FOCUS FEATURE:
New Trends in Connectomics
Using network analysis to localize the
epileptogenic zone from invasive EEG recordings
in intractable focal epilepsy
Adam Li
, Bhaskar Chennuri
1
9
William Stacey
7
, Robert Norton
1
, Sandya Subramanian
8
, Austin Jordan
1
1
1
, Robert Yaffe
, Jennifer J. Haagensen
Shubhi Agrawal
3
3
, William S. Anderson
Nathan Crone
1
Sridevi V. Sarma
5
, Jennifer Hopp
, Zach Fitzgerald
5
, Kareem A. Zaghloul
, Chalita Atallah
4
4
, Juan Bulacio
4
, and Jorge Gonzalez-Martinez
6
9
, Steve Gliske
,
, Sara K. Inati
,
5
, Emily Johnson
7
4
, John T. Gale
,
a n o p e n a c c e s s
j o u r n a l
1Institute for Computational Medicine, Biomedical Engineering, Johns Hopkins University, Baltimore, MD, USA
2Neurology, Johns Hopkins Hospital, Baltimore, MD, USA
3Neurosurgery, Johns Hopkins Hospital, Baltimore, MD, USA
4Neurosurgery, Cleveland Clinic, Cleveland, OH, USA
5Neurology, University of Maryland Medical Center, Baltimore, MD, USA
6Surgical Neurology Branch, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, MD, USA
7Office of the Clinical Director, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, MD, USA
8Uptake Technologies Inc., Chicago, IL, USA
9University of Michigan, Ann Arbor, USA
2
,
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
Keywords: Focal epilepsy, Network analysis, Eigenvector centrality, Intracranial EEG, Seizure onset
localization, Spectral models
ABSTRACT
Treatment of medically intractable focal epilepsy (MIFE) by surgical resection of the
epileptogenic zone (EZ) is often effective provided the EZ can be reliably identified. Even
with the use of invasive recordings, the clinical differentiation between the EZ and normal
brain areas can be quite challenging, mainly in patients without MRI detectable lesions.
Consequently, despite relatively large brain regions being removed, surgical success rates
barely reach 60–65%. Such variable and unfavorable outcomes associated with high
morbidity rates are often caused by imprecise and/or inaccurate EZ localization. We
developed a localization algorithm that uses network-based data analytics to process
invasive EEG recordings. This network algorithm analyzes the centrality signatures of every
contact electrode within the recording network and characterizes contacts into susceptible
EZ based on the centrality trends over time. The algorithm was tested in a retrospective study
that included 42 patients from four epilepsy centers. Our algorithm had higher agreement
with EZ regions identified by clinicians for patients with successful surgical outcomes and
less agreement for patients with failed outcomes. These findings suggest that network
analytics and a network systems perspective of epilepsy may be useful in assisting
clinicians in more accurately localizing the EZ.
AUTHOR SUMMARY
Epilepsy is a disease that results in abnormal firing patterns in parts of the brain that comprise
the epileptogenic network, known as the epileptogenic zone (EZ). Current methods to
localize the EZ for surgical treatment often require observations of hundreds of thousands
of EEG data points measured from many electrodes implanted in a patient’s brain. In this
paper, we used network science to show that EZ regions may exhibit specific network
signatures before, during, and after seizure events. Our algorithm computes the likelihood
Citation: Li, A., Chennuri, B.,
Subramanian, S., Yaffe, R., Gliske, S.,
Stacey, W., … Gonzalez-Martinez, J.
(2018). Using network analysis to
localize the epileptogenic zone from
invasive EEG recordings in intractable
focal epilepsy. Network Neuroscience,
2(2), 218–240. https://doi.org/10.1162/
netn_a_00043
DOI:
https://doi.org/10.1162/netn_a_00043
Supporting Information:
https://doi.org/10.1162/netn_a_00043
https://github.com/ncsl/eztrack
Received: 1 July 2017
Accepted: 9 January 2018
Competing Interests: The authors have
declared that no competing interests
exist.
Corresponding Author:
Sridevi V. Sarma
ssarma2@jhu.edu
Handling Editor:
Olaf Sporns
Copyright: © 2018
Massachusetts Institute of Technology
Published under a Creative Commons
Attribution 4.0 International
(CC BY 4.0) license
The MIT Press
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
of each electrode being in the EZ and tends to agree more with clinicians during successful
resections and less during failed surgeries. These results suggest that a networked analysis
approach to EZ localization may be valuable in a clinical setting.
INTRODUCTION
Epilepsy is one of the most common brain disorders, characterized by chronically recurrent
seizures resulting from excessive electrical discharges from groups of neurons (Brodie et al.,
1997). Epilepsy affects over 50 million people worldwide, and over 30% of all individuals with
epilepsy have intractable seizures, which cannot completely be controlled by medical therapy
(Berg, 2009; Berg & Kelly, 2006; Kwan & Brodie, 2000). That is, seizures continue to occur de-
spite treatment with a maximally tolerated dose of at least two antiepilepsy drugs (AEDs). The
direct cost of assessing and treating patients with medically intractable focal epilepsy (MIFE)
ranges from $3 to $4 billion annually ($16 billion in direct and indirect costs) in the United
States (Murray, Halpern, & Leppik, 1996). Eighty percent of these costs are incurred by pa-
tients whose seizures are not adequately controlled by AEDs (Begley et al., 2000). The burden
of MIFE, however, is much greater than heavy financial costs. MIFE is a debilitating illness
where individuals lose their independence, causing profound behavioral, psychological, so-
cial, financial, and legal issues (Ferro & Speechley, 2009; F. Gilliam et al., 1999; F. G. Gilliam,
2005; Hermann et al., 2006; Schuele & Lüders, 2008). Cognitive performance may be im-
paired by MIFE as well as by side effects of AED therapy (Ferro & Speechley, 2009; F. Gilliam
et al., 1999; F. G. Gilliam, 2005; Hermann et al., 2006; Schuele & Lüders, 2008).
Despite the heavy sequelae from MIFE, there is a potentially curative procedure, surgical re-
section of the epileptogenic zone (EZ), which can be defined as the minimal area of brain tissue
responsible for generating the recurrent seizure activity (Lüders, Najm, Nair, Widdess-Walsh,
& Bingman, 2006). However, to be effective, this procedure depends on correct anatomical
identification of the EZ, which is often poorly defined. A comprehensive presurgical evaluation
is necessary to better delineate the EZ as well as to identify the risk of neurologic morbidity such
as motor, visual, or speech impairment. Various noninvasive methods are currently applied in
the attempt of defining the EZ, the eloquent cortical and subcortical areas and, consequently,
the optimal resective surgical strategy. Noninvasive techniques include scalp EEG and video-
EEG monitoring, neuropsychological tests, speech-language studies, and brain imaging (MRI,
PET, ictal SPECT). Of these methods, the highest predictor of surgical success is identification
of a single visible MRI lesion (Bulacio et al., 2012; Jeha et al., 2007, 2006; McIntosh et al.,
2004; See et al., 2013; Urbach et al., 2004).
Localization and surgical success in seizure control are even more challenging in patients
with nonlesional MRI. When the noninvasive methods of localization fail to identify the EZ,
an invasive monitoring evaluation may be indicated, involving the implantation of subdural
grid electrodes (SDE) through open craniotomies or stereoelectroencephalography (SEEG; Nair,
Burgess, McIntyre, & Lüders, 2008; Önal et al., 2003; Widdess-Walsh et al., 2007). The process
of identifying the EZ then involves visually inspecting tens to hundreds of invasive EEG signals
without much assistance from computational tools. Epileptologists currently study the onset of
seizure events that occur over several days. Early presence of beta-band activity (beta buzz) or
bursts of high-frequency oscillations (HFOs) in the 100–300 Hz range, which typically occur
milliseconds before the clinical onset of seizures are localizing of the seizure onset (Fisher,
2012). Channels where seizure onset features first appear are commonly defined as the seizure
onset zone (SOZ), the current best estimate of the unknown EZ. This is based on the assumption
219
Focal epilepsy:
A subset of epilepsy in which
seizures originate from a focal area
of the brain.
Epileptogenic zone:
The minimal amount of brain region
that must be removed to stop
seizures from occurring.
High-frequency oscillations:
Electrophysiological phenomena that
involve oscillatory activity at very
high frequencies (such as greater
than 200 Hz).
Network Neuroscience
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
that the epileptic cortex generates epileptiform activity, which then entrains other regions into
a clinical seizure (Fisher, 2012). Electrodecremental responses (loss of rhythmic activity) are
also often observed.
In general, epileptologists look at a variety of signatures to make their
decision (Fisher, 2012). Despite all of these possible EEG signatures, determination of the EZ
may remain unclear for nonlesional patients (Gonzalez-Martinez et al., 2013; Jung, Pacia, &
Devinsky, 1999; Niedermeyer & Silva, 2004; Wieser, 1998). See Figure 1 for a schematic of a
current clinical process of localizing the EZ.
Network analysis of intracranial EEG data has been heavily used to study brain activity
(Bassett & Bullmore, 2006; Braun, Muldoon, & Bassett, 2015; Bullmore & Bassett, 2011;
Deuker et al., 2009). Networked-based analysis assumes that signals from different EEG chan-
nels are samples of activity from brain regions that are structurally and/or functionally con-
nected and therefore dependent (Kerr et al., 2011; Santaniello et al., 2011; Yaffe et al., 2012).
Several important prior studies have looked at network dynamics in epileptic cortex during
seizure events. Some works investigate correlation structure over seizure events and note
changes in network coherence over events without relating metrics back to clinically anno-
tated EZ (Kramer et al., 2010; Schindler, Leung, Elger, & Lehnertz, 2007). Other studies apply
network methods, computing interelectrode coherence, and relate these measures back to
clinically annotated EZ or resection regions, but on data collected from a relatively small set
of patients (Khambhati, Davis, Lucas, Litt, & Bassett, 2016; Korzeniewska et al., 2014; Schevon
et al., 2007; Sinha et al., 2017). Studies that incorporate computational modeling to explain
mechanisms of seizures and the EZ include Khambhati et al. (2016) and Sinha et al. (2017) .
Here, we show a novel network-based algorithm that takes advantage of a certain type of
signal evolution (ranked eigenvector centrality) and utilizes preictal, ictal, and postictal data
for tissue suspected to be within the EZ. Our study combines data from four centers and an-
alyzes a total of 113 seizures from 42 patients. We compute network-based statistics and
Eigenvector centrality:
is a graph theoretic measure of how
influential a node is within a
network.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
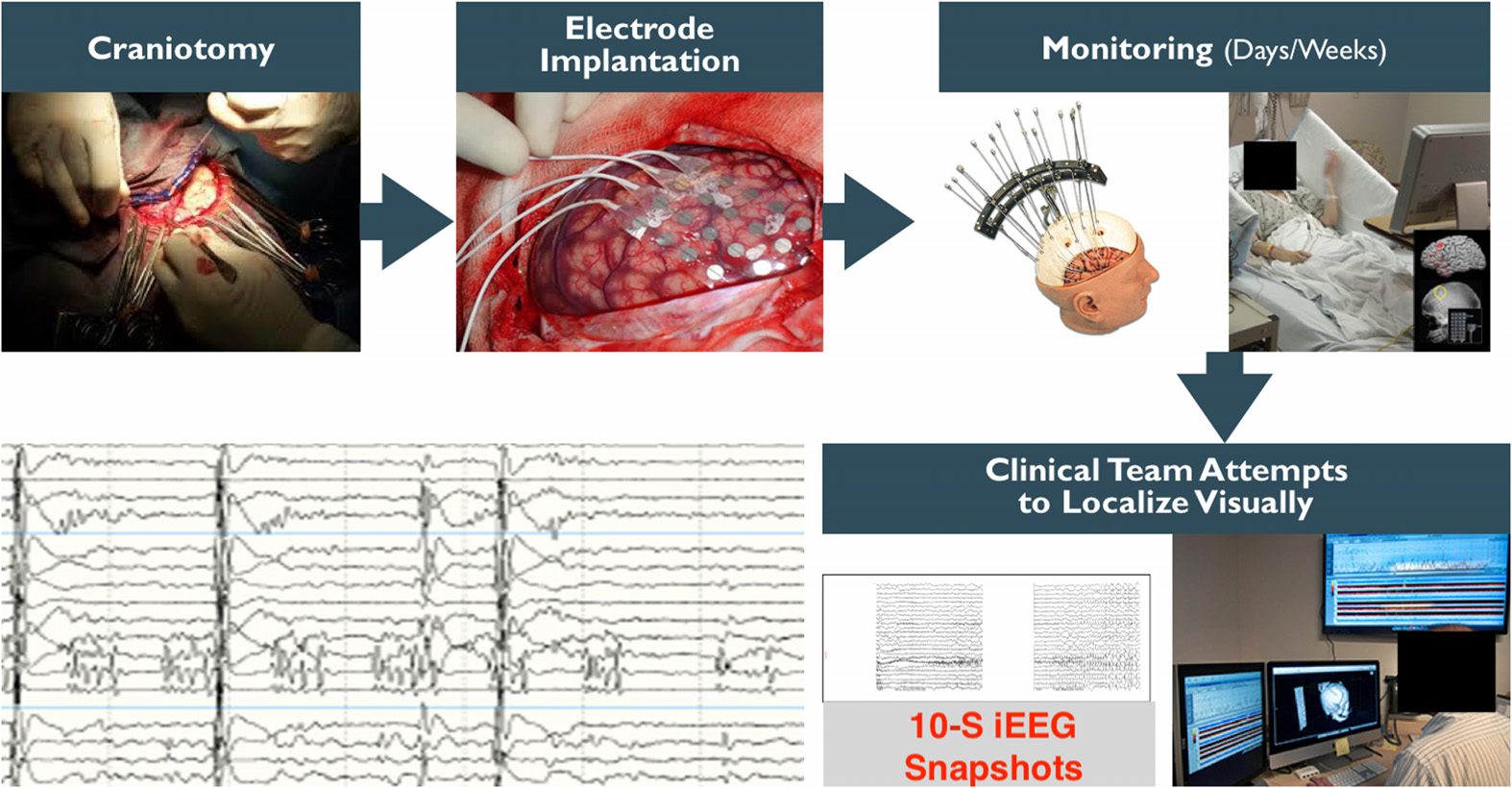
Figure 1. Clinical process for implantation of SDE and seizure onset localization. Clinicians
expose the brain through a craniotomy, then implant electrodes on the cortical surface of the brain,
monitor patient electrocorticography (ECoG) for days/weeks, and then attempt to localize the EZ
visually. Clinical teams look at recorded data on computers and annotate signals from certain
electrodes and time periods.
Network Neuroscience
220
Network analysis to localize the epileptogenic zone
Principal component analysis (PCA):
A dimensionality reduction
technique commonly used in data
analysis.
qHFO:
A quality high-frequency oscillation
(i.e., highly likely to be an actual
HFO) detected by an algorithm
described in the paper.
relate the eigenvector centrality (EVC) patterns back to clinically annotated EZ in patients with
both successful and failed outcomes. We recently demonstrated that intracranial EEG (iEEG)
is rich in network information beyond the typical signatures clinicians use to identify the EZ
In par-
(Burns et al., 2014; Kerr et al., 2011; Santaniello et al., 2011; Yaffe et al., 2012).
ticular, we modeled the epileptic brain as a dynamic networked system where EEG signals
are correlated both temporally and spatially. We constructed a set of network-based statistics
whose temporal evolution distinguishes the epileptic nodes from the nonepileptic nodes within
specific epileptic networks, thus defining an electrophysiological signature of the EZ (Kerr
et al., 2011; Yaffe et al., 2012). The electrophysiological signature of the EZ has a character-
istic arch shape when visualized in a two-dimensional principal component (2D PC) space
described below. The arch shape is significant because it indicates that the electrodes have
lower centrality before a seizure, become highly central during a seizure, and then become
less central after seizure offset. This suggests that the EZ is a brain region that becomes highly
centralized when seizures occur, recruiting many other brain regions to participate in epileptic
activity. We used these time series network-based statistics and the identified EZ arch signa-
ture to develop an algorithm that takes as inputs iEEG data and the patient’s brain image after
electrode implantation and outputs the likelihood of an electrode being in the EZ.
We hypothesized that a network-based algorithm will show higher degrees of agreement
with the clinically labeled EZ for successful surgical outcomes and lower degrees of agreement
with the labeled EZ for failed surgical outcomes. Our hypothesis is based on our expectations
that a network-based algorithm will perform favorably because epilepsy is a network disease of
the brain and simply looking at biomarkers of individual electrodes ignores this fact. To test our
hypothesis, we evaluated our algorithm in a blind, retrospective study on 42 patients that had
undergone invasive monitoring and in most cases were followed by surgery. EEG data on one
to three seizures were analyzed by our algorithm without knowledge of the seizure outcomes.
Clinically identified EZ nodes were then compared with the most central nodes as defined
by our algorithm. We found that the algorithm agreed more with clinical annotations for
patients with successful surgical outcomes and less for patients with failed surgical outcomes.
Since HFO is considered a gold standard for localization of high-frequency power, we wanted
to compare our results with such a method. We also applied qHFO algorithm presented in
Gliske et al. (2016) to all patients whose EEG recordings met the requirements of the qHFO
algorithm. We found that there were many patient datasets that could not be easily applied to
the qHFO algorithm because of limitations on data available and sampling rates of equipment.
However, on the datasets that could be compared with our network algorithm, there was a
higher degree of agreement (DOA) with clinicians using a network algorithm versus only the
qHFO algorithm.
Localization of the EZ is currently a time-consuming process since clinicians and techni-
cians visually inspect fairly large datasets. In today’s data science era, it is important to develop
and test computational tools to assist in localization of the EZ. An assistive computational tool
would not only likely reduce extraoperative monitoring time in the EMU, thereby cutting med-
ical costs and decreasing complications associated with invasive monitoring, but could also
improve seizure freedom rates, especially in the more difficult to localize patients (i.e., non-
lesional MRI patients). In addition, the underlying network-based algorithm that performs EZ
detection favorably will further our understanding of the organization and dynamics of brain
networks in epilepsy disease. Our results suggest that epilepsy changes how the different nodes
in the brain are connected, and that diseased nodes are more likely to be highly central in the
neuronal network and have a high centrality signature.
Network Neuroscience
221
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
METHODS: DATA COLLECTION
Patients included in this study were surgically treated for medically intractable seizures at four
different centers: the Johns Hopkins Hospital (JHH), the National Institute of Health (NIH),
the University of Maryland Medical Center (UMMC), and the Cleveland Clinic (CC). All pa-
tients included in this study underwent invasive presurgical monitoring with either subdural
grid-and-strip arrays or stereotactic EEG depth electrodes for seizure localization or mapping
of eloquent areas. Decisions regarding the need for invasive monitoring and the placement of
electrode arrays were made independently of this work and solely based on clinical necessity.
The research protocol was reviewed by the Johns Hopkins Institutional Review Board (IRB), the
National Institute of Neurological Disorders and Stroke IRB, the University of Maryland Medi-
cal Center IRB, and the Cleveland Clinic IRB. The acquisition of data for research purposes was
done with no impact on the clinical objectives of the patient stay. Digitized data were stored
in an IRB-approved database compliant with Health Insurance Portability and Accountability
Act (HIPAA) regulations (e.g., server hosted behind a firewall with SFTP and SSH access).
At all four centers, as part of routine clinical care, up to three board-certified epileptol-
ogists marked, by consensus, the unequivocal electrographic onset of each seizure and the
period between seizure onset and termination. The seizure onset was indicated by a variety of
stereotypical electrographic features, which include, but were not limited to, the onset of fast
rhythmic activity, an isolated spike or spike-and-wave complex followed by rhythmic activity,
or an electrodecremental response. Concurrently with the examination of the EEG recordings,
changes in the patients’ behavior were sought from the video segment of video-EEG recordings.
For each patient, we combined surgical notes about the electrodes corresponding to resected
regions and postoperative follow-up information about how the resection affected the patient’s
seizures. The surgery was deemed a success and the resected area determined to include the
EZ if, at least six months after surgery, a patient reported no seizures or could manage their
epilepsy with medications. Failure was defined as the inability to localize the EZ at all, or if
the patient continued to have seizures that were not manageable with medications after the
resection.
IEEG recordings were acquired through subdural grid arrays, subdural strip electrodes, or
depth-electrode arrays in various combinations as determined by clinical assessment for pa-
tients with temporal, occipital, or frontal lobe seizures. Subdural grids have 20–64 contacts per
array and were used in combination with subdural strips with 4–8 contacts or depth arrays,
thus having 80–116 recording electrodes per patient overall. Intracranial contact locations
were documented by postoperative CT coregistered with a preoperative MRI. Signals were
acquired using continuous multichannel iEEG recordings collected over 5 days on average
(min.: 2 days; max: 10 days). Clinical monitoring lasted 5–10 days per patient and included
two to seven clinical seizures. Then clinicians clipped what they deemed clean sets of data
and passed it through a secure transfer for the data analysis.
There were a total of 42 subjects analyzed retrospectively in this study: 7 from NIH, 20
from JHH, 7 from UMMC, and 8 from the Cleveland Clinic. There were 26 total successful
surgeries and 16 total failed surgeries. The total number of electrodes per patient was 111.86 ±
23.89. The total number of electrodes used in analysis per patient (after removal of noisy/faulty
channels, references, EKG, etc.) was 70.82 ± 24.84. The size of the clinically annotated EZ
(# electrodes) was 8.05 ± 4.34. The onset age was 17.21 ± 13.48 years old, while all patients
now are 34.68 ± 12.30 years old. The subject groups for each center are shown in Figure 2.
Network Neuroscience
222
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
Figure 2. Patient cohort population for different recording systems, and across different hospital
centers. Shows the distribution of successful and failed outcomes for each center.
NIH Intracranial EEG Monitoring Technique: ECoG
Seven patients included in this study were surgically treated for drug-resistant seizures at the
NIH National Institute of Neurological Disorders and Stroke and underwent invasive presur-
gical monitoring with subdural grids for seizure localization or mapping of eloquent areas.
Recordings were acquired with a Nihon Kohden clinical EEG system. IEEG signals were sam-
pled at a 1 kHz sampling rate and filtered using a 300 Hz antialiasing filter. Signals were
referenced to a common contact placed subcutaneously on the scalp, on the mastoid process,
or on the subdural grid. Each data file stores continuous iEEG data from all channels and is
automatically generated by the acquisition system.
Johns Hopkins Hospital Intracranial EEG Monitoring Technique: ECoG
Twenty patients included in this study were surgically treated for drug-resistant seizures at the
Johns Hopkins Hospital and underwent invasive presurgical monitoring with subdural grid and
strip arrays for seizure localization or mapping of eloquent areas. Recordings were acquired
with a Nihon Kohden clinical EEG system with a 1 kHz sampling rate and a 300 Hz antialiasing
filter, and were converted to EDF format for storage and further processing. Each EDF file stores
approximately 42 min of continuous ECoG data from all channels and is automatically gen-
erated by the acquisition system. Consecutive EDF files cover consecutive, nonoverlapping,
time windows with less than 5s-lag in between. Digitized data were stored in an IRB-approved
database compliant with HIPAA regulations.
UMMC Intracranial EEG Monitoring Technique: ECoG
Seven patients included in this study were surgically treated for drug-resistant seizures at the
University Maryland School of Medicine and underwent invasive presurgical monitoring with
subdural grid and strip arrays for seizure localization or mapping of eloquent areas. At the Uni-
versity of Maryland Medical Center (UMMC), recordings were acquired with a Natus/XLTEK
Inc., USA) with 250–1,000 Hz sampling rate and
system (Natus Medical Incorporated,
Network Neuroscience
223
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
t
/
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
50–300 Hz antialiasing filter, and were converted to EDF format for storage and further pro-
cessing. Each EDF file stores approximately 42 min of continuous ECoG data from all channels
and is automatically generated by the acquisition system. Consecutive EDF files cover consec-
utive, nonoverlapping, time windows with less than 5s-lag in between. Digitized data were
stored in an IRB-approved database compliant with HIPAA regulations.
Cleveland Clinic Stereotactic EEG Monitoring Technique: SEEG
Eight patients that underwent SEEG invasive monitoring from the Cleveland Clinic epilepsy
center were included in this study. The choice of electrode location was based on a preim-
plantation patient management conference and was made independently of the present study.
Criteria for patients undergoing SEEG implantation were reviewed by clinicians to determine
patient eligibility for enrollment in the current study. If the patient met study criteria, research
staff not involved in the surgery implantation or postsurgical care contacted the patient for
potential participation in the study.
For each subject, approximately 8–13 stereotactically placed depth electrodes were im-
planted. The electrode contacts were 0.8 mm in diameter, 2 mm in length, and spaced 1.5 mm
apart. Depth electrodes were inserted in either orthogonal or oblique orientations using a
robotic surgical implantation platform (ROSA, Medtech Surgical, Inc., USA) allowing intracra-
nial recording from lateral, intermediate, and/or deep cortical and subcortical structures in a
three-dimensional arrangement (González-Martínez et al., 2016). The day prior to surgery, vol-
umetric preoperative MRIs (T1, contrasted with Multihance 0.1 mmol/kg) were obtained and
used to preoperatively plan electrode trajectories. All trajectories were evaluated for safety;
any trajectory that appeared to compromise vascular structures was adjusted appropriately
without affecting the sampling from areas of interest.
SEEG electrophysiological data were acquired using a conventional clinical electrophysi-
ology acquisition system (Nihon Kohden 1200, Nihon Kohden America, USA) at a sampling
rate of 1 kHz and 300 Hz antialiasing filter. Behavioral event data were simultaneously ac-
quired during behavioral experiments along with the SEEG electrophysiology and stored for
subsequent analysis. All signals were referenced to a contact affixed to the skull. Archived
electrophysiological data were not filtered prior to offline analysis.
Each patient had electrode contacts characterized according to anatomical location. The
anatomical locations of all contacts were identified through inspection of postoperative imag-
ing, requiring agreement by two clinical experts. An example of postoperative imaging con-
tributing toward determining contact location is shown in Figure 1. Coronal and sagittal views
were available for every contact.
METHODS: COMPUTATIONAL STEPS
In this study, our raw dataset consisted of EEG recordings of seizures with 60 s of data be-
fore and after each seizure. Data were collected from 42 patients with at least two seizures
per patient. We applied network analysis techniques and considered each electrode in the
iEEG array to be a node in a network. The overall process of our algorithm is highlighted in
Figure 3. We computed the cross-power spectrum matrix for each time window, then the cor-
responding EVC, and then we trained a Gaussian weighting function that assigned a likelihood
to each electrode for being within the EZ. After computing the heat map for the EZ predicted
set of electrodes, we compared them to the clinical electrodes for both successful and failed
surgical outcomes. We show results for each center separately, and also all patients grouped
224
Cross-power spectrum:
The Fourier transform between two
pairs of iEEG time series (i.e., two
different channels).
Gaussian weighting function:
A Gaussian distributed function that
applies weights to different points in
the PCA space.
Network Neuroscience
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
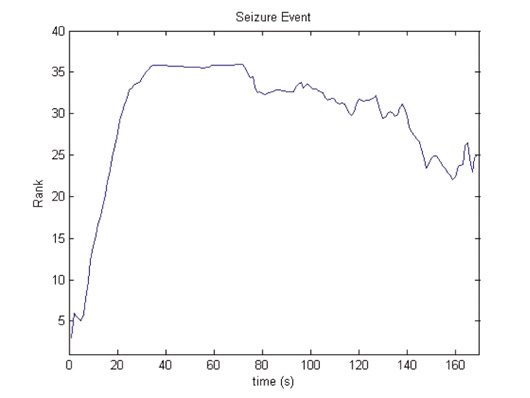
Figure 3. Computational steps for seizure onset localization: the algorithm processes raw ECoG to
compute the sequence of adjacency matrix A(t). From this sequence, A(t), it computes the sequence
of leading eigenvectors, v(t), as a network centrality measure, the EVC. Algorithm then converts EVC
into the sequence of rank centrality r(t). From this sequence, r(t), algorithm computes a heatmap
that generates predictions of the EZ. Yellow shading indicates the EVC of the first electrode evolving
in time whose rank centrality, r1(t), is illustrated in the plot.
together. Note that we trained the Gaussian weighting function only using one center’s pa-
tients, so that we could test our results across center. Clinical procedures can vary more from
center to center versus the variability within center, so it is a conservative approach to train
using one center and then test on all other centers to see whether our analysis holds across
different clinical procedures. All Matlab (R2016b) and Python (v 2.7) code is publicly available
online at Li (2018).
Preprocessing of Data
All data underwent digital filtering with a butterworth notch filter of order 4, implemented in
Matlab with the f ilt f ilt function (frequency ranges of 59.5 to 60.5). In general, EEG data are
known to be noisy and referencing schemes can play a significant role in downstream data
analysis. We decided to apply a common average referencing scheme to the data before
analysis (Ludwig et al., 2009). Here, we take an average signal from all recording electrodes
and subtract it from the electrodes. This has been shown to produce more stable results and
rejects correlated noise across many electrodes (Gliske et al., 2016). We made sure to ex-
clude any electrodes from subsequent analysis if they were informed to have artifacts in their
recording by clinicians.
Compute and Rank Nodal Centrality Over Time
Network centrality for each node was computed every second using a 2.5 s sliding window
sliding every second 60 s before seizure, during seizure, and 60 s after seizure for at least two
seizure events. For each window, the brain network was first represented by a connectivity
Common average referencing:
An EEG referencing scheme in which
a sample average of all the recording
sites is taken and is used as the
reference signal for all electrodes.
Network Neuroscience
225
Network analysis to localize the epileptogenic zone
matrix (Fisher, 2012), by computing all pairwise cross-power spectra between the signals in
the gamma frequency band (30–90 Hz); that is,
Aij =
(cid:2) 90Hz
30Hz
(Pi( f )Pj( f ))d f ,
(1)
where Pi, Pj are the magnitudes of the Fourier transform of the time series in the window
recorded from electrodes i, j, and Aij is the element of connectivity matrix and is the adjacency
between nodes i and j. We chose the gamma band because the gamma frequency band has
often exhibited the most modulation in power between nonseizure and seizure periods. It has
been thought to be correlated to neuronal spiking and fMRI activity and thus carries information
in such invasive recordings (Gotman, 1983; Worrell et al., 2004; Wu & Gotman, 1998).
The importance of each electrode to the network connectivity was measured by the strength
and number of connections it makes with other electrodes, referred to as centrality. We used
the eigenvector centrality (EVC) to measure the connectivity of each electrode, as EVC showed
interesting repeatable patterns over seizure events in our prior study (Burns et al., 2014). The
EVC of an electrode is defined as the sum of the EVCs of all other electrodes weighted by their
connectivity, which measures the relative influence of a node within the network. The EVC of
all electrodes is computed implicitly as
EVC(i) = λ
N
∑
j=1
AijEVC(j).
(2)
λ is the leading eigenvalue of the connectivity matrix A and the EVC is then the leading
eigenvector of A. In simple terms, the EVC of a node in the network (electrode) is proportional
to the sum of EVCs of its neighbors (nodes it is connected to). That is, a node is important if it
is (a) connected to a few nodes that are themselves very important or if it is (b) connected to a
very large number of not-so-important nodes. The leading eigenvectors of connectivity matri-
ces were calculated numerically at each second during the recordings from the connectivity
matrices. Finally, the EVC vector for each second was converted to a ranked vector containing
values 1 to N, where a 1 was placed in the component of EVC that had the smallest centrality
and an N was placed in the component of EVC that had the largest centrality.
Normalize Rank Evolution Signals
Next, we normalized the rank evolution signals (the EVC) for each electrode in the X (time) and
Y (rank centrality, i.e., number of electrodes) directions. This was done so that we can compare
signals from different patients that have varying numbers of electrodes and varying seizure
durations across individuals and within individuals. To normalize along the X-axis, we either
stretched (interpolated) or shrunk (simply downsampled at a lower sampling rate) each ranked
EVC signal during a seizure epoch such that all signals were 500 data points in length. Most
ranked EVC signals were under 500 s in length, so the majority of the rank centrality signals
were stretched using linear interpolation (using the interp1 function in Matlab) preserving the
shape of the signal during a seizure event. To normalize along the Y-axis, we scaled the rank
centrality between 0 and 1 by dividing by the number of electrodes. Further, in order to
compare the ranked EVC in a quantifiable manner, we normalized all the X, Y normalized
signals such that the centrality signal integrated to 1. We divided the normalized rank centrality
Network Neuroscience
226
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
by area under the curve. This normalization converted each signal into a probability density
function,
R(¯t) = EVC(t)/N,
(3)
¯t
where R(¯t) is the normalized rank signal in time after dividing by the number of electrodes
and ¯R(¯t) is the normalized rank signal at normalized time ¯t.
(4)
¯R(¯t) =
(cid:3)
R(¯t)
R(¯t) ¯dt
,
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Compute Feature Vector From Normalized Rank Signals
For each normalized signal, we extracted the deciles in time, the locations at which the signal
integrates equally to 10% of the total area under the curve, that is, points in normalized time
where the signal integrates to 0.1, 0.2, 0.3, and so on until the end of the signal is reached.
This gives a 10-dimensional vector for each signal that serves as a feature vector.
Electrode Weight Assignment Based on Feature Vectors
Once we calculated feature vectors for each signal, we projected the features into a 2D princi-
ple component (PC) space. This was done by assuming that each feature vector is an observa-
tion, hence the analysis was performed in space x time. We performed PC analysis and plotted
the features across all electrodes and patients projected onto the first and second PCs. Each
electrode (data point in Figure 4A) was labeled according to whether the electrode was in the
clinical annotated EZ region and whether the surgical resection was a success or a failure. We
then created a weighting function over the 2D PC space, which would assign a weight to an
electrode based on their location in PC space.
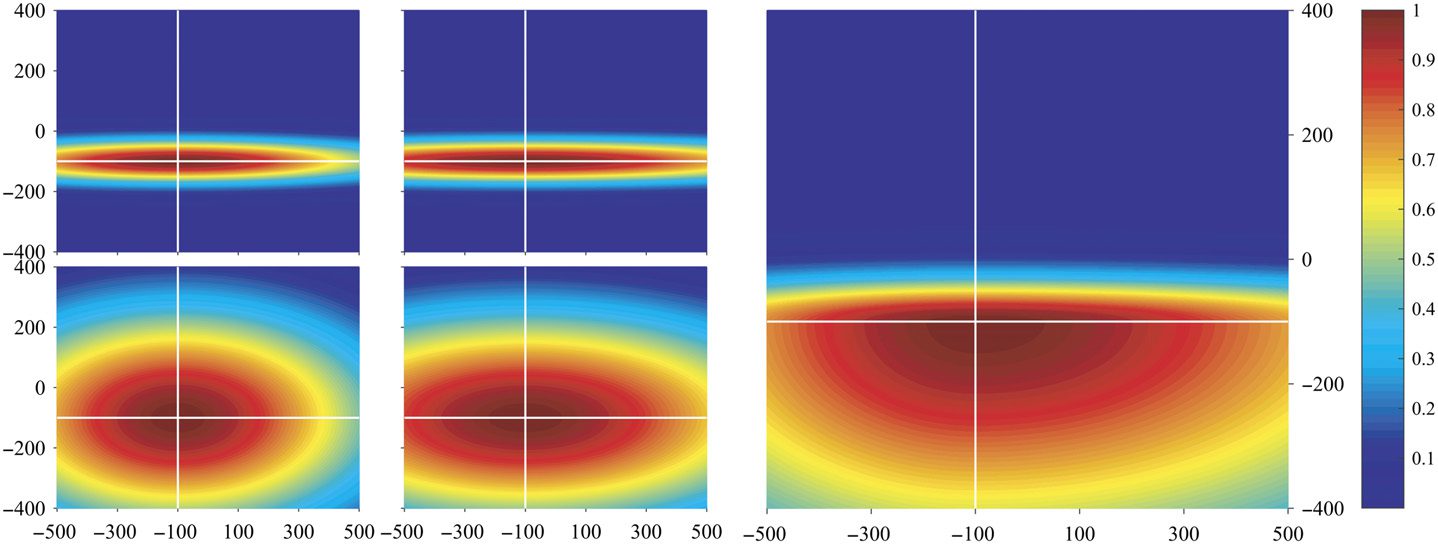
To generate this weighting function, we discretized it into equally sized square partitions
(100 × 100 along first and second principal components). The mean normalized rank signature
across all data points was computed for each partition. The signatures for the four corner
partitions are shown in Figure 4A. The shapes of the mean normalized rank signatures across
partitions change in a somewhat continuous manner. Moving vertically from the bottom of the
PC space to the top, the rank signatures transition from a concave to a convex shape. Moving
from left to right, the signature shifts horizontally: forward (to the right) if the partition is at the
bottom of the PC space, and backward (to the left) if at the top of the PC space.
Our hypothesis is that the arch signature displayed in the bottom left of Figure 4A represents
the signatures of the EZ because this is the region of the PC space that has the most isolated
channels that come from patients with successful outcomes (green + points). In fact, the bot-
tom portion of the PC grid shows the arch signature. Therefore, the weighting function is set
to be highest in these regions and decay as a function of distance from these regions. We de-
fined a weighting function to be the sum of four bivariate Gaussian-like functions (Equation 5,
Figure 4B) as shown in Equation 5. The 2D PC space is divided into four quadrants defined by
an origin. See Figure 4B (left) with origin (−100, −100).
Training Origin of Gaussian Weighting Function
Leave-one-out:
A training procedure for an algorithm
that leaves one data point out during
a pass-through of the training.
In each quadrant, the bivariate Gaussian-like function was initialized with the shapes in
Figure 4A. The covariance matrix in each quadrant was computed as the sample covariance
from the data points in that quadrant. The origin of the four quadrants is the mean vector,
which is trained. We followed a leave-one-out training procedure on the sample of 20 patients
Network Neuroscience
227
Network analysis to localize the epileptogenic zone
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
t
/
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
(A) First and second PCA component distribution. Points in PC space: 1. Green +: re-
Figure 4.
sected electrodes in successful outcomes, 2. Red •: nonresected electrodes in successful outcomes,
3. Black +: resected electrodes in failed outcomes, and 4. Black •: nonresected electrodes in failed
outcomes. The plots in each of the four insets show the mean normalized rank centrality signal for
points in the regions bounded by orange rectangles. The shaded regions in the plots indicate the
1 standard deviation bounds. The green and red lines in the plots indicate the start and end of a
seizure episode, respectively. The yellow circle highlights the region of interest, where there are
many green markers. (B) An example of the Gaussian weighting function, where the color repre-
sents the weight of an electrode being within the EZ. The four plots in the left-hand side represent
the Gaussian weighting function for each quadrant, respectively. The right-hand plot is the sum of
the four Gaussian functions, which gives the final Gaussian weighting function.
Network Neuroscience
228
Network analysis to localize the epileptogenic zone
collected at JHU. We chose JHU because it had the greatest number of patients collected within
center and would still account for less then 50% of the total patients. The mean of all four quad-
rants is optimized for maximizing the DOA. In Figure 4B, this is shown as (−100, 100), which
was found at the end. Once the optimized mean is found, then all four quadrants’ Gaussian
functions, wi(x, y), are linearly combined with a Heaviside step function to get the final Gaus-
sian weighting function, w(x, y). This final Gaussian weighting function, w(x, y), is used to
assign weights to all subsequent EVC of each electrode for every patient. This in turn produces
the likelihood of every electrode being within the EZ set.
w(x, y) =
4
∑
i=1
hi(x, y)wi(x, y),
where
(cid:4)
wi(x, y) = exp
αi – exponential decay factor for ith quadrant;
(cid:7)
−αi(x − µ)T ∑−1
(x − µ)
(cid:7)
(cid:6)
(cid:6)
;
i
(cid:5)
x −
x
y
, and µ −
μx
μy
define the position and mean vector, respectively;
∑i – covariance matrix of ith quadrant;
hi(x, y) = Θ(x − μx)Θ(y − μy) – Θ is the heaviside step function; and
(x, y) ∈ ith quadrant.
Computing Degree of Agreement and Statistical Analysis
For every seizure event for every patient in NIH, UMMC, and CC, we generated a set of elec-
trodes with their heatmap (defined by electrode weights; see Figure 3), which can be inter-
preted as their likelihood for being in the EZ. For each seizure recording, we then computed
the degree of agreement between the computed EZ likelihoods and clinical annotations of the
EZ. The likelihood was computed using the Gaussian weighting function trained as described
in the previous subsection. Then, a threshold α = 0.3, 0.6, 0.9 was applied to each heatmap,
and the set of electrodes whose likelihoods exceeded α were defined as the algorithm’s EZ
(AEZ). The AEZ was then compared with clinically annotated EZ (CEZ) using the following
degree of agreement (DOA) statistic:
DOA =
(CEZ ∩ AEZ)
CEZ
−
(
¯CEZ ∩ AEZ)
¯CEZ
.
(6)
Note that ¯S is the complement of the set S, and that D ∈ [−1, 1], where DOA = 1 implies
perfect agreement and DOA < 0 is less agreement.
Across all patients, electrodes, and seizure events, we have a collection of DOA values. We
then derive two distributions: (a) the distribution of DOA for all electrodes implanted in patients
who had successful treatments, and (b) the distribution of DOA for all electrodes implanted
in patients who had failed treatments. We then test whether there is a significant difference in
DOA distribution between these two patient groups using the Wilcoxon rank sum test to test
for statistical differences. This nonparametric test was selected, as the data are not guaranteed
to meet the normality conditions for a Student’s t test (Whitley & Ball, 2002). In addition, we
also added an across-center analysis where we combine all the data and test whether the DOA
distributions for successful versus failed outcomes are significantly different.
Network Neuroscience
229
(5)
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
On top of this analysis, we also add a min-max scaling to normalize the degree of agree-
ments within each center, so that success and failure could be compared at the same scale.
High-Frequency Oscillator: qHFO Detector
We compared our algorithm with the qHFO algorithm presented in Gliske et al. (2016), which
uses a sensitive HFO detector, then redacts HFOs that were produced by artifacts. Previous
work has shown that sampling rates of 1000 Hz are capable of recording HFOs, but only cap-
ture 60% of the events Gliske et al. (2016). Therefore, we only analyzed patients with sampling
rates ≥ 1,000 Hz and with available interictal data. This resulted in three patients from NIH
and two patients from JHU, with a total of 13 separate recorded datasets. The datasets here
analyzed had an average recording of 7.1 min, 83 total electrodes analyzed, and 10 electrodes
within the clinically annotated EZ set. Using the qHFO algorithm on this data required a few
minor adaptions.
We used a single common average reference applied to all analyzed intracranial electrodes
(as described earlier), rather than separating the referencing between depth-electrode channels
and grid channels as was done in Gliske et al. (2016). The popDet artifact rejection method
also could not be used, as it requires sampling rates of at least 2,000 Hz.
RESULTS
Every patient (n = 42) with at least two seizures was analyzed (total of 113 seizures), with 20
of the patients from JHU used to train the final Gaussian weighting function. The output of
the process for each seizure recording is each electrode’s likelihood of being in the EZ. These
likelihood scores are in turn used to produce a heatmap that can be overlaid on a brain MRI
to show the relative predicted EZ region for a certain patient. Figure 5 shows a few examples
of heatmaps for three patients who had successful outcomes and three patients with failed
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
t
.
/
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
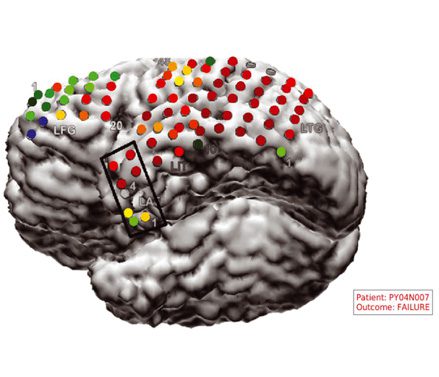
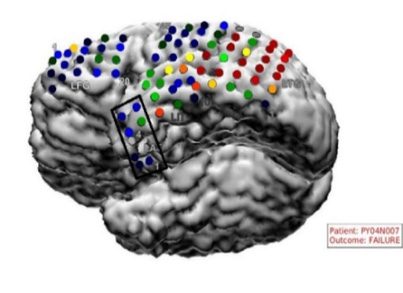
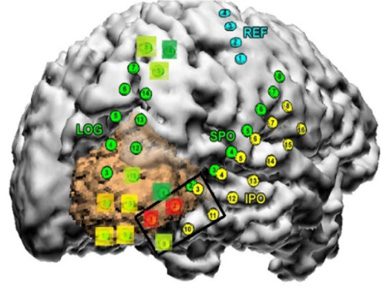
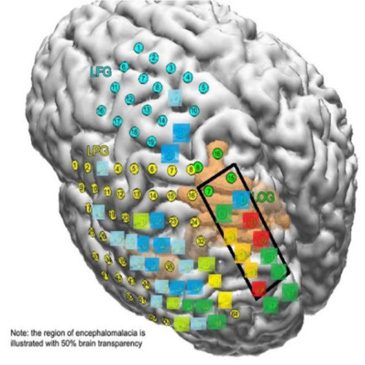
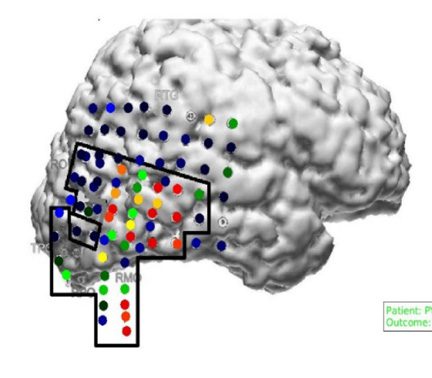
Figure 5. This figure shows an example overlay of the algorithm’s heatmap of likelihood on a
brain scan for six patients (three successful and three failed outcomes). The red region shows our
predicted onset zone and the black outlines represent where the clinicians performed a resection.
The orange, yellow, green, and blue regions represent lower likelihoods for that specific electrode
being within the EZ set as predicted by the algorithm.
Network Neuroscience
230
Network analysis to localize the epileptogenic zone
Table 1. HFO results for the two patients with interictal data from NIH. Only two datasets (two
patients) showed HFO rates not identically zero. Only one dataset had an HFO analysis with an
electrode within the clinically annotated set.
Patient
JH1
JH3
pt1aslp1
pt1aslp2
pt1aw1
pt1aw2
pt2aslp1
pt2aslp2
pt2aw1
pt2aw2
pt3aslp1
pt3aslp2
pt3aw1
Duration (seconds)
1,800
1,800
405
498
425
414
376
419
397
664
362
379
363
Identification by HFO
Rates identically zero
No anomalously high channels
Rates identically zero
Rates identically zero
Rates identically zero
Prediction has been made ‘AD1’
Rates identically zero
Rates identically zero
Rates identically zero
Rates identically zero
Rates identically zero
Prediction has been made ‘SFP6’
Rates identically zero
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
t
.
/
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
outcomes. For the three successful patients, the AEZ lies entirely within the resected regions,
suggesting a high DOA between the AEZ and CEZ. For one of the failed patients, the resected
region and the AEZ do not overlap, that is, DOA is low. For the other failed patient, the AEZ
is a very small set, suggesting that the EZ may not be appropriately covered by the electrode
implantation.
In our comparative HFO analysis, we analyzed 13 segments of data from five patients. Of
the 13 files, most patients have no HFOs, even at 1,000 Hz sampling rate (see Table 1). Only
three data segments had HFO detections, but one of them did not have an anomalous grouping
suggestive of the EZ (30% of the total recording time from all 13 data segments). In JH3, there
were HFOs, but no channels had an anomalous rate high enough to be predicted within the
EZ set. In NIH pt1aw2 and pt3alsp3, both only had a single channel predicted to be in the EZ.
This prediction was in concordance with clinically annotated EZ in pt1 but not in pt3.
The lower sampling rate and short time segments are not ideal for automated HFO analysis,
as is apparent from these results. In our network analysis, we had a high DOA with pt1 (0.62),
while a relatively lower DOA for pt3 (−0.16). It seemed that for pt3, HFO analysis completely
disagreed with clinical annotations, while the network analysis found more electrodes then
the clinically annotated EZ, which led to lower DOA. For pt1, the network analysis also high-
lighted the same electrode as being in the EZ set. This shows how HFO and network analysis
can complement each other in analyzing different sections of the data. Based on our limited
comparisons due to inherent data limitations, our analysis is more capable of identifying the
full clinically annotated EZ than HFOs in this specific dataset.
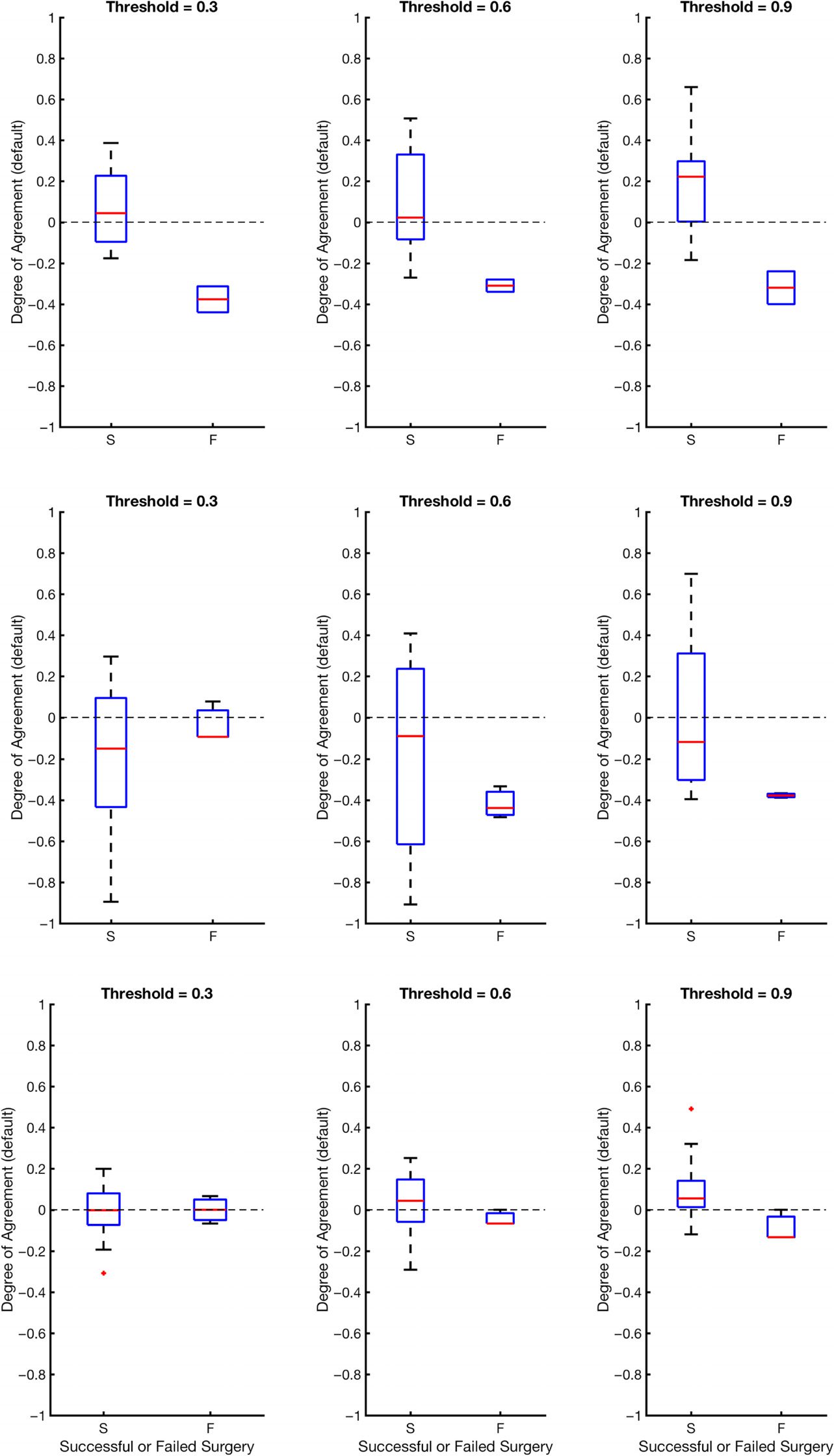
In Figure 6, we show the DOA for datasets collected from the test datasets (the three clin-
ical centers: UMMC, NIH, CC) for three different threshold values, α, that are placed on the
likelihood distribution (electrodes with likelihood greater then threshold are placed in the EZ
set). The resulting DOA after training the Gaussian weighting function for JHU are shown in
Supplementary Table 5 (Li et al., 2018). It also shows the same trend as seen in Figure 6. As
illustrated in Figure 6, the general trend is that the DOA distributions for successes and failures
separate more as α increases, and α = 0.9 appears to be an operative threshold that shows a
positive DOA for successes and a negative DOA for failed outcomes. For α = 0.9, the statistics
Network Neuroscience
231
Network analysis to localize the epileptogenic zone
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Figure 6. This figure shows degrees of agreement using the degree of agreement index between
our algorithm and clinical annotations for successful and failed surgical resections. The dashed line
at DOA = 0 represents neither agreement nor disagreement. The red line is the average DOA, and
the blue box is the box plot of the DOA; −1 is a perfect disagreement between the algorithm and
clinical set, while 1 is a perfect agreement between the algorithm and clinical set.
Network Neuroscience
232
Network analysis to localize the epileptogenic zone
Table 2. Degree of agreement results for α = 0.9 with average ± standard deviation from each
clinical center and also the resulting p value from the Wilcoxon rank-sum test. All centers show
a significant difference between success and failure cases. Note JHH is used in the training of the
Gaussian weighting function.
Center
UMMC
NIH
CC
*JHH
All
DOA statistics for success
0.09 ± 0.15
0.21 ± 0.25
0.01 ± 0.38
0.21 ± 0.23
DOA statistics for failure
−0.09 ± 0.08
−0.32 ± 0.11
−0.38 ± 0.01
0.08 ± 0.25
0.14 ± 0.27
0.00 ± 0.27
P value
0.027
0.020
0.024
0.016
0.002
for DOA (mean and standard deviation) are given in Table 2 for each center and across all
centers together. By applying a Wilcoxon rank-sum test, we also see a significant difference at
significance level 0.05 for all centers at threshold level of 0.9. At each center, there is a trend
of the DOA that is a function of clinical outcome of the patient. This is consistently shown
across recording platform (ECoG for UMMC, NIH and SEEG for CC) and patient population.
In all cases, as the threshold increases from 0.3 to 0.9, the difference of DOA between success-
ful and failed cases increases. If there is low DOA with the algorithms EZ and the clinically
annotated EZ and the patient is a failed outcome, then this may be a case of mislocalization.
If, on the other hand, there is no visible EZ from the algorithm (all weights are low), then the EZ
may not be in the vicinity of the electrode, suggesting a possible misplacement of electrodes.
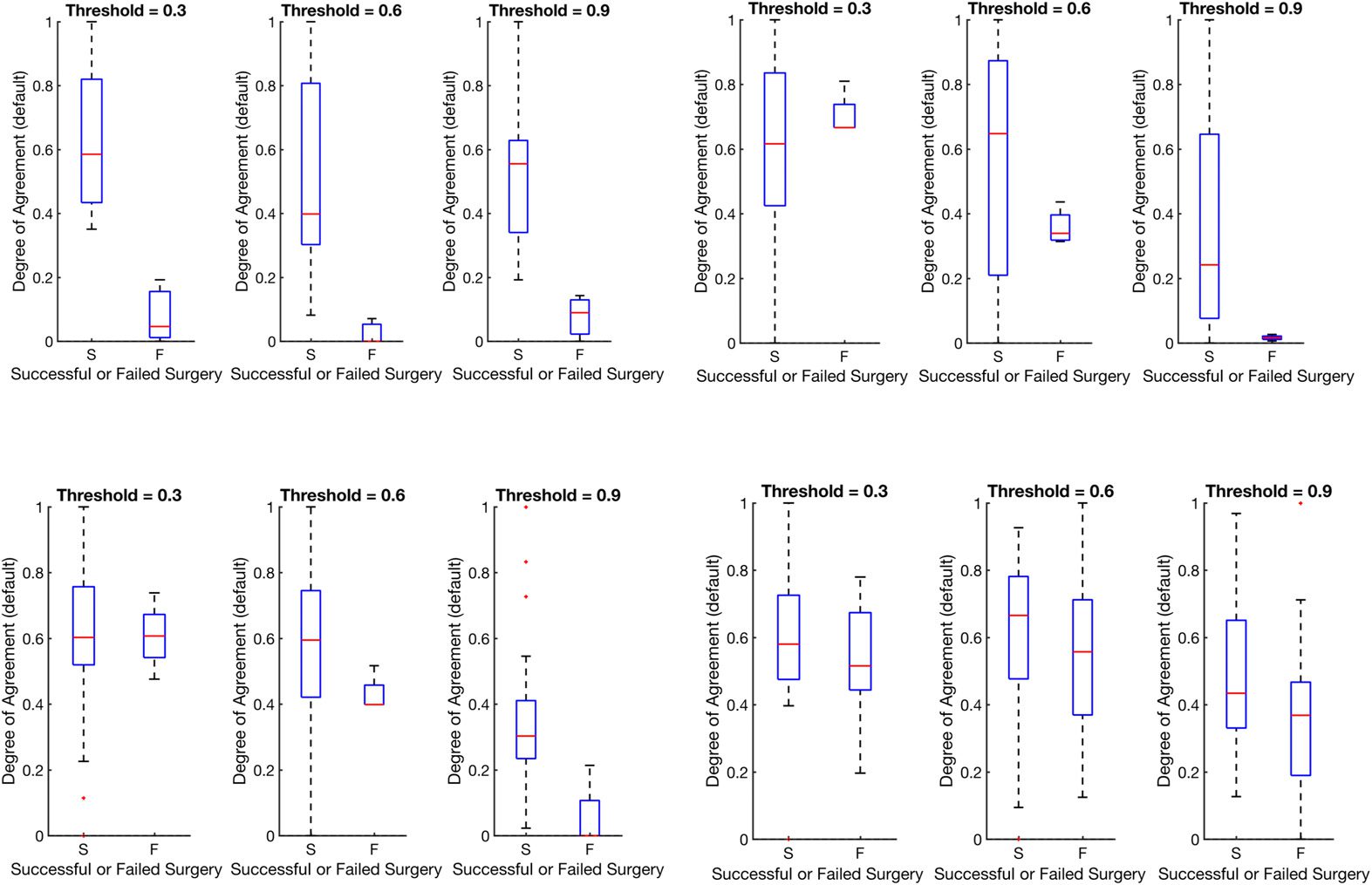
We also show in Figure 7 that there is no bias due to center (results are shown in Table 3.
All centers, when normalized, show a significant difference between successes and failures.
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Figure 7. This figure shows distributions of the degree of agreement for every center including JHU
after min-max normalization to compare each center on the same scale of success versus failure.
Note that min-max normalization scales all distributions between 0 and 1.
Network Neuroscience
233
Network analysis to localize the epileptogenic zone
Table 3. Degree of agreement results for α = 0.9 with average ± standard deviation from each
clinical center after min-max scaling and also the resulting p value from the Wilcoxon rank-sum
test. All centers show a significant difference between success and failure cases.
Center
UMMC
NIH
CC
*JHH
All
DOA statistics for success
0.35 ± 0.23
0.54 ± 0.23
0.36 ± 0.34
0.50 ± 0.23
DOA statistics for failure
0.05 ± 0.11
0.08 ± 0.07
0.02 ± 0.01
0.36 ± 0.24
0.45 ± 0.27
0.29 ± 0.25
P value
0.0057
0.0061
0.0016
0.0158
0.0005
The large variation is due to the varying number of electrodes implanted per patient and the
varying size of the clinical EZ hypothesis. However, all centers show significant difference
when compared with a Wilcoxon rank-sum test.
In the case that a patient has failed outcomes, we would not expect to see a perfect dis-
agreement DOA score of −1 because of the above reasons. There may have been no visible EZ
recorded from the electrode network, or the EZ may not have been fully resected (but part of it
was still clinically annotated). It is also important to note that when a patient has a successful
surgical outcome, clinicians remove a large portion of the brain, which is a superset of the
clinically annotated EZ. It is not certain that all clinically annotated EZ electrodes are actually
part of the true underlying EZ, so we would expect some deviation from perfect agreement
with the clinically annotated EZ (e.g., we should not expect to see a perfect DOA score of 1
for successful patients).
DISCUSSION
The definition of the EZ, including its anatomical and electrophysiological signatures, has been
an evolving and controversial topic since the foundation of modern epilepsy surgery. The EZ,
defined as the site of primary organization of the ictal discharge, refers to the cortical ar-
eas connected together through an excessive synchronization at seizure onset (Talairach &
Bancaud, 1973; Wendling, Chauvel, Biraben, & Bartolomei, 2010). Fast activity (FA) at ic-
tal onset has been clinically accepted as the main feature of the EZ since the beginning of
the invasive monitoring era, particularly in the SEEG literature (Talairach & Bancaud, 1973).
Since the development of subdural ECoG recordings, much attention has also been paid to the
time precedence of phasic transients, especially spiking activities (Boonyapisit et al., 2003;
Palmini et al., 1995). In the last 15 years, identification of high-frequency oscillations (HFO)
during interictal and ictal periods in experimental models reoriented research interest toward
high-gamma activities in human epilepsies as a potential EZ marker (Bragin et al., 2002;
Matsumoto et al., 2013; Zijlmans et al., 2012). In parallel, DC recordings exemplified the con-
fast and ultra-slow frequencies (Gnatkovsky et al., 2014; Ikeda et al., 1996;
comitance of
Thompson et al., 2016; Wu & Gotman, 1998), which could be used as potential biomarkers
of the EZ.
Although clinical definitions have been explored, a network-based operational definition
of the EZ is currently not well defined in the literature. Novel computational network analyses
may overcome some of the challenges associated with more conventional invasive monitoring
recordings methods. In this study, we analyze how centrality signatures of electrode recordings
within an epileptic network change over time and how they relate to clinical annotations from
Network Neuroscience
234
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
four different hospital centers. We take in ECoG and SEEG data from 60 s before and after a
seizure instance for 42 patients and produce a frequency connectivity network over time using
the cross-power spectra of the signal in the 30–90 Hz range. Then we computed the EVC for
each electrode at a time window to obtain a normalized ranked centrality of every electrode
over time. By overlaying a Gaussian weighting function that was trained only with patients
from one center, we then obtain a likelihood for each electrode of being in the EZ. Then we
computed a degree of agreement between our algorithm and clinically labeled EZ using the
DOA index for all patients by setting an arbitrary threshold.
Some previous approaches for marking the EZ included FA, signal flattening, and slow
potential shift. Fast activity frequently occurs quasisimultaneously in multiple areas so that
visual discrimination can be cumbersome and can lead to subjective interpretations. A differ-
ent approach, frequency localization, was used by Gnatkovsky et al. (2014). After defining
frequencies of interest (FOIs) and plotting their power change over time, they localized the
distribution of FOIs in different contacts of the depth electrodes. The EZ, defined as the area
exhibiting frequency changes at seizure onset, could then be delineated.
In a retrospective
and prospective study of patients investigated using SEEG, the same method was applied to test
three potential biomarkers of EZ, namely FA, signal flattening, and slow potential shift. These
biomarkers colocalized with the EZ as defined by standard SEEG criteria and postresection
seizure outcome (Gnatkovsky et al., 2014).
Other approaches for marking the EZ include HFO analyses.
Interictal HFOs have been
shown to have some value in identifying the EZ (Burnos et al., 2016; Jacobs et al., 2012;
Xiang, 2008; Malinowska, Bergey, Harezlak, & Jouny, 2015; Usui et al., 2011; Van Klink et al.,
2014). In our comparative analysis, we made modifications to the algorithm based on limita-
tions in the data that were available at the clinical centers. First, in the 1,000 Hz sampled data,
the number of HFOs is significantly reduced, although the detected HFOs are still useful to
identify the EZ (Gliske et al., 2016). The lower sampling rate also required some modifications
to the algorithm: the fast-transient artifact detector could not be used (as it requires sampling
rates > 2 kHz) and the upper edge on the band-pass filter needed to be reduced from 500
to 400 Hz. Second, the limitation to interictal data restricts the identification of the full EZ:
HFO results typically report a very small number of channels involved, which are typically
much smaller than the eventual resected volume of tissue. Although HFO analyses show
promise in analyzing electrophysiology of epileptic patients, they do not take into account the
network nature of epilepsy. HFO analyses are important for analyses of interictal data, since
our analysis is limited by requiring recorded seizure events.
In future studies, it would be
interesting to see how network algorithms and HFO algorithms can complement each other to
improve EZ localization.
It is important to note that network-based analyses are not new to analyzing EEG recordings
from epilepsy patients. Previous studies have shown that seizure activity is a dynamic multi-
channel process, and the correlation structure right around a seizure event also follows a typ-
ical evolution, similar to our ranked EVC signal (Kramer, Kolaczyk, & Kirsch, 2008; Schindler
et al., 2007).
In Kramer et al. (2008) and Schindler et al. (2007), they do not relate it back
to EZ, but just look at network dynamics during seizure events. In Schevon et al. (2007), the
authors compute interelectrode synchrony using the mean phase coherence algorithm and re-
late locally synchronous EEG channels back to the EZ, but analyzed only nine patients from
a single center. A similar small-scale study was performed in Korzeniewska et al. (2014) with
six epilepsy patients from one center. Other studies use computational models to understand
Network Neuroscience
235
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
.
t
/
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
the biophysical mechanisms related to epilepsy surgery (Khambhati et al., 2016; Sinha et al.,
2017).
In Khambhati et al. (2016), they applied a virtual resection model using data from
10 patients. In Sinha et al. (2017), the authors developed patient-specific dynamical network
models of epileptogenic cortex (computational models). However, there were only 16 patients
analyzed from one center.
This manuscript describes a somewhat large-scale research study that applies network-
based data analysis tools to invasive EEG data to explore possible EEG signatures of the EZ. In
no way are we proposing that this algorithm be directly translated into the clinic. Rather, it now
compares how pairwise correlations may improve over quantifying HFOs in each channel indi-
vidually, which has been the most recently accepted approach. We present a network analysis
related back to the annotated EZ, analyzing data from before and after seizures, and analyzing
data from multiple centers (with 113 seizures from 42 patients). In our study, we showed that
there is a general higher degree of agreement between our algorithm and clinically successful
surgical resections of the EZ and a lower degree of agreement between our algorithm and clin-
ically failed resections. By setting a simple threshold on the likelihood maps, we can obtain
a similarity measure between our algorithm and clinical labels for both successful and failed
surgeries. As the threshold increases, our algorithm becomes better at identifying whether suc-
cessful resections had the correct EZ. We observed that the algorithm’s performance degraded
with respect to degree of agreement when patients were implanted sparsely with single strips
across all four lobes (UMMC patients) and sometimes in both hemispheres. The clinicians
place these strips with such wide coverage if there is no clear preimplantation hypothesis and
if seizures are thought to be starting from multiple brain regions. Often, these patients do not
have clear EZ localization and/or do not end up as candidates for surgery. We also found that
if the electrographic onset of seizure is not close to the clinically annotated onset of seizure,
then the degree of agreement with clinicians is reduced. The electrographic onset is the start
of seizure that is seen on the EEG recordings but not manifested in any behavioral changes in
the patient. The clinical onset is the time at which the patient exhibits noticeable behavioral
changes due to seizure onset (e.g., muscle twitches).
Our results suggest that network data analytics may be a useful tool to assist in localization of
the epileptogenic zone, especially when electrode implantation covers the EZ network densely.
This is expected, since the threshold on the network’s likelihood is essentially a threshold
on the algorithm’s confidence in an electrode being within the EZ set. Future work entails
exploring different weighting functions applied over the rank centrality space and possibly
merging features from HFO and network algorithms. Besides looking solely at gamma power
(30–90 Hz) cross-power matrices, the work could expand to encompass more frequency bands
that could contain signals of importance in EZ localization. In addition, a more comprehensive
study that compares the outcomes between SEEG and ECoG could help understand limitations
of the algorithm, and also be of clinical importance in using SEEG versus ECoG. In addition, if
we had more patient data from other centers, then it would be interesting to see how a pooled
training procedure may improve our results. This work is meant to supplement the growing
evidence in the literature that epilepsy is a network phenomenon and therefore also requires
network algorithms to better understand its manifestation.
ACKNOWLEDGMENTS
We would like to thank the reviewers for their valuable advice.
Network Neuroscience
236
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
SUPPORTING INFORMATION
Code is open source at https://github.com/ncsl/eztrack. Since this was a retrospective data
study, there is no table of the JHU patients and their clinical operative notes because the data
were not available from JHU.
AUTHOR CONTRIBUTIONS
Adam Li: Formal analysis; Methodology; Software; Validation; Visualization; Writing –
original draft; Writing – review & editing. Sridevi Sarma: Conceptualization; Formal analysis;
Funding acquisition;
Investigation; Methodology; Project administration; Resources;
Supervision; Writing – original draft; Writing – review & editing. Robert Yaffe: Data cura-
tion. Bhaskar Chennuri: Conceptualization; Data curation; Formal analysis; Methodology;
Writing – original draft; Writing – review & editing. Kareem A. Zaghloul: Data curation;
Funding acquisition; Investigation; Writing – original draft; Writing – review & editing. Sara
Inati: Data curation; Funding acquisition; Writing – original draft; Writing – review & editing.
Jennifer Haagensen: Data curation; Writing – original draft; Writing – review & editing. Jennifer
Hopp: Data curation; Writing – original draft; Writing – review & editing. Emily Johnson: Data
curation; Writing – original draft; Writing – review & editing. Nathan Crone: Data curation;
Writing – original draft; Writing – review & editing. William Stan Anderson: Data curation;
Writing – original draft; Writing – review & editing. Zach Fitzgerald: Data curation; Writing –
original draft; Writing – review & editing.
Juan Bulacio: Data curation; Writing – original
John T. Gale: Data curation; Writing – original draft;
draft; Writing – review & editing.
Writing – review & editing.
Jorge Gonzalez: Conceptualization; Data curation; Writing –
original draft; Writing – review & editing. Austin Jordan: Formal analysis; Software. Sandya
Subramanian: Data curation; Formal analysis; Methodology; Software. Chalita Atallah: Data
curation; Writing – original draft; Writing – review & editing. Shubhi Agrawal: Data cura-
tion. Bobby Norton: Conceptualization; Software; Writing – review & editing. Steve Gliske:
Methodology; Validation; Writing – review & editing. William Stacey: Methodology; Valida-
tion; Writing – review & editing.
FUNDING INFORMATION
AL is supported by NIH T32 EB003383 and SVS by the Coulter Foundation and the Mary-
land Innovation Initiative. RY was supported by the Epilepsy Foundation Predoctoral Research
Training Fellowship. SVS, NC, and WSA are supported by Maryland Technology Development
Corportation (TEDCO) through MII. SVS was supported by the US NSF Career Award 1055560
and the Burroughs Wellcome Fund CASI Award 1007274. Data collection work was supported
by the Intramural Research Program at NIH.
REFERENCES
Bassett, D. S., & Bullmore, E.
(2006). Small-world brain net-
works. The Neuroscientist, 12(6), 512–523. https://doi.org/10.
1177/1073858406293182
Berg, A. T. (2009). Identification of pharmacoresistant epilepsy.
Neurologic Clinics, 27(4), 1003–1013. https://doi.org/10.1016/
j.ncl.2009.06.001
Begley, C. E., Famulari, M., Annegers, J. F., Lairson, D. R., Reynolds,
T. F., Coan, S., . . . Rocca, W. A. (2000). The cost of epilepsy in the
United States: An estimate from population-based clinical and
survey data. Epilepsia, 41(3), 342–351. https://doi.org/10.1111/
j.1528-1157.2000.tb00166.x
Berg, A. T., & Kelly, M. M. (2006). Defining intractability: Com-
parisons among published definitions. Epilepsia, 47(2), 431–436.
https://doi.org/10.1111/j.1528-1167.2006.00440.x
Boonyapisit, K., Najm,
I., Klem, G., Ying, Z., Burrier, C.,
LaPresto, E., . . . Lüders, H. (2003). Epileptogenicity of focal
Network Neuroscience
237
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
t
/
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
malformations due to abnormal cortical development: Direct
electrocorticographic-histopathologic correlations. Epilepsia, 44(1),
69–76. https://doi.org/10.1046/j.1528-1157.2003.08102.x
Bragin, A., Wilson, C. L., Staba, R. J., Reddick, M., Fried, I., & Engel,
J. (2002). Interictal high-frequency oscillations (80-500Hz) in the
human epileptic brain: Entorhinal cortex. Annals of Neurology,
52(4), 407–415. https://doi.org/10.1002/ana.10291
Braun, U., Muldoon, S. F., & Bassett, D. S.
(2015). On hu-
man brain networks in health and disease. In eLS (Vol. 22,
pp. 1–9). Chichester, UK: John Wiley & Sons. https://doi.org/10.
1002/9780470015902.a0025783
Brodie, M. J., Shorvon, S. D., Canger, R., Halasz, P., Johannessen,
S., Thompson, P., . . . Wolf, P. (1997). Commission on European
Affairs: Appropriate standards of epilepsy care across Europe.
Epilepsia, 38(11), 1245–1250. https://doi.org/10.1111/j.1528-
1157.1997.tb01224.x
Bulacio, J. C., Jehi, L., Wong, C., Gonzalez-Martinez, J., Kotagal,
P., Nair, D., . . . Bingaman, W. (2012). Long-term seizure out-
come after resective surgery in patients evaluated with intra-
cranial electrodes. Epilepsia, 53(10), 1722–1730. https://doi.org/
10.1111/j.1528-1167.2012.03633.x
Bullmore, E. T., & Bassett, D. S.
(2011). Brain graphs: Graphical
models of the human brain connectome. Annual Review of Clini-
cal Psychology, 7(1), 113–140. https://doi.org/10.1146/annurev-
clinpsy-040510-143934
Burnos, S., Frauscher, B., Zelmann, R., Haegelen, C., Sarnthein,
J., & Gotman, J. (2016). The morphology of high frequency os-
cillations (HFO) does not improve delineating the epileptogenic
zone. Clinical Neurophysiology, 127(4), 2140–2148. https://doi.
org/10.1016/j.clinph.2016.01.002
Burns, S. P., Santaniello, S., Yaffe, R. B., Jouny, C. C., Crone,
N. E., Bergey, G. K., . . . Sarma, S. V. (2014). Network dynamics
of the brain and influence of the epileptic seizure onset zone.
Proceedings of the National Academy of Sciences, 111(49),
E5321–E5330. https://doi.org/10.1073/pnas.1401752111
Deuker, L., Bullmore, E. T., Smith, M., Christensen, S., Nathan,
P. J., Rockstroh, B., & Bassett, D. S.
(2009). Reproducibility of
graph metrics of human brain functional networks. NeuroImage,
47(4), 1460–1468. https://doi.org/10.1016/j.neuroimage.2009.
05.035
Ferro, M. A., & Speechley, K. N. (2009). Depressive symptoms
among mothers of children with epilepsy: A review of preva-
lence, associated factors, and impact on children. Epilepsia,
50(11), 2344–2354. https://doi.org/10.1111/j.1528-1167.2009.
02276.x
Fisher, R. S. (2012). Therapeutic devices for epilepsy. Annals of
Neurology, 71(2), 157–168. https://doi.org/10.1002/ana.22621
Gilliam, F., Kuzniecky, R., Meador, K., Martin, R., Sawrie, S.,
Viikinsalo, M., . . . Faught, E. (1999). Patient-oriented outcome
assessment after temporal
lobectomy for refractory epilepsy.
Neurology, 53(4), 687–687. https://doi.org/10.1212/WNL.53.4.
687
Gilliam, F. G. (2005). Diagnosis and treatment of mood disorders
in persons with epilepsy. Current Opinion in Neurology, 18(2),
129–133. https://doi.org/00019052-200504000-00009[pii]
Gliske, S. V., Irwin, Z. T., Davis, K. A., Sahaya, K., Chestek, C., &
(2016). Universal automated high frequency
Stacey, W. C.
long term EEG. Clinical
oscillation detector
real-time,
Neurophysiology, 127(2), 1057–1066. https://doi.org/10.1016/
j.clinph.2015.07.016
for
Gnatkovsky, V., De Curtis, M., Pastori, C., Cardinale, F., Lo Russo,
G., Mai, R., . . . Francione, S.(2014). Biomarkers of epileptogenic
zone defined by quantified stereo-EEG analysis. Epilepsia, 55(2),
296–305. https://doi.org/10.1111/epi.12507
Gonzalez-Martinez,
J., Bulacio,
J., Alexopoulos, A.,
Jehi, L.,
Bingaman, W., & Najm, I. (2013). Stereoelectroencephalography
in the “difficult to localize” refractory focal epilepsy: Early expe-
rience from a North American epilepsy center. Epilepsia, 54(2),
323–330. https://doi.org/10.1111/j.1528-1167.2012.03672.x
González-Martínez,
J., Bulacio,
J., Thompson, S., Gale,
J.,
Smithason, S., Najm, I., & Bingaman, W. (2016). Technique,
results, and complications related to robot-assisted stereoelec-
troencephalography. Neurosurgery, 78(2), 169–179. https://doi.
org/10.1227/NEU.0000000000001034
Gotman, J. (1983). Measurement of small time differences between
EEG channels: Method and application to epileptic seizure prop-
agation. Electroencephalography and Clinical Neurophysiology,
56(5), 501–514. https://doi.org/10.1016/0013-4694(83)90235-3
J., Rutecki,
P., Bhattacharya, A., & Bell, B. (2006). Cognitive prognosis in
chronic temporal lobe epilepsy. Annals of Neurology, 60(1),
80–87. https://doi.org/10.1002/ana.20872
Hermann, B. P., Seidenberg, M., Dow, C.,
Jones,
Ikeda, A., Terada, K., Mikuni, N., Burgess, R. C., Comair, Y., Taki,
W., . . . Shibasaki, H. (1996). Subdural recording of ictal DC shifts
in neocortical seizures in humans. Epilepsia, 37(7), 662–674.
https://doi.org/10.1111/j.1528-1157.1996.tb00631.x
Jacobs, J., Staba, R., Asano, E., Otsubo, H., Wu, J. Y., Zijlmans,
M., . . . Gotman, J. (2012). High-frequency oscillations (HFOs)
in clinical epilepsy. Progress in Neurobiology, 98(3), 302–315.
https://doi.org/10.1016/j.pneurobio.2012.03.001
Jeha, L. E., Najm, I., Bingaman, W., Dinner, D., Widdess-Walsh, P.,
& Lüders, H. (2007). Surgical outcome and prognostic factors of
frontal lobe epilepsy surgery. Brain, 130(2), 574–584. https://doi.
org/10.1093/brain/awl364
Jeha, L. E., Najm, I. M., Bingaman, W. E., Khandwala, F., Widdess-
Walsh, P., Morris, H. H., . . . Lüders, H. O. (2006). Predictors
of outcome after temporal lobectomy for the treatment of in-
tractable epilepsy. Neurology, 66(12), 1938–1940. https://doi.
org/10.1212/01.wnl.0000219810.71010.9b
Jung, W. Y., Pacia, S. V., & Devinsky, O. (1999). Neocortical tempo-
ral lobe epilepsy: Intracranial EEG features and surgical outcome.
Journal of Neurophysiology, 16(5), 419. https://doi.org/10.1097/
00004691-199909000-00003
Kerr, M. S. D., Burns, S. P., Gale, J., Gonzalez-Martinez, J., Bulacio,
J., & Sarma, S. V. (2011). Multivariate analysis of SEEG signals
during seizure. Proceedings of the Annual International Confer-
ence of the IEEE Engineering in Medicine and Biology Society,
EMBS, 8279–8282. https://doi.org/10.1109/IEMBS.2011.6092041
Khambhati, A. N., Davis, K. A., Lucas, T. H., Litt, B., & Bassett,
D. S. (2016). Virtual cortical resection reveals push-pull network
control preceding seizure evolution. Neuron, 91(5), 1170–1182.
https://doi.org/10.1016/j.neuron.2016.07.039
Korzeniewska, A., Cervenka, M. C., Jouny, C. C., Perilla, J. R.,
(2014). Ictal
Harezlak, J., Bergey, G. K., . . . Crone, N. E.
Network Neuroscience
238
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
propagation of high frequency activity is recapitulated in interic-
tal recordings: Effective connectivity of epileptogenic networks
recorded with intracranial EEG. NeuroImage, 101, 96–113.
https://doi.org/10.1016/j.neuroimage.2014.06.078
Kramer, M. A., Eden, U. T., Kolaczyk, E. D., Zepeda, R., Eskandar,
E. N., & Cash, S. S. (2010). Coalescence and fragmentation of
cortical networks during focal seizures. Journal of Neuroscience,
30(30), 10076–10085. https://doi.org/10.1523/JNEUROSCI.6309-
09.2010
Kramer, M. A., Kolaczyk, E. D., & Kirsch, H. E. (2008). Emer-
gent network topology at seizure onset in humans. Epilepsy Re-
search, 79(2-3), 173–186. https://doi.org/10.1016/j.eplepsyres.
2008.02.002
Kwan, P., & Brodie, M. J. (2000). Early identification of refractory
epilepsy. New England Journal of Medicine, 342(5), 314–319.
https://doi.org/10.1056/NEJM200002033420503
. . . Gonzalez-Martinez,
Li, A. (2018). EZTrack, GitHub. https://github.com/ncsl/eztrack
Li, A., Chennuri, B., Subramanian, S., Yaffe, R., Gliske, S., Stacey,
W.,
J. (2018). Supplemental mate-
rial for “Using network analysis to localize the epileptogenic
zone from invasive EEG recordings in intractable focal epilepsy.”
Network Neuroscience, 2(2), 218–240. http://doi.org/10.1162/
netn_a_00043
Lüders, H. O., Najm, I., Nair, D., Widdess-Walsh, P., & Bingman,
W. (2006). The epileptogenic zone: General principles. Ep-
ileptic Disorders, 8(Suppl. 2). Retrieved from http://campus.
neurochirurgie.fr/IMG/pdf/versionPDFtheepilepticzone.pdf
Ludwig, K. A., Miriani, R. M., Langhals, N. B., Joseph, M. D.,
Anderson, D. J., & Kipke, D. R. (2009). Using a common average
reference to improve cortical neuron recordings from microelec-
trode arrays. Journal of Neurophysiology, 101(3), 1679–1689.
https://doi.org/10.1152/jn.90989.2008
Malinowska, U., Bergey, G. K., Harezlak,
J., & Jouny, C. C.
(2015). Identification of seizure onset zone and preictal state
based on characteristics of high frequency oscillations. Clinical
Neurophysiology, 126(8), 1505–1513. https://doi.org/10.1016/
j.clinph.2014.11.007
Matsumoto, A., Brinkmann, B. H., Matthew Stead, S., Matsumoto,
J., Kucewicz, M. T., Marsh, W. R., . . . Worrell, G. (2013).
Pathological and physiological high-frequency oscillations
in focal human epilepsy. Journal of Neurophysiology, 110(8),
1958–1964. https://doi.org/10.1152/jn.00341.2013
McIntosh, A. M., Kalnins, R. M., Mitchell, L. A., Fabinyi, G. C. A.,
Briellmann, R. S., & Berkovic, S. F. (2004). Temporal lobectomy:
Long-term seizure outcome, late recurrence and risks for seizure
recurrence. Brain, 127(9), 2018–2030. https://doi.org/10.1093/
brain/awh221
Murray, M. I., Halpern, M. T., & Leppik, I. E.
(1996). Cost of re-
fractory epilepsy in adults in the USA. Epilepsy Research, 23(2),
139–148. https://doi.org/10.1016/0920-1211(95)00090-9
Nair, D. R., Burgess, R., McIntyre, C. C., & Lüders, H. (2008).
Chronic subdural electrodes in the management of epilepsy.
Clinical Neurophysiology, 119(1), 11–28. https://doi.org/10.1016/
j.clinph.2007.09.117
Niedermeyer, E., & Lopes da Silva, F. H. (2004). Electroencephalog-
raphy: Basic principles, clinical applications, and related fields
(Vol. 1). Baltimore, MD: Urban & Schwarzenberg.
Önal, Ç., Otsubo, H., Araki, T., Chitoku, S., Ochi, A., Weiss, S.,
. . . Rutka, J. T. (2003). Complications of invasive subdural grid
monitoring in children with epilepsy. Journal of Neurosurgery,
98(5), 1017–1026. https://doi.org/10.3171/jns.2003.98.5.1017
Palmini, A., Gambardella, A., Andermann, F., Dubeau, F., da Costa,
J. C., Olivier, A., . . . Kim, H. (1995). Intrinsic epileptogenicity of
human dysplastic cortex as suggested by corticography and sur-
gical results. Annals of Neurology, 37(4), 476–487. https://doi.
org/10.1002/ana.410370410
Santaniello, S., Burns, S. P., Golby, A. J., Singer, J. M., Anderson,
W. S., & Sarma, S. V. (2011). Quickest detection of drug-resistant
seizures: An optimal control approach. Epilepsy and Behavior,
22(Suppl. 1). https://doi.org/10.1016/j.yebeh.2011.08.041
Isler,
J., Emerson, R.,
Schevon, C. A., Cappell,
J., Grieve, P.,
Goodman, R., . . . Gilliam, F. (2007). Cortical abnormalities in
epilepsy revealed by local EEG synchrony. NeuroImage, 35(1),
140–148. https://doi.org/10.1016/j.neuroimage.2006.11.009
Schindler, K., Leung, H., Elger, C. E., & Lehnertz, K. (2007). As-
sessing seizure dynamics by analysing the correlation structure
of multichannel intracranial EEG. Brain, 130(1), 65–77. https://
doi.org/10.1093/brain/awl304
Schuele, S. U., & Lüders, H. O. (2008). Intractable epilepsy: Man-
agement and therapeutic alternatives. The Lancet Neurology,
7(6), 514–524. https://doi.org/10.1016/S1474-4422(08)70108-X
See, S. J., Jehi, L. E., Vadera, S., Bulacio, J., Najm, I., & Bingaman,
W. (2013). Surgical outcomes in patients with extratemporal
epilepsy and subtle or normal magnetic resonance imaging
findings. Neurosurgery, 73(1), 68–76. https://doi.org/10.1227/
01.neu.0000429839.76460.b7
Sinha, N., Dauwels, J., Kaiser, M., Cash, S. S., Westover, M. B.,
Wang, Y., & Taylor, P. N. (2017). Predicting neurosurgical out-
comes in focal epilepsy patients using computational modelling.
Brain, 140(2), 319–332. https://doi.org/10.1093/brain/aww299
Talairach, J., & Bancaud, J. (1973). Stereotaxic approach to epi-
lepsy. In Progress in neurological surgery (Vol. 5, pp. 297–354).
Basel, Switzerland: Karger Publishers. https://doi.org/10.1159/
000394343
Thompson, P. J., Conn, H., Baxendale, S. A., Donnachie, E.,
McGrath, K., Geraldi, C., & Duncan, J. S. (2016). Optimizing
memory function in temporal lobe epilepsy. Seizure, 38, 68–74.
https://doi.org/10.1016/j.seizure.2016.04.008
Urbach, H., Hattingen, J., Von Oertzen, J., Luyken, C., Clusmann,
H., Kral, T., . . . Schild, H. H. (2004). MR imaging in the presur-
gical workup of patients with drug-resistant epilepsy. American
Journal of Neuroradiology, 25(6), 919–926. https://doi.org/25/6/
919 [pii] ET-2004/06/19
Usui, N., Terada, K., Baba, K., Matsuda, K., Nakamura, F., Usui,
K., . . . Inoue, Y. (2011). Clinical significance of ictal high fre-
quency oscillations in medial temporal lobe epilepsy. Clinical
Neurophysiology, 122(9), 1693–1700. https://doi.org/10.1016/
j.clinph.2011.02.006
Van Klink, N. E. C., Van’t Klooster, M. A., Zelmann, R., Leijten,
F. S. S., Ferrier, C. H., Braun, K. P. J., . . . Zijlmans, M. (2014).
High frequency oscillations in intra-operative electrocorticogra-
phy before and after epilepsy surgery. Clinical Neurophysiology,
125(11), 2212–2219. https://doi.org/10.1016/j.clinph.2014.03.
004
Network Neuroscience
239
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network analysis to localize the epileptogenic zone
Wendling, F., Chauvel, P., Biraben, A., & Bartolomei, F.
(2010).
From intracerebral EEG signals to brain connectivity: Identifica-
tion of epileptogenic networks in partial epilepsy. Frontiers in Sys-
tems Neuroscience, 4. https://doi.org/10.3389/fnsys.2010.00154
Whitley, E., & Ball, J. (2002). The sign test. Critical Care, 6(6),
509–513. https://doi.org/10.1186/cc1820
Widdess-Walsh, P., Jeha, L., Nair, D., Kotagal, P., Bingaman, W.,
& Najm, I. (2007). Subdural electrode analysis in focal cortical
dysplasia: Predictors of surgical outcome. Neurology, 69(7),
660–667.https://doi.org/10.1212/01.wnl.0000267427.91987.21
Wieser, H. G. (1998). Epilepsy surgery: Past, present and future.
Seizure, 7(3), 173–184. https://doi.org/10.1016/S1059-1311(98)
80032-0
Worrell, G. A., Parish, L., Cranstoun, S. D., Jonas, R., Baltuch, G.,
& Litt, B. (2004). High-frequency oscillations and seizure gener-
ation in neocortical epilepsy. Brain, 127(7), 1496–1506. https://
doi.org/10.1093/brain/awh149
Wu, L., & Gotman,
J. (1998). Segmentation and classification
of EEG during epileptic seizures. Electroencephalography and
Clinical Neurophysiology, 106(4), 344–356. https://doi.org/10.
1016/S0013-4694(97)00156-9
Xiang, J. (2008). Localizing functional brain cortices and epilep-
togenic zones with HFOs (Tech. Rep.). Cincinnati, OH: Chil-
dren’s Hospital Medical Center. Retrieved from http://www.
clinicalconnection.com/clinical-trials-from-other-databases/
study-details-from-other-databases/249846/37020000/
searchstudies.aspx?nav=expp
Yaffe, R., Burns, S., Gale, J., Park, H. J., Bulacio, J., Gonzalez-
Martinez, J., & Sarma, S. V. (2012). Brain state evolution dur-
ing seizure and under anesthesia: A network-based analysis of
stereotaxic EEG activity in drug-resistant epilepsy patients. In Pro-
ceedings of the Annual International Conference of the IEEE Engi-
neering in Medicine and Biology Society, EMBS (pp. 5158–5161).
IEEE. https://doi.org/10.1109/EMBC.2012.6347155
Zijlmans, M., Jiruska, P., Zelmann, R., Leijten, F. S. S., Jefferys,
J. G. R., & Gotman, J. (2012). High-frequency oscillations as a
new biomarker in epilepsy. Annals of Neurology, 71(2), 169–178.
https://doi.org/10.1002/ana.22548
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
–
p
d
l
f
/
/
/
/
0
2
0
2
2
1
8
1
0
9
2
1
9
3
n
e
n
_
a
_
0
0
0
4
3
p
d
/
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Network Neuroscience
240