V. Kasturi Rangan and R.D. Thulasiraj
Making Sight Affordable
Fallbeispiel „Innovationen“.: The Aravind Eye Care System
About 40 million people in the world are blind. The prevalence of blindness in
most industrialized countries of Europe and North America varies between 0.15%
Und 0.25%, compared with blindness rates of nearly 1.5% for the developing coun-
tries in Africa, Asia and Latin America. While age-related macular degeneration,
diabetic retinopathy, and glaucoma are the dominant causes in developed coun-
versucht, cataracts are the major cause of blindness in the developing countries,
accounting for nearly 75% of all cases in Asia.
A cataract forms as the natural lens of the eye clouds over time, and has to be
surgically removed and replaced by an artificial one. The causes of cataracts are
viele, but lack of proper nutrition and the effects of tropical weather are certainly
two of the more significant. In 2006, an estimated 20 million people were blind
from cataracts worldwide, mehr als 80% of them in developing countries.
In 2006, India had nearly 7 million cataract-blind individuals, with roughly 3.8
million new cases occurring annually.1 With a population of over a billion, und ein
per-capita income of about $600/year (PPP $3,600), nearly 25% of Indians were
considered to be below the poverty line, but much larger numbers (etwa
50%) were at income levels that would place treatment at private eye clinics
beyond their reach. In theory, anyone who is unable to afford payment is eligible
for free surgery at government-run district hospitals but in practice, a vast num-
ber of poor people prefer to pay a small fee to get better quality care at an NGO.
V. Kasturi “Kash” Rangan is the Malcolm P. McNair Professor of Marketing at the
Harvard Business School. Until recently the chairman of
the Marketing
Department (1998-2002), he is now the co-chairman of the school’s Social
Enterprise Initiative.
R. D. Thulasiraj is Executive Director of the Lions Aravind Institute of Community
Ophthalmology (LAICO). Mr Thulasiraj is also the Chairman of International
Agency for Prevention of Blindness-South East Asia Region (IAPB-SEAR). Herr.
Thulasiraj received a MBA in Management from Indian Institute of Management,
Kolkata(Calcutta).
A case narrative describing Aurolab, a subsidiary of Aravind, was published in volume
1, number 3, of Innovations with the title “Making Sight Affordable (Teil I).”
The Schwab Foundation for Social Entrepreneurship has recognized R.D. Thulasiraj
and the late Dr. Govindappa Venkataswamy as Outstanding Social Entrepreneurs.
© 2007 V. Kasturi Rangan and R.D. Thulasiraj
Innovationen / fallen 2007
35
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023
V. Kasturi Rangan and R.D. Thulasiraj
Some government eye hospitals have reputations for offering good service, Aber
overall the poor consumers prefer private or voluntary eye hospitals because the
services are more reliable and overall outcomes better.2 The country’s capacity to
perform cataract surgeries has surged from about 1.2 million a year in 1991-92 Zu
nearly 5 million a year by 2006, much of it coming from the catalyzing efforts of
pioneering organizations such as the Aravind Eye Hospital. Von 2006, grob 25%
of the work was done in the government sector, 40% by the NGOs, Und 35% von
private clinics.
There are many examples of excellent public health delivery models around
die Welt, but rarely do we see one that has been able to grow steadily over three
decades, and yet simultaneously maintain, even increase, the excellent quality of its
service. Aravind is an exemplar in this regard. Even more interestingly, it is fueled
by a self-funding model: grob 40% of its patients, those “paying” for its servic-
es, provide the profit margins to deliver a high-quality service for the rest of the
60%, “non-paying” poor patients.
This paper attempts to dissect what we have learned from Aravind’s success for
the benefit of healthcare professionals managing other similar public health sys-
Systeme.
The first author, Kash Rangan, started his work with Aravind almost 15 Jahre
ago with the development of the first business case study of its workings. The sec-
ond author, Thulasiraj, the nephew of Aravind’s founder, has been a part of the
hospital group’s senior leadership team from the time of its founding.
THE FOUNDING OF ARAVIND
In 1976, a retired ophthalmologist, DR. G. Venkataswamy (better known as Dr. V.),
Dann 58 Jahre alt, founded the Aravind Eye Hospital in Madurai (a bustling town
von 3.5 million people in the southern state of Tamil Nadu) to address his mission
of eradicating “needless” blindness in India and indeed all over the world. Beginnend
mit 11 beds in the living room of his home, he recruited his extended family to
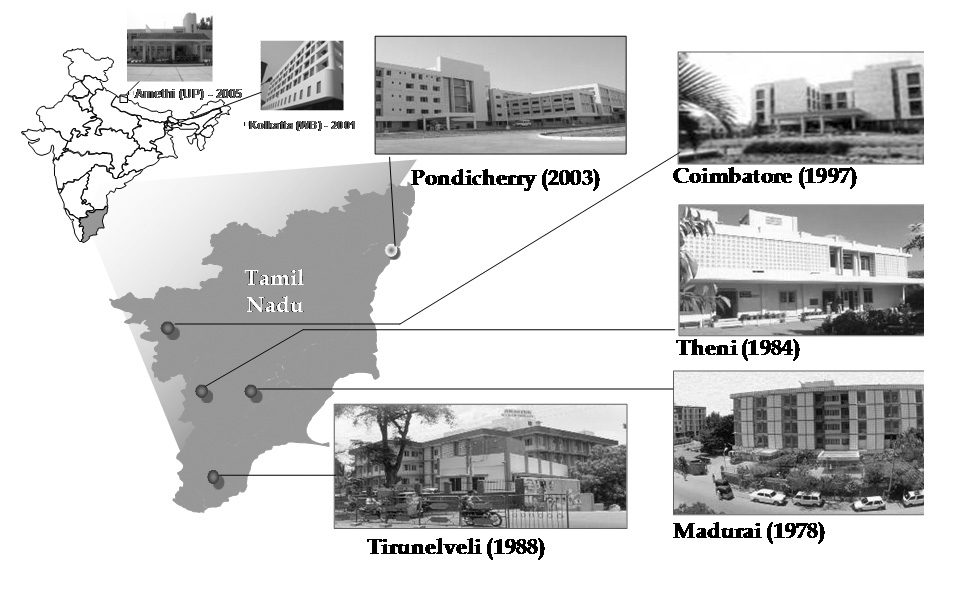
join in his mission. Heute, mit 3,500 beds in five hospitals, it is one of the largest
eye care systems in the world. Figur 1 shows Aravind Eye Hospital locations in
Indien. In the most recent fiscal year (2006-2007), Aravind screened 2.3 million out-
patients and performed 270,000 surgeries. Over the last 30 years since its found-
ing, Aravind has screened 22.37 million outpatients and performed 2.8 Million
surgeries.
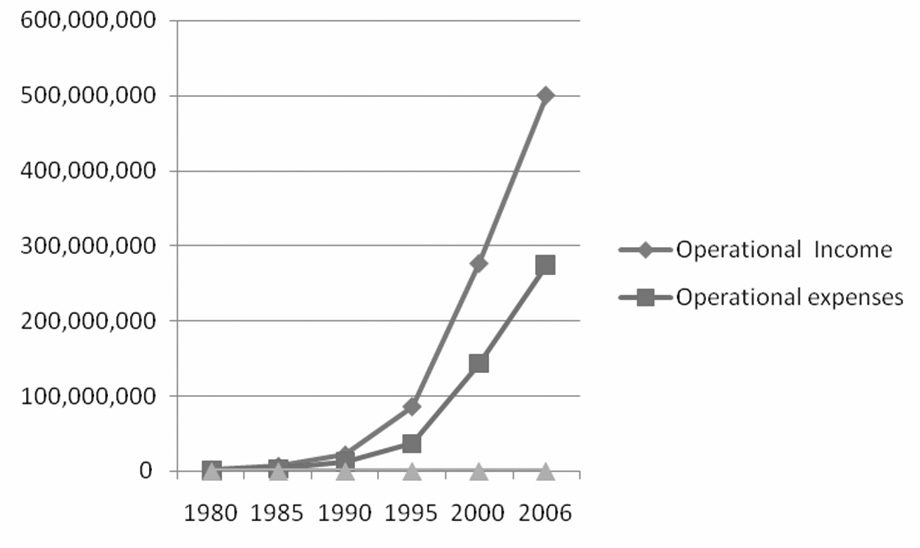
One of the truly astounding aspects of this high-performance model has been
the self-sustaining fiscal engine that has driven Aravind’s impressive growth.
Figur 2 shows how its revenues and expenses have evolved since its founding in
1976. Because Aravind was set up as a charitable trust (d.h., as a nonprofit) the sur-
plus has been constantly fed back into the system for improvements and expan-
sion.
36
Innovationen / fallen 2007
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023
Making Sight Affordable
Figur 1. Aravind Eye Hospital Locations
SUCCESS DRIVEN BY VISIONARY LEADERSHIP
AND FIVE KEY STRATEGIC CHOICES
DR. V. died in July 2006, but for most of the 30 years since the hospital’s founding,
he was undoubtedly the system’s visionary and architect. It may be tempting for
writers, especially those who have personally interacted with Dr. V. and experi-
enced the breadth of his vision, his boundless energy, and his enormous will
power, to ascribe Aravind’s success primarily to his leadership qualities. But many
other significant forces also influenced Aravind’s success, including the contribu-
tions of several key family members who were important members of the group’s
core leadership team.3 Moreover, DR. V. was acutely aware of the importance of
management systems as a way to scale the model. He also knew that Aravind had
to be molded into a learning organization, so that it could grow rapidly to achieve
its audacious ambitions. Above all, he knew that if the organization was to succeed,
it needed a leadership team to assume responsibility for its growth.
The success of Dr. V. and Aravind lay in their masterfully constructing—over
many years—a health care system in which many components were strategically
designed and brought together. Underlying the development of that system were
numerous innovations and strategic choices. Some are based on hard-nosed eco-
nomic reasoning and others have to do with the development of management
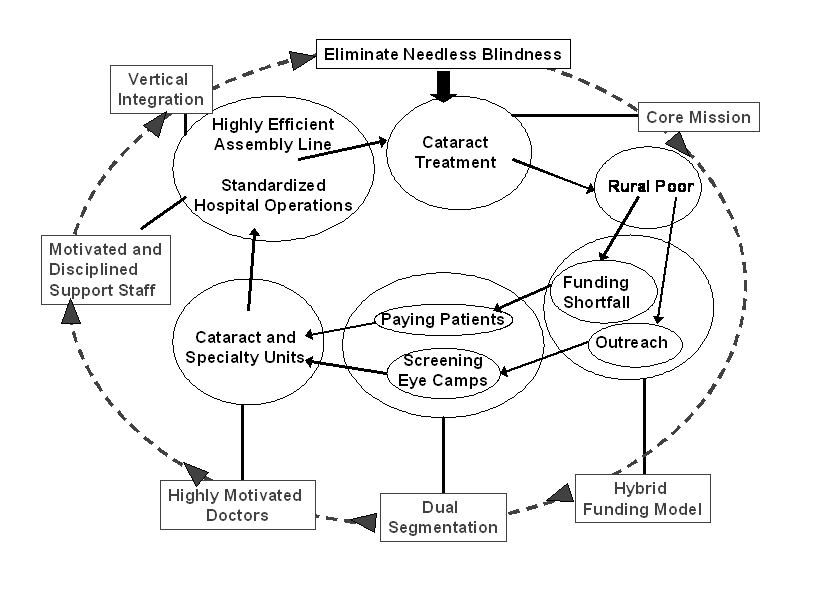
processes that consistently align the organization with its mission. Every one of
those elements is tightly interwoven into a virtuous cycle of performance, reinforc-
ing and amplifying their individual contributions. Five key strategic choices are
particularly notable.
Innovationen / fallen 2007
37
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023
V. Kasturi Rangan and R.D. Thulasiraj
Learning-by-Doing
Throughout its first three decades, Aravind’s strategy was very much shaped by
an experimentation model: key ideas floated by any member of the leadership
team would be tried out, though not always with a fully fleshed out implemen-
tation plan. Early results would then be analyzed and a revised strategy readied,
and the process repeated till tangible results emerged.
The hybrid funding model itself was the result of such a strategy molding
Verfahren. During the early years, 1976-78, DR. V. was not very successful in rais-
ing money to support his vision of providing free care for those who would not
be able to afford the fee, so he took a detour and arranged to build the ground
floor of the “fee-for-service” hospital. But even then the senior management
team had the vision to lay the foundation so that the facility could be expanded
upwards. From the surplus of the ground floor operation, the first floor was
built, und so weiter, till the five-story main hospital was readied. The free hospital
was built following the completion of the main hospital using the cash flow gen-
erated from earned revenues.
After it had served paying customers in its first few years, as a strategic
necessity, Aravind learned the many advantages of the paying customer beyond
merely providing funding sustenance; thus the hybrid strategy of combining
specialty clinics with cataract treatment began to gel. This then led Aravind to
structure a unique, cutting-edge clinical practice environment as a way to
attract and retain highly qualified doctors.
The same spirit of learning by doing has also pervaded many of Aravind’s
other strategic forays. When Aravind formulated its early strategy on eye camps,
the “yield” was below 20%. Das ist, less than one in five potential patients actu-
ally availed of the offer of free surgery. Through a process of client research its
field personnel discovered the many barriers that poor rural people faced in
making the choice to have the surgery. It added services—food, lodging, Und
transportation—to address exactly those constraints. Today the acceptance rates
are over 90%. Through a similar process of trial and error the yield at refractive
camps (those where eye glasses are prescribed and fitted) have surged from less
als 10% In 2000 to over 80% In 2006. Aravind now takes with it a selection of
frames and lenses, including the equipment to make adjustments and fittings to
deliver the prescriptions on the spot. A small amount of custom glasses alone
are mailed to the patient from a central facility.
But trial and error also means that unsuccessful experiments must be termi-
nated. In den 1980er Jahren, to make it convenient for rural people to accept the surgery,
Aravind engaged in several surgical camps on-site. Das ist, the outreach organ-
ization would temporarily convert a facility, such as a school building, into a
surgical facility, and Aravind doctors and support staff would do the surgery.
Soon Aravind realized that the medical outcomes were hard to manage because
of the variable quality of the surgical environment. So Aravind abandoned the
surgical camp model and converted to a screening camp only model.
38
Innovationen / fallen 2007
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023
Figur 2. Income and Expenditure
Notiz: The dollar to rupee exchange rate varied over the time period. It was about
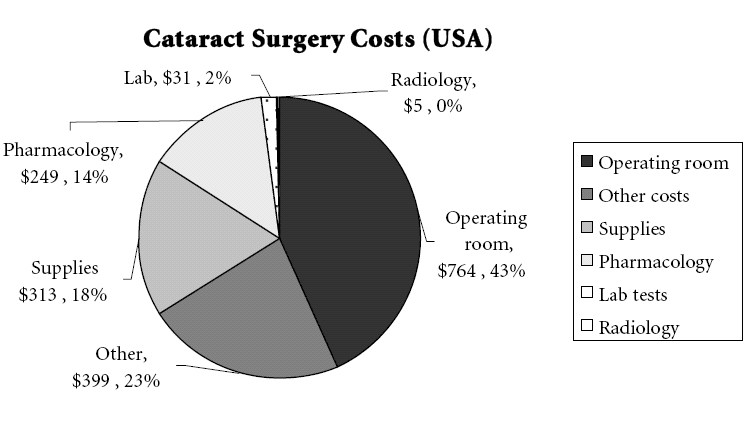
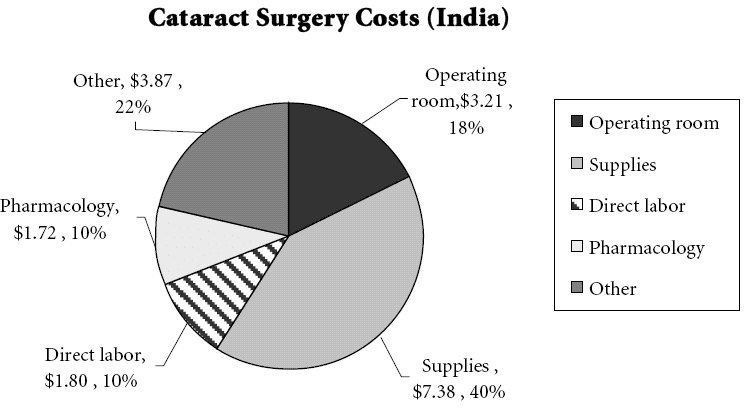
Rs 12 = $1 In 1980, about Rs 25 = $1 In 1993, and Rs 45 = $1 In 2006. The first strategic choice key to Aravind’s success has been the organization’s unstinting focus on the elimination of cataract blindness. In founding Aravind, DR. V. could have gone in many directions to eliminate blindness. He chose cataract blindness. That first singular choice was the most important in Aravind’s develop- ment, and the rest of its later strategy was predicated on it. The organization’s second key strategic choice—to pursue a “hybrid” business model—was initially driven by necessity. While Aravind’s mission from the outset was to serve the under-served, particularly the rural poor, DR. V.and his early core management team (his brother, Herr. G. Srinivasan; his sister, DR. Natchiar and her husband, DR. Namperumalsamy; and Dr. Nam’s sister, DR. Vijayalaksmi and her husband Dr. M. Srinivasan) recognized that in order to achieve this mission they needed funding. Lacking other options, they decided to raise revenue by building a clientele of paying customers seeking specialized services. They soon recognized that their improvised, hybrid business model had many advantages over the alter- native of offering only one level of service to patients unable to pay; earning rev- enue to cross-subsidize their core mission was only one of the many benefits. (See the text box above titled “Learning by Doing.”) The core motivation behind the hybrid operating model was the ambition to reach a scale of operations that matched the scale of the challenge. Surprising as it may seem, during those early days, one of Dr. V’s main obsessions was to study the principles that enabled retail systems, such as McDonald’s and Sears, to attain scale. Given India’s population demographics and disease incidence, if Aravind was truly to have an impact, it had to design a system to take care of the millions of rural poor who were cataract blind. That led Aravind to adopt and refine the chan- Innovationen / fallen 2007 39 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 V. Kasturi Rangan and R.D. Thulasiraj nel of “screening camps” as a way of reaching out to the rural poor, as described further below. Having put in place a strategy for gaining volume, the next big challenge lay in building the capacity to take care of the massive volume of cataract surgery that was being targeted. This led to Aravind’s third key strategic choice: to design an operational system that would be low-cost, without compromising on the quality of care. The design of an “assembly” line system was a direct outcome of this effort. Clearly a low-cost assembly line system would produce quality outputs at affordable cost only if the components going into the assembly were high quality at low cost. This logic led Aravind to its fourth key strategic choice: vertical integration of key production inputs. [D]uring those early days, one of Dr. V’s main obsessions was to study the principles that enabled retail systems, such as McDonald’s and Sears, to attain scale… [ICH]f Aravind was truly to have an impact, it had to design a system to take care of the millions of rural poor who were cataract blind. Ultimately none of these systems would have had stay- ing power without the fifth key choice: to have doctors and support staff work together as the human engine to design and run such a system. The healthcare delivery model needed to be supportive of the highly disciplined and motivated work force. This was the behind-the-scene crucial fuel that provided the energy to sustain the other four key elements of strategy. Every one of these strategic elements that we have briefly alluded to was critical to Aravind’s success, as Figure 3 indicates. If even one element failed, the entire system could unravel, but if they all clicked the synergy would be exponential. We attempt to explain each of these factors in more detail in the following paragraphs.4 1. A Predominant Focus on Cataract Treatment In practice, Aravind is a multi-faceted research and clinical institution with many centers of excellence in ophthalmic specialties, such as Retina and Vitreous Surgery, and Laser Procedures, but in principle it remains a large scale “focused factory,” emphasizing cataract surgery. A little over two-thirds of all Aravind sur- geries are for cataract removal, for good reason: cataracts are by far the leading cause of blindness in India, and therefore the quickest route to making a dent on the blindness problem. So even though Dr. V.’s ambition called for the organiza- tion to take on the elimination of blindness as its overarching “big mission," In 40 Innovationen / fallen 2007 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 Figur 3. Virtuous Cycle of Performance at Aravind reality the organization focused on cataract treatment. Nor did the organization get deflected in making “prevention” a significant piece of its programming. Because of Aravind’s wide reach into rural communities, it may seem well suited to carry out the critical functions of education and information dissemination, but those in its target audience come to its camps much later in the cycle after they have incurred the affliction, rather than before. Every year, Aravind conducts sev- eral studies, as part of its public health research program, that investigate the caus- es of blindness, including nutrition, Lebensstil, Kultur, and customs, but once again these activities are not a significant part of its core programs, which are focused on cataract treatment. In 2000, recognizing that its outreach program could benefit the huge numbers of those who would need prescription glasses, Aravind started a Refraction Camp service. In 2006 allein, between the 124 refraction camps and 1,442 regular camps, Aravind screened nearly 440,000 people and fitted about 68,000 with prescription glasses. More recently Aravind has moved into the treatment of another eye ailment, diabetic retinopathy, welche, like cataract, is widespread in India. As the name indi- cates, some diabetic patients will develop a condition in the retina that leads to the bleeding of blood vessels. Unless treated with laser procedures in a timely fashion, the ailment can result in permanent loss of eyesight. In India, the World Health Organization (WHO) estimates that currently 3.2% of the general population, or about 32 million people, have diabetes. Roughly 20% of them would have devel- oped diabetic retinopathy and among these, 20% would require active treatment such as a laser procedure. The WHO also estimates that in the next 25 years the innovations / fallen 2007 41 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 V. Kasturi Rangan and R.D. Thulasiraj prevalence of diabetes in India will increase to 5.6% of the projected population of 1.4 Milliarde, or about 80 million persons.5 In the 2006-2007 fiscal year, über 70,000 outpatients were screened for this ailment (through mobile screening camps and patient visits to one of Aravind hospitals), and nearly 3,500 were identified as needing treatment. This kind of laser-like engagement is valuable, especially in the delivery of pub- lic health. Causes of illnesses are complex, and often one cannot undertake treat- ment without engaging in prevention. But it may not be possible for any one enti- ty to cover the full span from prevention to treatment. Many different institutions and organizations will all have to work in a coordinated fashion to cover the entire spectrum. Aravind’s focus was “cataract surgery.” In essence, even when Aravind extended itself through refraction or diabetic retinopathy outreach camps, it stayed very faithful to its strategy model. Patients identified as needing further treatment at either of these camps were provided a definitive solution within hours when fitting glasses or within days in the case of diabetic retinopathy. 2. Client Segmentation and Quality Assurance The core mission of the hospital and the primary purpose of its founding was to address the needs of the vast numbers of poor, who live mainly in rural areas. Recognizing that surgical centers in urban centers would not be able to attract the vast masses of the rural poor (about two-thirds of India’s poor), DR. V. pioneered the massive use of eye screening camps to reach out to the rural poor and bring into the base hospital those selected for surgery. Instead of waiting for those in need to come to its door, Aravind conducts eye camps in rural areas to find patients. Medical teams work closely with community leaders and service groups to set up camps that screen hundreds of people in a single day. Free screening camps are held every day, and while Aravind provides the staff and the medical equipment, community partners like the Lion’s Club, charitable organizations, or local philanthropists publicize and organize the camp and provide food and bus- ing for those selected for surgery. The same afternoon or evening of the camp, those selected for surgery are then transported by buses to a base hospital for sur- gery the following day. (Aravind recognized the value of partnerships with local communities and philanthropic organizations to gain scale, especially in reaching out to poor patients in far-flung villages.) In the most recent year, 2006-07, Aravind offered 2,049 outreach screening eye camps. Of the 270,000 surgeries performed, über 110,000 were admitted through these outreach activities and received free surgeries. These admissions and anoth- er 35,000 walk-in patients to the “free section” in the base hospitals accounted for about 60% of all surgeries performed.6 Paying patients made up approximately 40% of the total pool. These are patients who walk into one of the five hospitals seeking the high-quality services they would seek in a private clinic. Such customers are provided a differentiated service in both the outpatient and inpatient clinics. A dedicated part of the hospi- tal is devoted to their care and recovery. The paying segment is crucial to Aravind’s 42 Innovationen / fallen 2007 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 Making Sight Affordable strategy for two reasons. Erste, patients pay market prices for their eye care because Aravind is the quality leader in its field, and the income generated subsidizes the organization’s core mission. Zweite, paying customers set high demands on qual- ity care (at least higher than non-paying customers), and those standards are used as a benchmark for nonpaying customers. Because the paying patients are so central to its funding model, Aravind pro- vides them a differentiated service: beds (as opposed to floor mats), optional air conditioning and semi-private bathrooms. But in spite of such differences in the pre- and post-operative services, the same team of surgeons provides the surgery. Doctors rotate between the “free” and “paying” hospitals on a set schedule, so that whether senior or junior, every doctor treats patients at eye camps and in surgical procedures. Because Aravind’s paying patients subsidize its nonpaying patients, it avoids some of the critical problems of funding sustainability that other nonprofits and NGOs face on this front. But Aravind’s paying patients play an important quality assurance role, and an even more crucial professional development role. Without the earned-income pool of paying patients, market feedback would be muted. If that occurred, the discipline needed to maintain high-quality stan- dards would diminish, and so would the treatment of poor patients. Partly to address the market needs of this funding segment, Aravind offers a comprehensive variety of non-cataract specialty clinics. Retinal detachment corrections, vitreous surgery, laser procedures, and other special treatments make up nearly 25% of Aravind’s services. Aravind’s doctors are challenged to master new skills for these specialist disciplines, which helps them remain committed to Aravind. Without such intangible benefits, doctors could well be tempted by the higher salaries at private clinics. Many surgeons might not consider cataract surgery, allein, to be professionally challenging and rewarding, even if it provided the spiritual satisfac- tion of serving the poor and needy. 3. A Laser-Like Focus on Operational Efficiency and Cost Control During the 1970s and 1980s, India had only about 12,000 ophthalmologists, which severely handicapped its capacity to treat its blind. It was this “production” bottle- neck that Dr. V. addressed by his innovative “assembly” line system for surgery. Patients were readied for surgery in groups, with qualified ophthalmic assistants doing almost all the preparatory work including the anaesthetizing, so that sur- geons could focus on the surgery itself. When the procedure is completed, appro- priate supplies are quickly refurbished as the next patient is brought in and the treated patient is escorted to the recovery room. Each operating room, except those used for complicated surgeries such as retinal detachment, usually had two or three operating tables as a way of efficiently utilizing the OT supporting staff. At each operating table, there were multiple sets of instruments and support staff to ensure that the waiting time between surgeries was almost zero. The same principle is also applied in the outpatient examinations: trained support staff carry out all the rou- tine diagnostic procedures, some of which tend to be quite time consuming. The innovations / fallen 2007 43 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 V. Kasturi Rangan and R.D. Thulasiraj Figure 4. Comparison of Costs (UNS. and India) Sources: Naeim A. 2002. Healthcare Cost-Effectiveness Analysis for Older Patients: Using Cataract Surgery and Breast Cancer Treatment Data. RAND publication RGSD-168 [top]. Aurolab. 2004 [bottom]. Reproduced from “Making Sight Affordable (Part I): Aurolab Pioneers Production of Low-Cost Technology for Cataract Surgery,” by Mahad Ibrahim, Aman Bhandari, Jaspal S. Sandhu, and P. Balakrishnan, Innovations 1:3 (Sommer, 2006), S. 25-41. ophthalmologists perform only those tasks, such as surgery or diagnosis, which require good clinical judgment based on their medical knowledge. This process not only enhances the utilization but also improves the quality. Both of these in turn reduce the cost of care. 44 Innovationen / fallen 2007 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 Making Sight Affordable Aravind’s process of readying the patient for surgery, performing the surgery, and getting the patient through recovery is all configured like a modern assembly line. So while the average ophthalmologist in India performs about 400 cataract surgeries a year, an Aravind doctor performs about 2,000: an efficiency factor of about 5. Much of the efficiency can be attributed to the superbly constructed assembly-line process, even though the Aravind surgeons, because of their training and long work hours, perform more surgeries compared to their Indian counter- Teile. The factors behind this level of efficiency can be broadly grouped into the following categories, listed in the order of importance: • steady flow of patients—keeping patient supply line busy; • surgical flow, which ensures minimal waiting time between surgeries; • well-trained surgical assistants and adequate staffing; • detailed logistics planning ensuring zero downtime for want of supplies or equipment; • daily micro-planning to match the surgical load to staffing and supply require- gen; and • surgeons’ skill and stamina. As a result of all these factors, von 2006, Aravind’s cost of providing cataract sur- gery was about $18 per person—including the intra-ocular lens (IOL). In compar-
ison, the cost of surgery in the U.S. is about $1,800 and the lens alone could cost as much as $150. Studies of patient outcomes have shown that the quality of care at
Aravind is comparable to that in top hospitals, not only in India, but in the U.S.
and other developed countries as well. Siehe Abbildung 4.
4. Vertical Integration
As shown in Figure 4, two important cost elements are personnel and the critical
components in the surgery: in diesem Fall, first the salaries and wages of the doctors
and nurses and second, high-tech essentials like the IOL. An essential part of the
Aravind model is to leverage the doctor’s time by providing him/her the support
of highly efficient and trained ophthalmic assistants (nurses). But doing that
required hiring and training large numbers of assistants and retaining them. Solch
a large pool of talent was not easily available, so Aravind chose to create its own
supply. Ähnlich, later in its growth phase, as surgical techniques and technologies
evolved, Aravind was caught in a huge quality gap between the paying and the
poor, because it lacked an essential component in the surgery for the poor: Die
intra-ocular lens. Again Aravind chose to innovate boldly in order to fulfill its mis-
sion. We briefly discuss those two initiatives as illustrations of its operational excel-
lence.
Nursing Staff: The clinical ophthalmic assistants, often referred to as nurses,
continue to be the backbone of Aravind’s clinical operations. Each year over 300
young women, gealtert 18 Zu 23, from nearby villages are selected to undergo two
years of training at Aravind before they are hired there full-time. Since the hospi-
tal is spread across 5 Standorte, the recruitment pool comes from the service area
of these hospitals. Most of these young women have barely passed high school, Und
Innovationen / fallen 2007
45
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023
V. Kasturi Rangan and R.D. Thulasiraj
under normal circumstances would not have found any meaningful employment
in the village. Going to the nearby city to look for a job is a viable option but not
entirely accepted due to cultural and social norms of most village dwellers, partly
because of the real or anticipated fears of working in a large city, especially for
unaccompanied young women. Aravind steps in to hire, and the training is given
free and the women also receive free housing and a stipend.
During the training, the emphasis is placed equally on developing skills in
ophthalmic techniques and also learning how to deliver those skills in a compas-
sionate, patient-centric way. After the first six months of common training, jede
person is channeled to develop her skills in a specific area such as outpatient serv-
ices, Wächter, operating room, refraction, patient counseling, housekeeping or med-
ical records. Once they successfully complete training (über 98% do so), they are
all absorbed into the Aravind system. Many families see Aravind’s structured train-
ing program and supervised living accommodation at the nurses’ hostel as the ulti-
mate solution to gaining employment, vocational training, and income in a safe
Umfeld. After training, most such qualified women spend several years serv-
ing at Aravind, picking up confidence, skills and money. Their loyalty to the insti-
tution is demonstrated by the relatively low turnover: nur 10% annually. Most go
back to their families after three to five years of service at Aravind to marry and
settle down.
IOL manufacture: In the early 1990s, the preferred surgical technique for pay-
ing patients and in private clinics in India was ECCE (extra-capsular surgery with
intra-ocular lens). This surgery was inevitably performed with an operating
microscope: the surgeon left the posterior capsule intact and then inserted the IOL.
The outcome for patients was far superior, but Aravind was handicapped by a lack
of resources (operating microscopes, training for surgeons and the availability of
cheap IOLs). But Dr. V., in his drive to provide quality care for the poor, drove an
ambitious vertical integration program.
The primary hurdle to IOL adoption in India at that time was price. IOLs sold
for nearly $150 apiece in the U.S. and Western Europe, making IOL manufactur- ing among the most profitable segments of medical device manufacturing. In the early 1980s, strong profits in North America and Europe enabled American IOL manufacturers to donate some lenses to Aravind and other charitable eye hospi- tals. As Aravind’s surgical volumes grew, Jedoch, the donor organizations could hardly keep up. Only paying patients were offered the IOL option at a fee. Although IOL prices were coming down, Aravind and its patients, especially the poor, could not afford to buy the implants in the open market. Darüber hinaus, as the IOL implant became available, patients in their 40s and 50s came in for surgery, having heard that they could regain their vision fully and could go back to their livelihoods. DR. V. and his colleagues looked for a way out. IOL manufacturing was consid- ered extremely high-tech at that time. It required the latest in precision machining, sterile techniques, and quality control. While a few Indian companies were special- izing in ophthalmic products, even fewer had yet ventured into IOLs.7 In 1992, 46 Innovationen / fallen 2007 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 Making Sight Affordable based on the need for affordable IOLs, Aravind, with help from external support- ers (David Green from Seva Foundation in the U.S.), began a process of technolo- gy acquisition that resulted in setting up Aurloab, an internal manufacturing capacity under the auspices of an independent charitable trust. Heute, that facility produces more than enough quality lenses at an affordable cost to meet all its needs It sells the excess to other hospitals and NGOs in India, and the margins go to further support its core mission.8 5. Hardwiring the Spirit for Service Over the years, as we pointed out earlier, Aravind has constantly reinvested its operating surplus to acquire the latest technology and equipment, even while being very innovative in keeping costs to the efficient minimum. But in a highly service-oriented business such as eye care, especially when the majority of cus- tomers are from the poorer segments of society, what keeps the system humming is the people: the vast cadres of doctors and nursing staff that make the strategy happen. Von 2006, the Aravind system had nearly 125 ophthalmologists, 615 clini- cal nursing staff, 480 people supporting other functions, 70 individuals directly involved in outreach activities, Und 130 people in administration, totaling over 1,400 people engaged in the mission. It is a family business, but only about 35 of Dr. V.’s family members are part of the operation. How can such a huge system run on the philosophy of its founder and core management team, when it calls for extraordinary attention to efficiency and dedication to service quality? The answer is that throughout the system Aravind has inbuilt institutional mechanisms to motivate its human resources. Zum Beispiel, its doctors are encour- aged and supported in research activities, which can involve training in cutting- edge techniques. Given its size and reputation, Aravind has been able to attract doctors from leading academic institutions around the world to visit and spend some time training its doctors and doing research. The same is true for technolo- gies from leading equipment suppliers. Aravind is often the lead user for advanced technologies or treatments. All of this, along with the satisfaction of providing people the gift of being able to see again, is the source of its doctors’ motivation. The nursing staff, zu, as we pointed out earlier, is treated with care and attention to their own development. In a service business the welfare of the service provider is the key antecedent to the welfare of the client, and at Aravind this principle is thoroughly institutionalized. GOING TO SCALE It is important to recognize that Aravind’s strategy model was shaped by trial and error; it was a classic case of learning by doing. As a consequence, the core man- agement team was in complete harmony with its direction, with Dr. V. being the chief architect and keeper of its mission. But even as the strategy was being joint- ly sculpted, each key member took on primary responsibility for an aspect of the strategy and its implementation. Zum Beispiel, DR. Natchiar oversaw the clinical innovations / fallen 2007 47 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 V. Kasturi Rangan and R.D. Thulasiraj and service side of the operations, including the crucial task of recruiting and training the nursing staff. DR. Namperumalsamy oversaw the clinical specialties and advanced training for doctors, along with the connections to leading research and innovations in the field. As the group’s current chairman, he has been invest- ing in its research capabilities. Herr. G. Srinivasan provided the oversight for the expansion and maintenance of physical plant. DR. Vijayalakshmi and her husband M. Srinivasan provided the leadership with respect to cataract surgery and its advances. Thulasiraj provided the leadership in organizing outreach activities, and later for training outside providers who wished to learn from Aravind. Others, zu, were handpicked by Dr. V. for special tasks. Zum Beispiel, Balakrishnan, with a Ph.D in engineering, was attracted from his U.S. job to take over the leadership of Aurolab, the manufacturing arm. As new hospitals were added, a second-genera- tion leadership team from Madurai was transferred to the new location to get it launched. Because of their significant experience with the operating procedures and principles at Madurai, the translation was usually smooth. Interessant, most discussions of strategy were informal within the core leadership group, and often took place outside the work environment. There was a tacit understanding of, and empathy for, each other’s perspective, so much so that strategy formulation was a group affair. There was harmony and coherence at the top. A key requirement for scaling is standardizing core activities. The nature of the screening activity at eye camps, or for that matter the surgical procedures for cataracts, are highly amenable to such value-engineering techniques. But that alone would not ensure a smooth scaling of the system. The surrounding activities that comprise the end-to-end system have to be standardized as well. Here is where Aravind has been innovative in its design of its healthcare delivery model. It is all boiled down into a routine: Erste, through word of mouth, and then through the discipline of formal analysis and written documentation, every activity is orches- trated, starting with how the eye camp is promoted, how the patients are brought in, and how the logistics is organized, all the way to how the medical screening occurs, and how patients are selected and readied for the trip to the main hospital. The same applies to the actual surgical procedure, and the pre- und posten- surgical processes at the main hospital. LAICO (Lion’s Aravind Institute for Community Ophthalmology) came into existence in 1992, essentially to promote best practices in the running of an eye hospital. Internally, with ambitious plans to expand to other major sites like Coimbatore, the senior management felt the need to formalize the lessons it had learned. Even then, those in the center realized that much of the hospital’s cost leverage came from its systems perspective, not just the routinization and stan- dardization of its treatment protocol. And the knowledge gained could not only readily be applied to Aravind, but perhaps could be transferred to other like-mind- ed institutions as well. Over the last 15 years this direction has translated into a number of structured training programs, consulting and capacity building activi- Krawatten, research and publications. LAICO has been in the forefront in promoting best practices, especially in the area of management. Its most significant work and con- 48 Innovationen / fallen 2007 Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023 Making Sight Affordable tribution has been in the area of capacity building in other eye hospitals. This came out of the realization that most eye hospitals in the voluntary and the government sector were under-performing when benchmarked against their own capacity and the unmet eye-care needs in their own service area. LAICO has worked with over 225 eye hospitals to enhance their capacity, essentially in cataract services. While most of these hospitals are in India, um 40 are in other countries, including Tanzania, Sri Lanka, Nepal, China, Indonesien, Bolivia, and Sub-Saharan African nations. Studies have shown that on an average, the participant hospital’s produc- tivity has jumped by 50% on most factors a year after the appropriate lessons have been implemented in each of these hospitals. In 2006, not satisfied with its reach and expansion, Aravind set a goal of per- forming one million surgeries a year by the year 2015. The senior leadership group has put together a strategy to achieve this through the concept of “Managed Hospitals,” which involves staffing and managing the day-to-day operations of an eye hospital that is not owned by Aravind. In this partnership model, the partner manages the investments and creates an enabling interface for the hospital’s effec- tive functioning. A core team from Aravind Eye Hospital would manage the staffing through local recruitment, selection and training at Aravind Eye Hospital. The hospital would be run as if it were an integral part of Aravind’s own network of hospitals. In the pilot phase, three hospitals in India (at Kolkata in West Bengal, Amethi in Uttar Pradesh, and Amreli in Gujarat) are functioning in this mode. The next great “learning-by-doing” experiment has thus been launched. If successful, an exemplar system will achieve another level of scale, with millions more cured of blindness. 1 Krisnan, Pavithra. Infinite Vision. Aravind Eye Care System; Br J Ophthalmol. 1990; 74 (6):341-3. 2. The Lancet (cid:127) Bd 355 (cid:127) Januar 15, 2000: 180-4 3. DR. V’s sister, DR. Natchiar; her husband, DR. Namperumalsamy (Nam), now the hospital group’s chairman; DR. V’s brother, Herr. G. Srinivasan; DR. Nam’s sister Dr. Vijayalkshmi; and her husband Dr. M. Srinivasan, along with Dr. V’s nephew, R.D. Thulasiraj, have all played important roles in building the institution. The second- generation team is now very active in the development and implementation of its strategies; among them are Dr. Aravind, DR. Prajna, DR. Kim and his wife Dr. Usha, DR. Kalpana, DR. Ravindran, DR. Balakrishnan, and R.D. Sriram. 4. For a more conceptual explication of the Aravind strategy model, also see V.K. Rangan, “Lofty Missions, Down-to-Earth Plans.” Harvard Business Review 82, NEIN. 3 (Marsch 2004). 5. Quelle: Global Prevalence of Diabetes—Estimates for the Year 2000 and Projections for 2030; Sarah Wild, MB, BCHIR, Ph.D, Gojka Roglic, MD, et. al; Diabetes Care, Bd. 27, NEIN. 5, Mai 5, 2004: http://www.who.int/diabetes/facts/en/diabcare0504.pdf 6. Roughly a third of the 60% “free” patients paid a small amount, equivalent to $10, and the rest
paid nothing.
7. Ebenda.
8. For more on Aurolab, Mahad Ibrahim, Aman Bhandari, Jaspal S. Sandhu, and P. Balakrishnan,
“Making Sight Affordable (Part I): Aurolab Pioneers Production of Low-Cost Technology for
Cataract Surgery,”Innovations 1:3 (Sommer, 2006), S. 25-41.
Innovationen / fallen 2007
49
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/2/4/35/704211/itgg.2007.2.4.35.pdf by guest on 08 September 2023