to callers over a period of four to eight hours each day. As in any business, turnover has several impacts: the operators need to hire and 138 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket train replacement staff, accumulated knowledge may be lost when a call-taker leaves, and morale and productivity can drop when turnover reaches a critical level. The health hotlines we studied described a range of strategies to cope with, or mitigate, this turnover. MedicallHome in Mexico tries to balance its own demands on doctors with their other interests and responsibilities. It pays its doctor call agents a wage comparable with what they would earn in a traditional position: about U.S. $1,000 per month for working half-time. It contends that because they
make it a part-time rather than full-time position, the doctor can still have face-to-
face patient interaction, increase his or her experience base by handling many
patients, and keep skills sharp—all while satisfying the desire to perform tradition-
al consultations.
At the other end of the spectrum, Healthline in Bangladesh believes that
turnover of doctors is healthy. TRCL operates the hotline with full-time doctors
and encourages them to leave after two to three years to pursue higher studies or
fellowships that will strengthen their clinical skills. After this amount of time, most
lose their focus and motivation to handle phone-based consultations. Healthline’s
management believes that working in a medical call center is a wonderful transi-
tion job for young doctors, to fine-tune their clinical expertise and knowledge in a
challenging and dynamic environment, and to become familiar with technology
that can help doctors increase clinical efficiency. To ensure a regular flow of doc-
tors to staff the hotline, the firm is based in the Dhanmodi residential area of
Dhaka, where medical colleges and physician practices are concentrated.
COMMERCIAL RESULTS OF HEALTH HOTLINES
Health hotlines are interesting from a commercial standpoint, since they offer
callers low-cost access to basic health information and consultations and provide
competitive differentiation for mobile operators and possibly reduce subscriber
churn; they may also make public health care provision more efficient. Insofar as
they are profitable, health hotlines may be poised to scale far beyond the size of
most mobile health services deployed to date.28
In this section ,we address two questions. First, is the health hotline business
viable, today and for the long term? Second, what are the commercial limits to this
business, in terms of its potential for scale and its ability to be replicated across
markets?
Viability of the Health Hotline Business
Since all four of the hotlines studied operate in competitive environments and take
a strong commercial approach to their businesses, we are not able to discuss key
financial results. However, the three for-profit companies report healthy profits or
at least say they cover costs. Based on the cost structure of the health hotline
model, the viability of these operations is a sign that the providers have been able
to offset the variable costs of call agents (doctors, nurses, and non-medical person-
nel) and the amortization of the callcenter setup, with revenue from callers. As a
innovations / winter 2009
139
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
further sign of their confidence in the model’s financial viability, Healthline and
MedicallHome have begun expanding internationally in partnership with local
players and commercial financiers. Teledoctor is planning similar expansion in
the coming year or two.
But it is not clear that health hotlines can be expected to continue on an
unabated path to large scale and further profits. Our analysis of these four relative-
ly young hotlines suggests several areas of vulnerability. These concerns are most
relevant to hotlines that are sponsored by an MNO or a government. In essence,
the risk is that the operating partner’s demand to scale up and expand its scope
may not be matched by that of its partners—whether they are MNOs, govern-
ments, or other actors. At the least, a mismatch could lead to friction and delay, and
insufficient financing for new opportunities.
Partners in the MNO-sponsored model may find themselves moving at differ-
ent speeds over time. The two health hotline providers, TRCL (Bangladesh) and
eHealth Services (Pakistan), have formed ambitious plans to add new mobile-
enabled services to their portfolio, including electronic prescriptions, automated
referrals, and video consultations via telemedicine. But MNOs, which have aggres-
sive targets to increase penetration in relatively open markets, may prioritize
investments to expand their core business rather than allocating resources to
develop new health hotline services.
A similar challenge may await the government-sponsored model. As HMRI’s
scope and scale increases, neither the state government nor the Satyam Foundation
(privately funded by the founder of Satyam Computer Services) may have the
financing to keep it free of cost to customers. In addition, there is always the risk
that a government-funded program will lose funding or support should the gov-
ernment change. This may be a minor risk given the professionalism and wide
reach of the HMRI service and the level of funding made by private donors and
industry. Still, this is a long-run risk to the viability of the government-sponsored
approach.
Commercial Limitations of the Model
Some observers, seeing the success of health hotlines in reaching relatively large
numbers of people, including those in hard-to-reach and rural areas, have won-
dered how big this model can grow, and how easy it is to replicate in developing
countries. In general, it seems that scaling up the health hotline to handle more
and more calls will be an easier task than expanding the scope of the service to
integrate with physical health care facilities.
Increasing scale: Expanding call volumes
For operators scaling up call volumes, technology does not seem to be a constraint.
The technology and human resources that make up a call center can theoretically
support far greater numbers of concurrent calls. While not specifically for a health
hotline, an international consortium in Karachi, Pakistan is building what will
house the world’s largest call center, with 10,000 seats (the largest, in Sydney, has
140
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
8,000 seats).29 By comparison, the largest health hotline today, HMRI, maintains
just over 400 seats to handle 50,000 calls per day. Extrapolating from the staffing
of the four health hotlines we studied, a 10,000-seat call center would be able to
handle more than one million calls per day.
Existing health hotlines maintain excess technical capacity, although some sys-
tems are likely to need upgrading or even “re-architecting” as volumes multiply.
TRCL in Bangladesh reports that its existing call answering and routing systems
can handle up to 240 concurrent lines, although only about 15 are used today at
peak hours. New entrants to each of these markets would also be able to handle
latent demand and increased call volumes.
Instead, the main constraint to scaling up call volumes is likely to be the limit-
ed availability of physicians and other medical personnel to staff the health hot-
line. Also, some health hotline operators report a lack of funding for expansion.
In Bangladesh, for example, the management of Healthline sees real challenges
in identifying, hiring, training, and retaining 500 doctors to answer hundreds of
thousands of calls daily. Although the company does foresee changing its staffing
complement to include paramedics and nurses, health hotlines in many countries
may not be able to take that approach. Whether the need is doctors or less-experi-
enced medical personnel, the health system and existing educational institutions in
the countries examined will probably not be able to keep providing the number of
staff required if call volumes rise quickly and dramatically.
A further constraint is the simple fact that the hotline operator may not have
an interest in scaling up call volumes beyond a certain point. In Mexico,
MedicallHome is interested in maintaining a subscriber base of about one million
households in the face of significant (15 percent) annual turnover within this base.
Similarly, TRCL in Bangladesh and eHealth Services in Pakistan plan to expand the
scope of their health hotline services, which may require paying less attention to
acquiring new callers and expanding call volume.
Solutions to these constraints may include an expansion in the number of
medical education providers, systems that route calls directly to doctors and other
medical personnel rather than requiring them to sit in call centers, and locating
health hotlines offshore, in markets with a greater availability of personnel.
Increasing scope: Integrating with the health care infrastructure
The constraints to expanding the functionality of health hotlines may be harder to
overcome than those to simply increasing call volumes. Several health hotline
providers now envision connecting their service to rural medical practitioners,
health clinics and labs, and even urban hospitals. But if many more people call the
hotlines and require referrals to clinics, lab testing, or medicines from pharmacies,
these physical service points may find themselves stretched beyond their capacity.
Also, the standards and collaboration required to connect all of these organiza-
tions—from both a regulatory and a technological standpoint—are not in place.
For example, today most developing country health systems lack any unique sys-
innovations / winter 2009
141
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
tem for identifying patients who reliably use multiple health providers, insurance
companies, and other health facilities.
Replicating health hotlines
The high demand for health care services and health information across develop-
ing countries, and the successful track record of the health hotlines studied, would
suggest a rationale for setting up similar services in new markets.
If a government wishes to set up a health hotline, special conditions need not
apply. If committed to the idea, policymakers should be able to adapt regulation
and enlist private firms and foundations to set up a health hotline service. But
based on the experience reviewed in this report, we see two sets of exogenous fac-
tors that will determine whether a for-profit health hotline can launch. These are,
first, the conditions of the market, and second, the openness of health policy and
regulation.
At the market level, there are three requirements. First, there should be a crit-
ical mass of individuals willing to pay for phone-based health information. Based
on the experience of Healthline and Teledoctor, it seems that even reaching a level
of 10,000 calls per day can generate sufficient revenue to cover costs.
Second, the health hotline must be able to partner with at least one MNO or
other firm with a large-scale retail business, in order to be able to collect payments
from callers or subscribers. Collecting payment by credit or debit card through the
Internet or over the phone may be possible in some places, but in many markets
this would restrict the potential user base to only middle-class or affluent cus-
tomers. In some least-developed countries, the only potential partners with suffi-
cient retail reach are MNOs. Ensuring their buy-in and resource commitment may
be essential to the feasibility of a new health hotline.
Finally, there should be an adequate supply of relatively low-cost, qualified
health personnel to staff the hotline. In countries without such a supply, it may be
feasible to “offshore” the hotline to a neighboring country or one with the same
language.
In most developing countries, no specific regulation is in place that either pro-
motes or prohibits these services. Instead, health hotline operators have had to
secure regulatory permission to run the service by situating it within existing
healthcare, call center, and telecommunications regulations. To do this, providers
setting up new health hotlines have made regulators comfortable with their com-
mitment to quality, their business approach, and their systems.
In general, they do not perceive this process as having been very difficult.
According to one hotline manager, the health system needs are so great that the
country’s regulators are permitting all sorts of providers—even those with mini-
mal or no formal training—to advertise themselves as health care professionals.
Therefore, even though health care regulators are not entirely sure how to treat the
health hotline, they are satisfied with a provider that is licensed by some regulato-
ry authority, can show that its staff has medical certifications and experience, and
142
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
can demonstrate that its processes and protocols are standardized and of good
quality.
The main requirement from a regulatory standpoint, therefore, is that health
regulators be open to considering a new approach led by private firms, and willing
to grant some regulatory space and flexibility to permit this innovative model to
emerge.
In Mexico, MedicallHome operates with a legal opinion that draws a distinc-
tion between its service and activities regulated by the General Health Act.
According to the opinion, the act makes no limitation regarding the service of
medical advice via telephone, as it is not considered a medical consultation as
established elsewhere in the Mexican regulation. (To be a medical consultation, a
physician must conduct a physical examination of the patient.) MedicallHome’s
hotline
is only treated as a value-added service under the Federal
Telecommunications Law, and is licensed to operate as a call center in Mexico.
In Bangladesh, the health hotline is treated differently. TRCL, the hotline oper-
ator, is registered as a health related information, technology, and service compa-
ny, received a license under the telecommunications regulator’s new call center
licensing regime, and is also considered a value added service provider to telecom-
munications firms and taxed at 5.5 percent on all call charges. Although there is no
formal regulation governing phone-based medical consultations, the government
has implicitly legalized this activity by announcing that all public health centers at
the sub-district level will be equipped with mobile phones to answer calls from
patients at no cost.30
These examples suggest that an enabling regulatory framework is one that per-
mits the setup of a new call center, allows health information and advice to be
delivered over the telephone, and does not overly tax mobile phone “value-added
services,” such as health information. Doing so would raise the price of calling a
health hotline above a level that poor customers can afford.
THE SOCIAL IMPACT OF HEALTH HOTLINES IN DEVELOPING
COUNTRIES
At least six factors determine the social impact of a health hotline:
• The degree to which the population served lacks other sources of affordable
and accurate health information;
• The nature of health inquiries that a population directs to the health hotline;
• The quality of the information provided;
• The affordability of the service;
• The ease with which even the least empowered and technology-savvy individu-
als can access it;
• The degree to which the hotline supports and shares information with local
healthcare providers;
Understanding social impact, therefore, requires an analysis of both the hotline
itself (the “supply side”) and the population it targets and serves (the “demand
innovations / winter 2009
143
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
Table 8. Estimated Calls Related to Serious Diseases or Conditions.
side”).
In this study we did not specifically analyze the cost, availability, and quality of
the health information already accessed by the people whom the health hotlines
target in developing countries. We do not know of any such rigorous impact
assessments being conducted. And since the health hotlines identified in develop-
ing countries have only been operating for two to three years, the results of such
evaluations might still be years away.
Instead, we can draw some early insights about the likely social impact of
health hotlines in developing countries based on two sources of information.
First, a handful of small “point-in-time” surveys and some anecdotal evidence sug-
gest that health hotlines are having a positive impact on people’s lives. We can also
examine the data these four hotlines collected through their call-tracking software.
In examining this impact, we will consider two types of benefits to society: direct
benefits to callers, and indirect benefits to the health system as a whole.
Early evidence of impact
Based on initial surveys and anecdotal evidence, we draw four early insights about
the social impact of the hotlines we studied:
144
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in Your Pocket
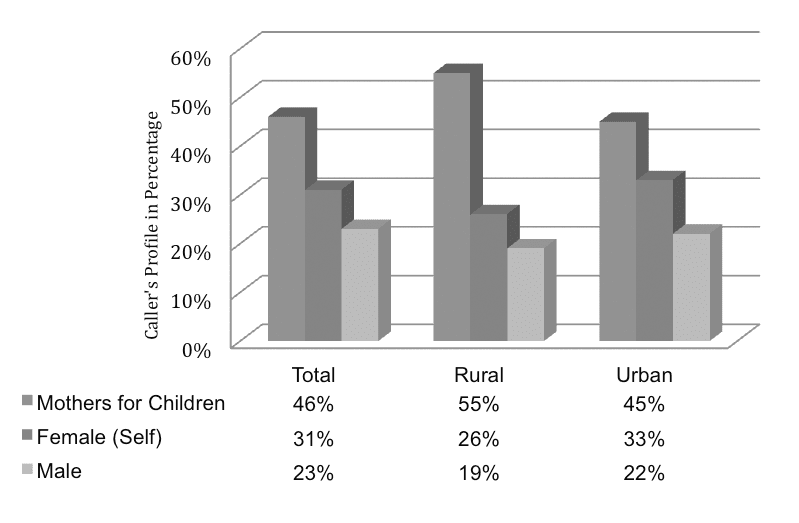
Figure 3. Callers to Healthline (Bangladesh).
Source: TRCL, Bangladesh.
• Health hotlines may reach people who have historically had poor access to
quality, affordable primary care.
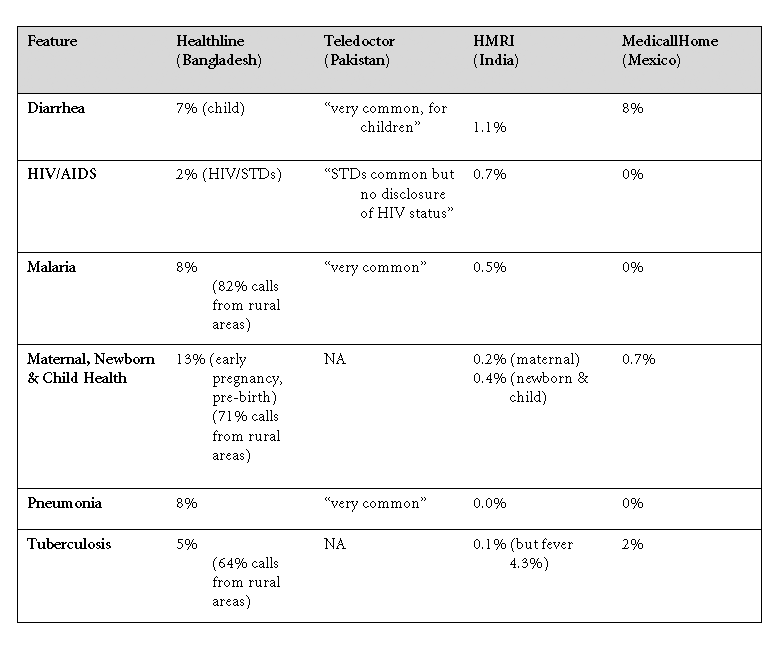
• In some cases, many people who call health hotlines are battling diseases or
conditions that affect large populations in the developing world.
• Using health hotlines instead of traveling to physical health care providers
appears to save people time and money.
• Callers are generally satisfied with the quality of information and advice they
receive from these hotlines.
Health hotlines may reach people that who historically had poor access to quality,
affordable primary care.
A survey31 of 253 callers to Healthline in Bangladesh, selected at random from
among GrameenPhone’s subscribers and asked questions adopted from the
Patients Satisfaction Questionnaire (PSQ-18),32 found that most callers had
income below the poverty line (56 percent), and that most were located in rural
areas (63 percent). Of those in rural areas, 72 percent reported not having access
to a modern health care provider within a five mile radius of their home.33 Figure
2 shows a further breakdown of callers to the Healthline service by gender, role,
and geographic location, based on TRCL’s internal survey of 2,160 callers over a
period of one month during the last quarter of 2008.
Not every health hotline studied reported serving a similar demographic pro-
innovations / winter 2009
145
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
Gautam Ivatury, Jesse Moore, and Alison Bloch
file. HMRI in Andhra Pradesh, India, reports that 90 percent of its callers are men,
and nearly 40 percent are between the ages of 15 and 24. Still, 20 percent come
from India’s most disadvantaged communities (scheduled castes and tribes), and
an estimated 70 percent from rural areas.
In Mexico, on the other hand, although gender information was not available,
the typical caller is from an urban location and is middle class. The pricing of the
service—a subscription of MXP 50 (U.S. $3.64) per caller per month—is likely to rule out those who are poor. (According to Mexico’s Secretary of Social Development, urban dwellers earning up to MXP 42 per day are classified as living in poverty.)34 For a poor person, it would not make sense to pay more than a day’s earnings to subscribe to a service he or she might not call. The customer base is further restricted by the necessity of owning a fixed-line phone connection; Telmex, the country’s fixed-line operator, handles the billing for MedicallHome by including it as a service on monthly phone bills. And there are only ten million fixed-line connections in the country. Finally, MedicallHome has tracked 80 per- cent of its calls as originating in 21 cities. Significant percentages of callers suffer from serious diseases and conditions. Table 8 shows the percentage of callers from each of the hotlines who are suffering from a serious disease or condition, or were diagnosed with that ailment by the hotline. Receiving phone-based advice on treating these conditions may be valu- able. A recent study in Pakistan found that home-based treatment of children with pneumonia was as effective as hospitalization, the course of action recommended by the WHO protocol.35 According to Healthline’s founder, in 2009 the company aims to serve more than six million diabetes patients in the country, two million children up to age five who often suffer from diarrheal diseases, and about one million patients suf- fering from tuberculosis (TB). Teledoctor recently took special initiatives to serve people suffering from res- piratory tract infection (RTI), pneumonia, influenza, and dengue, particularly when many people were sleeping outdoors after the earthquake that occurred in Baluchistan on October 29, 2008. Telenor, the hotline’s MNO partner, made all calls to the Teledoctor service free for one month, and the hotline’s call volume doubled. In addition to hiring extra doctors to staff the hotline, the company recorded preventative information about malaria and dengue fever for callers to listen to while they were on hold waiting to speak to a doctor. In India, HMRI has prioritized its battles against diabetes, hypertension, and asthma in rural areas, as large numbers of people remain undiagnosed. Using health hotlines instead of traveling to physical health care providers can save people time and money. On this question, the survey of Healthline users in Bangladesh again yields useful data.36 By using the service, most callers reported saving travel time (98 percent) 146 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket and money (91 percent), and experiencing shorter wait times (97 percent) and reduced doctor’s fees (83 percent). HMRI in India makes a similar case for the cost savings it creates, by analyzing the high cost of health care for rural villagers. According to its research, the rural “out-of-pocket” expenditure on health care, relative to household income, is five times higher than for urban dwellers. And since 70 percent of healthcare spending is out-of-pocket, rural citizens carry virtually their entire health care burden on their own shoulders. Transportation costs are a big part of this disparity: in one community, HMRI found that 19 of 22 rural villages lay more than 3 kilometers away from a primary health care center. Meanwhile, 95 percent of the primary users of a health clinic lived within a distance of three kilometers. Therefore, rural villagers apparently go without health care, or spend exorbitant amounts to access it. In addition to saving rural and urban callers money by reducing their need to visit clinics or physicians, several health hotlines take advantage of their relatively large numbers of users to give callers discounts at these facilities, hospitals, labora- tories and pharmacies. MedicallHome in Mexico gives subscribers discounts of up to 50 percent at nearly six thousand clinics, hospitals and pharmacies. Healthline in Bangladesh text-messages discount “coupons” to frequent callers that they can present at hospitals for discounts of 10 percent off hospital bills. Callers are generally satisfied with the quality of information and advice they receive from these hotlines. HMRI in India reports a customer satisfaction score of 4.3 out of 5.0 from its reg- ular customer satisfaction surveys. Similarly in Bangladesh, Healthline received a score of 4.36 out of 5.0 in a customer satisfaction survey conducted by AC Nielson during the first quarter of 2008, Fifty-nine percent of callers surveyed rated the service “excellent” and 22 percent labeled it “fair.” And 68 percent said the informa- tion they received was “very helpful.” Indirect Benefits of Health Hotlines In addition to direct benefits, health hotlines may perform some functions typical- ly covered by other parts of the public health system at lower cost, thereby indirect- ly improving the efficiency and quality of these facilities. For example, HMRI in India estimates that of the 600,000 outpatient visits that go unmet in Andhra Pradesh, about 60 percent may be conducted without an in- person consultation, and 55 percent of ailments may be treated at home without a doctor. Through phone-based triage and consultation, health hotlines can take on a function that would ordinarily be performed by primary health facilities. Rural health clinics and medical practitioners benefit indirectly when fewer patients show up, and those who do can be offered more attention. Limitations of Social Impact Still, several factors may limit the social impact of health hotlines. innovations / winter 2009 147 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 Gautam Ivatury, Jesse Moore, and Alison Bloch Affordability Evidence from India and Bangladesh suggests that pricing may be too high for the very poorest. Healthline in Bangladesh charges callers only 15 taka (U.S. $0.22) for
the first three minutes and 5 taka (U.S. $0.07) per minute thereafter, including the cost of the prepaid talk time. Still, Healthline’s management and some of the callers it randomly surveyed acknowledge that this cost is too high for many poten- tial users. Availability Poor mobile coverage and call quality is also a barrier to use in both India and Bangladesh. The managers of HMRI in India say that despite claims of near-uni- versal mobile network coverage in the state, only about 50 percent of the state’s geography is reached. Several phone numbers from which the largest numbers of calls originate are public telephones in areas where mobile coverage is poor. Furthermore, as many as 50 percent of the average daily 50,000 calls to HMRI are cut short because the signal is poor or interrupted. Accessibility Managers of HMRI in Andhra Pradesh are also concerned about the accessibility of their hotline to women, given that women make up such a relatively small per- centage (10%) of the callers. Meanwhile, 60 percent of callers are males under age 25 who inquire about sexuality, acne, and other issues of concern to their demo- graphic group. Two possible explanations are that because the service is free, more young men are likely to use it casually or make prank calls, and that far fewer women than men use mobile phones in Andhra Pradesh. More research is needed to better under- stand caller demographics. But call pricing may explain more than gender differ- ences: Healthline in Bangladesh charges callers but reports high usage by women. In the short term, HMRI is making it a priority to rebalance its caller demo- graphics through health care camps that operate temporarily in a given location, mobile vans, and dedicated marketing, among other strategies. Integration Finally, because the patient database and electronic health records that health hot- lines maintain on callers are not accessible by local clinics, laboratories, or hospi- tals (and vice versa), it is not possible for hotlines to communicate with these health care facilities to improve patient care. Patient information captured at any one location would ideally be shared with other facilities and the hotline to ensure a complete picture, avoid gathering information multiple times, and improve accuracy. Local practitioners would know if callers to a health hotline needed fol- low up or in-person visits. CONCLUSION: OPPORTUNITIES FOR SUPPORT In Section 5, we presented initial evidence of the benefits that health hotlines can 148 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket have for poor people in developing countries. On the basis of those arguments, we suggest that opportunities exist for donor agencies, governments, and industry bodies, including the GSMA Development Fund, to support the emergence and growth of health hotlines. We conclude with some thoughts for these actors: first policymakers and regulators, and then donors. Considerations for Policymakers and Regulators The first step for policymakers is to develop a view on the role (if any) that health hotlines should play in the health system. The state government of Andhra Pradesh in India took the position that a free, high-quality hotline would go far towards increasing the penetration of health information and basic care into areas that were mostly unserved. Similarly, after seeing the success of Healthline in Bangladesh, the country’s Health Ministry announced that it would equip all pub- lic hospitals in the country’s 481 sub-districts with mobile phones to answer calls from patients at no cost.37 On the other hand, Mexico’s health ministry seems to have chosen to allow private health hotlines to emerge. One explanation offered by observers is that it sought to avoid the political opposition that would arise if jobs in government hospitals and clinics were replaced by seats at a private call center. After establishing a vision of the role that the hotline can play in the health care system, a reasonable next step for policymakers would be to calibrate the level of intervention in the market required to achieve that desired state. In other words, should policymakers allocate funding to develop a free public health hotline? Should they instead encourage private health hotlines to develop, and rely on them to serve poor people who do not have good access to health care? Or, do some pri- vate hotlines already in operation need incentives to target poor and rural commu- nities in addition to the higher-income market segments that they already serve? And, as always, what are the political priorities and competing resource demands, and how much attention is available to dedicate to this topic? This second step requires policymakers to ground their vision in market and political realities. Should policymakers decide that health hotlines are an integral part of their public health systems, they may wish to ensure that barriers to their setup and growth are tackled. For instance, health policymakers could require that public and/or private doctors or paramedics spend part of each work week helping staff health hotlines. This could reduce the need for private operators to compete for these doctors and could ensure that the model can be scaled up. Governments could also subsidize calls to health hotlines from people who live in areas that are underserved by the public health system. This could be done simply, with private health operators being reimbursed for calls customers make from fixed-line num- bers in particular geographic areas or in the vicinity of specific mobile base sta- tions. At the very least, governments may decide that setting regulatory parameters can help ensure that any private health hotline activity results in positive outcomes for poor people. People with limited financial resources often lack the education and experience with formal services that they need to make good decisions about innovations / winter 2009 149 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 Gautam Ivatury, Jesse Moore, and Alison Bloch their health care (or their money, or anything else). As described above, operators of private health hotlines will certainly take strong steps to mitigate risks and avoid litigation, but they also have incentives to act in ways that do not necessarily serve the public interest. For instance, a private hotline may decide to refer customers to clinics or hospitals that pay better referral fees. Or, it might not make clear and simple disclosures to callers about the limitations of its advice and the need to visit a physician in person. One approach, therefore, might be to establish minimum standards of quality, availability, and public disclosure. In the area of emergency response (calls to 911 lines), some governments mandate that calls be answered in a certain amount of time and that certain information be collected. In this area, it might be worth con- sidering similar rules. They could govern, for example, the amount of capacity the call center should have, the minimum medical qualifications of call responders, and the minimum frequency and type of training given to call responders. Disclosure guidelines could also be standardized so that customers understand what they are and are not receiving. Another useful step, although it would likely require coordination with telecommunications regulators, would be to require mobile operators and fixed-line telephone companies to agree to a given 3- or 4- digit code (such as 9-1-1 or 3-8-3-8). This approach could avoid the scenario in which several MNOs or fixed-line telephone companies offer health hotline serv- ices through different codes, causing confusion among consumers. Considerations for Donors Bearing in mind both the large potential for health hotlines, and the challenges related to their growth and expansion, donors and development agencies may wonder what they should do to help the market mature. We have five recommen- dations. 1. Awareness. Health hotlines are new and still relatively unknown within the broader community of mobile operators and health practitioners. By supporting conferences, research studies, Web portals, social marketing campaigns, and other ways of evaluating and publicizing these services, donors can help build awareness and excitement among those who could deploy new hotlines. 2. Research. This paper has identified the emergence of health hotlines as being potentially valuable for expanding access to health care in developing countries. Further research must now be done to inform industry, policymakers, and donors. This should include careful analysis of the public health benefits, the effect on health outcome disparities, and the commercial benefits of health hotlines. The results should be shared widely via awareness activities like those mentioned above. 3. Regulation. Health care regulation is likely to become a key factor in the suc- cessful growth of health hotlines, as regulators become aware of these services and call volumes rise. Depending on how it is structured, regulation could either facil- itate new deployments or inhibit them. It will be important to help regulators understand health hotlines and educate policymakers on the research mentioned 150 innovations / winter 2009 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 A Doctor in Your Pocket above in order to make informed decisions. Ultimately, regulations will need to strike a careful balance: they must be open enough to encourage innovation in the marketplace, but restrictive enough to ensure client/patient privacy, protection, and a high standard of care. 4. Technical Assistance. As the market evolves and various stakeholders— including mobile operators, governments, and start-ups—begin to offer services, they will benefit from outside technical assistance and expertise. Donors should consider creating or supporting organizations that can develop that expertise and help support the nascent industry, for example by leading the creation of technical and performance standards around electronic medical records, electronic pre- scriptions, and other medical applications, and by promoting interoperability and connectivity. 5. Social Investment. Though it is not yet clear what type of social investment might be required to help accelerate deployments, donors can likely play a key financing role through a combination of seed grants, low-interest loans, venture capital, and subsidies. In supporting the four types of activities listed above, donors should aim to gain a solid understanding of what type of social investment would be required. Endnotes 1. Authors’ estimate using data from health hotline operators in these and other developed coun- tries. 2. Authors’ estimate using data from health hotline operators in Bangladesh, Mexico, Pakistan and India. 3. 3G Americas, Mobile connections reach 4 billion worldwide. Press release, December 22, 2008. Available at http://www.3gamericas.org. 4. TRCL internal survey of 2,160 callers over a one-month period during the fourth quarter of 2008. 5. This is sometimes referred to as “doctor-to-patient” or ‘D2P’ rather than “doctor-to-doctor” or ‘D2D’. 6. Global Call Center Network, The Global Call Center Report: International Perspectives on Management and Employment, 2007. Available at www.globalcallcenter.org. 7. A hotline may very well transition from one type of sponsorship to another: once its exclusive arrangement with an MNO expires, an MNO-sponsored hotline such as Teledoctor in Pakistan may partner with additional mobile operators and become an independent hotline. Including indirect costs, such as in-kind contributions of Satyam Computer Services staff to program the hotline’s software, this ratio is closer to 60 percent paid by the government, and 40 percent paid by Satyam Foundation and affiliates. 8. McKesson Asia Pacific, Telephone triage, advice, and referral services. Electronic brochure avail- able on McKesson webpage, www.mckesson.com.au, December 2006. Population of Western Australia found at www.wikipedia.org/wiki/Western_Australia. 9. V. Turner et al., Telephone triage in Western Australia. Medical Journal of Australia 176 (3): 100- 103 (2002). 10. From NHS Direct webpage: http://www.nhsdirect.nhs.uk/article.aspx?name=FactsAndFiguresAboutNHSDirect, accessed December 18, 2008. 11. E. Rolland et al., Using Ontario’s “Telehealth” health telephone helpline as an early-warning sys- tem: A study protocol. BMC Health Services Research 6:10 (2006). 12. NHS Direct webpage. 13. Rolland et al. innovations / winter 2009 151 Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023 Gautam Ivatury, Jesse Moore, and Alison Bloch 14. McKesson, Telephone triage. 15. NHS Direct webpage. 16. Ian St. George et al., “Telephone triage reduces out of hours work for country doctors.” 17. David Dunt, Robert Wilson et al., “Impact of telephone triage on emergency after hours GP Medicare usage: A time-series analysis.” Australia and New Zealand Health Policy 4:21 (2007). 18. NHS Direct calls cost GBP 16 each. E-Health Insider Primary Care, March 4 2008. 19. Ruth Wetta-Hall et al., “Help on the Line: Telephone-Triage Use, Outcomes, and Satisfaction Within an Uninsured Population.” Evaluation & the Health Professions 28 (4), 414-427 (2005). 20. J. Labarère, “Patient compliance with medical advice given by telephone.” The American Journal of Emergency Medicine 21, (4), 288-292 (2003). 21. S. Bagchi, “Telemedicine in rural India.” PLoS Med 3(3): e82 (2006). 22. E. Ganguly, PR Deskhmukh, and BS Garg, “Quality Assessment of Private Practitioners in Rural Wardha, Maharashtra.” Indian Journal of Community Medicine 33(1) (2008). 23. BK Patro et al., “Community Perception and Client Satisfaction about the Primary Health Care Services in an Urban Resettlement Colony of New Delhi.” Indian Journal of Community Medicine 33(4) October 2008. 24. They also offer performance-based bonuses of US$ 200 per month.
25. David Hildebrandt, John Westfall, et al., “Harm resulting from inappropriate telephone triage in
primary care.” Journal of the American Board of Family Medicine 19(5) (September-October
2006)
26. Available at http://www.telenor.com.pk/services/teleDoctor.php. Accessed December 18, 2008.
27. “Schmitt and Thompson telephone triage protocols for adults and children.” More information
at http://www.stcc-triage.com.
28. “Vital Wave Consulting, mHealth in the developing world—A landscape analysis.” Available at
www.vitalwaveconsulting.com.
29. Karachi’s IT Tower to be biggest in world: Nazim. Daily Times, Karachi, June 9 2008. Accessed at
http://www.dailytimes.com.pk/default.asp?page=2008\06\09\story_9-6-2008_pg7_17.
30. Bangladesh to introduce countrywide “telehealth care services.” Xinhua news service, January 8
2009. Accessed at http://www.cctv.com/english/special/techmax/20090108/101361.shtml
31. Rahman, 2008.
32. Ware, J. E., Snyder, M. K., and Wright, W. R. Development and Validation of Scales to Measure
Patient Satisfaction with Health Care Services: Volume I of a Final Report. “Part A: Review of
Literature, Overview of Methods, and Results Regarding Construction of Scales,” (Publication
No. PB 288-329) Springfield, VA: National Technical Information Service (NTIS), 1976 (262
pp).
33. A “modern” healthcare provider refers to a practitioner trained in allopathic care as opposed to
“traditional” healers or homeopathic practitioners.
34. Secretaria de Desarollo Social, “Medicion de la pobreza, varientes metodologicas y estimacion
preliminar” (2002). Serie: Documentos de Investigation 1. ISBN: 968-838-476-3. Comite Tecnico
para la Medicion de la Pobreza.
35. T Hazir et al. (2008) “Ambulatory short-course high-dose oral amoxicillin for treatment of
severe pneumonia in children: A randomised equivalency trial.” Lancet (371) 9606: 49-56.
36. Rahman, 2008.
37. Bangladesh to introduce countrywide “telehealth care services.” Xinhua news service, January 8
2009. Accessed at http://www.cctv.com/english/special/techmax/20090108/101361.shtml.
References
Bagchi, S. (2006). “Telemedicine in rural India.” PLoS Med 3(3): e82.
Bali, S. and Amar Jeet Singh (2007). “Mobile phone consultation for community health care in rural
north India.” Journal of Telemedicine and Telecare (13): 421-424.
Dunt, David, Robert Wilson, et al. (2007). “Impact of telephone triage on emergency after hours GP
Medicare usage: A time-series analysis.” Australia and New Zealand Health Policy 4:21.
152
innovations / winter 2009
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023
A Doctor in your Pocket
Ganguly E., PR Deskhmukh, and BS Garg (2008). “Quality Assessment of Private Practitioners in
Rural Wardha, Maharashtra.” Indian Journal of Community Medicine 33(1).
Global Call Center Network (2007). The Global Call Center Report: International Perspectives on
Management and Employment. Available at www.globalcallcenter.org.
Hazir, T., et al. (2008) “Ambulatory short-course high-dose oral amoxicillin for treatment of severe
pneumonia in children: A randomised equivalency trial.” Lancet (371) 9606: 49-56.
Hildebrandt, David, John Westfall, et al. (2006). “Harm resulting from inappropriate telephone
triage in primary care.” Journal of the American Board of Family Medicine 19(5), 437-442.
“Karachi’s IT Tower to be biggest in world: Nazim.” Daily Times, Karachi, June 9, 2008.
Labarère, J., et al. (2003). “Patient compliance with medical advice given by telephone.” Am J Emerg
Med 21: 288-92.
McKesson Asia Pacific, “Telephone triage, advice, and referral services.” Electronic brochure,
December 2006. Available at McKesson webpage, www.mckesson.com.au.
Munro, J., et al. (2005). “The impact of NHS Direct on the demand for out-of-hours primary and
emergency care.” British Journal of General Practice 55: 790-792.
NHS Direct Annual Report 2007/08. Available at http://www.nhsdirect.org.uk.
“NHS Direct calls cost GBP 16 each.” E-Health Insider Primary Care, Issue No. 158, March 4, 2008.
Accessed at http://ehiprimarycare.com.
Patro, BK et al. (October 2008). “Community Perception and Client Satisfaction about the Primary
Health Care Services in an Urban Resettlement Colony of New Delhi.” Indian Journal of
Community Medicine 33(4), 250-255.
Rahman, Mohammad A. (2008). “Introduction of Cellular Phone-Based Call-Center in Bangladesh:
Impact on Access to Health Care Information.” Dissertation, California State University, Fresno,
CA. This is a PowerPoint presentation received from author.
Review of NHS Direct to reduce number of patients it refers to GPs and hospitals. The Telegraph
(UK), November 22, 2008. Accessed at
Rolland, E., et al. (2006). “Using Ontario’s ‘Telehealth’ health telephone helpline as an early-warning
system: A study protocol.” BMC Health Services Research 6:10.
St. George, I., et al. (2003). Telephone triage reduces out of hours work for country doctors. New
Zealand Family Physician 30(2), 95-99.
Turner, V., et al. (2002). “Telephone triage in Western Australia.” Medical Journal of Australia 176 (3):
100-103.
“Victoria’s NURSE-ON-CALL Adds to Existing Health Call Centre Network.” June 4 2006. Available
at http://www.Callcentres.net, accessed on December 18, 2008.
Vital Wave Consulting (2008). “mHealth in the developing world: A landscape analysis.” Available at
www.vitalwaveconsulting.com.
Wetta-Hall, Ruth, et al. (2005). “Help on the Line: Telephone-Triage Use, Outcomes, and Satisfaction
within an Uninsured Population.” Evaluation & the Health Professions, 28 (4), 414-427.
3G Americas (December, 2008). Mobile connections reach 4 billion worldwide. Press release, avail-
able at http://www.3gamericas.org.
innovations / winter 2009
153
Downloaded from http://direct.mit.edu/itgg/article-pdf/4/1/119/704291/itgg.2009.4.1.119.pdf by guest on 07 September 2023