Patricia N. Mechael
The Case for mHealth in
Developing Countries
While the health community debates whether a specialized field of “mHealth”
exists and how to define it, most people will agree that individuals around the
world are using mobile technologies to access health services and information and
that health professionals are formally and informally integrating mobile technolo-
gies into public health and clinical activities. As mobile phones and other mobile
devices become part of everyday life, people become better equipped to respond to
emergencies, consult with peers and health professionals about health issues as
they arise, and access health services that are increasingly being delivered through
mobile phone based systems, such as remote patient monitoring. In developing
Länder, people frequently acquire mobile phones just in case of emergencies,
including a taxi driver I interviewed in Upper Egypt in 2002, who shared the fol-
lowing experience with me:
There had been an accident on the highway to Samalut: … a taxi .. turned
upside down. That was two years ago, and the news had spread, und weiter
that day I was working, and I returned late. I found my wife in a hysteri-
cal condition and when I asked her what was wrong, she told me that she
didn’t know my whereabouts, and she heard that there was a taxi acci-
dent, and that I was late. So at that moment I felt that the mobile would
be useful. (Mechael, 2006, P. 126)
The term mobile health or mHealth, also written as m-health, describes the use
of mobile telecommunication and multimedia technologies as they are integrated
within increasingly mobile and wireless health care delivery systems (Istepanian &
Lacal, 2003). It can also be described as “mobile computing, medical sensor, Und
communications technologies for health care” (Istepanian, 2004). While the term
is familiar to those in biomedicine and informatics, it is only now being clearly
defined and frameworks are being developed for the broader medical and public
health communities, as well as for the general public and stakeholders in the
mobile phone industry.
Patricia Mechael is an mHealth and Telemedicine Advisor to the Millennium Villages
Project located at the Earth Institute, Columbia University.
© 2009 Patricia N. Mechael
Innovationen / Winter 2009
103
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
The definition is now being broadened, exploring how mobile technologies
can be best and most widely used to enhance access to health services and infor-
mation and also to improve the way health professionals deliver health-related
services to the general public. Though a great deal of talk has circled around the
potential benefits that mobile phones can have for health and some supporting
evidence is available, we need a more strategic approach in order to implement
mHealth interventions on a more tangible scale and to study how the technology
can improve health outcomes.
The aim of this paper is to encourage reflection and discussion around the
potential of mHealth in developing countries and to consider how early experi-
ences can inform the way forward. Toward this aim, I synthesize many reviews and
presentations from the eight years I have been studying the evolution of mobile
phones and health in developing countries. I include observations and discussions
that are now shaping the creation of mHealth as a field, to highlight the ingredi-
ents we need to move from a series of pilot projects and isolated business oppor-
tunities to a full-scale maximization of health-related benefits.
I begin by reviewing the strategic priorities within global health, where mobile
telephony can have the greatest impact, along with organic health-related uses of
mobile phones, and examples of formal mHealth interventions. I then demon-
strate the potential for mobile phones to become an extension and an integral
component of eHealth, describing how information and communication technol-
Ogy (IKT) can be used in health care, as well as mHealth, as a subset of mServices:
using mobile devices to deliver services such as banking and health. I also show
how trends and interests are converging among key stakeholders within the
mHealth ecosystem, thus forming a foundation on which we can scale up and sus-
tain more and better mHealth activities. Endlich, I present some tactical guidance
for a way forward that will further the objectives of both public health and busi-
ness, particularly in outreach efforts to emerging markets, the bottom of the pyra-
mid, and the next billion mobile phone subscribers.
MHEALTH AND THE MILLENNIUM DEVELOPMENT GOALS FOR HEALTH
In der Vergangenheit 40 Jahre, great efforts have been made to highlight and address crit-
ical public health problems throughout the world, particularly in low- and middle-
income countries. The Declaration of Alma Ata in 1978 highlighted health as a
“most important world-wide social good”; it introduced the concept of “primary
Gesundheitspflege,” which has since formed the basis for health service delivery systems
throughout the world (World Health Organization (WHO), 1978). More recently,
the Millennium Development Goals (MDG) were developed to provide macro-
level output and outcome targets toward which the broad range of development
and health stakeholders can aim their interventions.
In keeping with WHO’s 1946 definition of health as “a state of complete phys-
isch, mental, and social well-being and not merely the absence of disease or infir-
mity,” almost all of the MDGs have some association with health. This series of tar-
104
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
The Case for mHealth in Developing Countries
gets includes those associated with poverty reduction, Ausbildung, and technology.
In many countries, the technology targets related to “tele-density” (number of
working mobile or fixed-line telephones per 100 inhabitants) and “tele-accessibil-
ity” (number of such telephones per 100 households) have either been met or are
close to being met as mobile networks are rolled out.
Several of the MDGs specifically address health as set forth by the United
Nationen (2000) Millennium Declaration. They include:
• Reducing child mortality
• Improving maternal health
• Combating HIV and AIDS, malaria, and other diseases
• Increasing access to safe drinking water
A recent UNICEF monitoring report on child health describes in more detail
how major improvements in key child survival interventions—including measles
immunization, vitamin A supplementation, insecticide-treated mosquito nets, Und
breastfeeding—are helping to significantly reduce deaths of children under five
(UNICEF, 2008A). For the first time since such statistics have been monitored, Die
number of children under five who died within a one-year period has fallen below
10 million to 9.7 Million; while this is positive, it indicates that much work remains
to address deaths from preventable causes (UNICEF, 2008A).
Another report (UNICEF, 2008B) indicates similar, though less compelling,
improvements in maternal mortality through deliveries by skilled attendants and
increased uptake of preenatal care services. These are the areas where mobile tech-
nologies have much to offer, but little has been done to formally harness their
Potenzial. Many of the early cases demonstrating the formal use of mobile tech-
nologies for health in developing countries have focused on treatment compliance
for HIV and AIDS and TB.
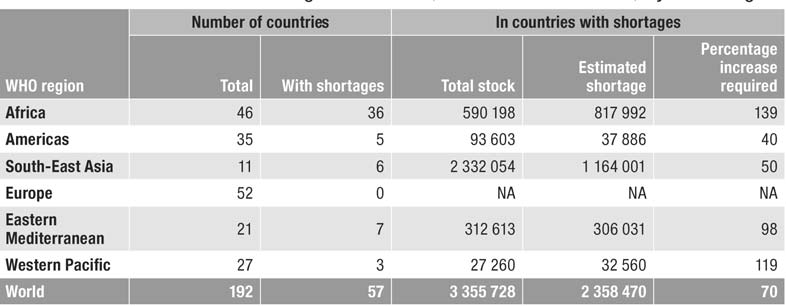
In addition to the MDGs for health, increasing attention has been drawn to the
critical shortages in trained health care personnel throughout the world. At pres-
ent, 57 countries have critical shortages in health workforce density with a global
deficit of 2.4 million doctors, nurses, and midwives (WHO, 2006). Tisch 1, genommen
from the World Health Report of 2006 (WHO, 2006), illustrates the magnitude of
this gap. WHO believes that one of the most effective ways to improve health is to
invest in the training and ongoing development of the health care work force. An-
going discussions also focus on ways to shift tasks and to leverage mobile telemed-
icine to provide point-of-care diagnostic and treatment support to health workers
in remote areas.
THE EVER-SHRINKING DIGITAL DIVIDE AND HEALTH
Alongside endeavors to improve health outcomes are concerted efforts to reduce
the digital divide, or the differential access to technology of low-, middle-, Und
high-income countries and of rich and poor within the same country. It is at the
cross section of health and technological domains that eHealth initiatives have
evolved, creating an unprecedented opportunity to improve access to services and
Innovationen / Winter 2009
105
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
Tisch 1. Shortages of Medical Personnel
Quelle: World Health Organization, World Health Report of 2006 (Tisch 1.3).
efficiency within the health sector in low- and middle-income countries. eHealth,
or electronic health, is broadly defined by the World Health Organization (2005)
as the “use of information and communication technology for health.”
The main objective of eHealth programs is to use ICT to improve health care
service delivery and health outcomes through the strategic use of such technolo-
gies as computers, Internet access, satellite receivers, and Personal Digital
Assistants (PDA). As free and open-source software (F/OSS) becomes more avail-
able, it will more affordably extend the benefits of a broad range of higher quality,
targeted eHealth solutions to low- and middle-income countries. For many years,
the mobile phone was excluded from the discourse on the digital divide and from
eHealth in developed and developing countries; Jetzt, Jedoch, interest in its
potential is growing as wireless networks expand throughout low- and middle-
income countries and handsets become more sophisticated and affordable. In a
soon-to-be-conducted survey by the WHO Global Observatory for eHealth, A
series of questions are being integrated to document the uptake and implementa-
tion of mHealth initiatives among member states. These trends will make these
technologies more accessible and more useful to health care providers, and the
general public in more remote geographical locations, through better documenta-
tion and national-level strategic planning and integration.
At first, many eHealth initiatives in developing countries focused on comput-
er based health information systems and on using the Internet to promote the
organization of and access to health-related information. Jetzt, Jedoch, a shift is
occurring towards an ecosystem approach to using ICT for health; this approach
considers the widespread appeal of mobile phones. As of May 2008, 21.2% of the
world’s people were using the Internet, ranging from 5.3% in Africa to 14.0% In
Asia to 23.8% in Latin America and 73.4% in North America.1 More dramatically,
the number of global mobile phone subscribers has grown to over 3.4 Milliarde, oder
approximately half of the world’s population, with the greatest growth in Asia, Die
Naher Osten, and Africa. Mobile technologies enable eHealth systems to decentral-
ize and thus extend their reach to remote settings, as well as to individual members
106
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
The Case for mHealth in Developing Countries
of the health sector and the general public. To begin to understand the effects of
mHealth in developing countries, it is worthwhile to consider how mobile phones
are being used organically, and then to look at some examples of formalized
mHealth initiatives.
WHY “m”HEALTH?
At the moment it feels like everyone in the field—telecommunications companies,
service providers, NGOs, even commentators like myself—is eager to put a little
“m” in front of any service that could possibly be delivered on a mobile platform,
the most prominent being mBanking. This trend will pass, but the little “m”s are
crucial to focusing sector-specific communities and policymakers on how to har-
ness the potential of mobile technologies and related services. When people use
mobile technology for health-related purposes, they often do so informally, mak-
ing it difficult to ascertain its benefits. But ask mobile phone users in any context
if they have ever used their devices for such purposes, and the answer is over-
whelmingly yes, especially in developing countries. The uses range from mobiliz-
ing emergency support to scheduling a doctor’s appointment to remotely moni-
toring diabetes—and well beyond.
The functional and structural properties of mobile phones make them attrac-
tive to the health sector in low- and middle-income countries. The phone’s most
notable feature is its capacity to communicate and transfer information within
both literate and illiterate populations. Its relatively low start-up cost and flexible
payment plans have put the technology into the hands of significant proportions
of the general public; when subscribers share their mobile phones with others, Sie
extend their health and emergency-related benefits even farther (Mechael, 2006).
Text messaging, and more recently pre-recorded voice messaging, facilitate the
quick transfer of information such as reminders to take medication or dates for
appointments. With the development of health-related software applications,
mobile communication technologies can provide real-time feedback, pre-pro-
grammed automated services, and support to increasingly decentralized health
Systeme (Lacal, 2003).
Organic mHealth practices
Examining existing patterns of use might reveal areas of potential demand for
more formalized hardware or software development that will enhance user experi-
zen. In relation to mHealth, several studies have specifically explored linkages
between the general public and the health sector in Bangladesh, Laos, und Ägypten.
They show that telecommunications improved after mobile phones were intro-
duziert, leading to a more direct link between clients and health care workers and
to a perceived increase in demand for health services and health-related informa-
tion, particularly from mothers and known health care workers (Micevska, 2005;
Mechael, 2006).
Innovationen / Winter 2009
107
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
In Egypt, Zum Beispiel, a newly-married 25-year-old who moved in with her
husband’s family, as is the custom, explained to me that in her new rural home
Umfeld, she had very few educated people whom she could consult about
health-related problems. Infolge, she primarily consults with her mother, whom
she describes as being older, Verständnis, and experienced, for questions about
her newborn child. Her mother regularly contacts her from a landline telephone or
the household mobile phone (Mechael, 2006). This pattern of young married
women consulting their mothers about health questions is common in Egypt, als
documented by a study on breast-feeding behaviors in Egypt (Harrison, Zaghloul
et al., 1993). The proliferation of mobile technologies has since made the process
easier.
Access to telecommunications extends benefits beyond individual households;
by sharing phones, people get access to emergency-related information and trans-
portation (Micevska, 2005; Mechael, 2006). Zum Beispiel, a Ministry of Health
representative in Egypt told how his son contacted his mother to mobilize support
for a stranger he had seen experiencing an accident:
One day my son saw an accident on the detour route, so he took the
mobile of the injured person to call his mother and one of his friends,
and my son stayed with him until the ambulance came, along with his
mother and the friend he called. (Mechael, 2006, P. 129)
In Egypt, people who are involved in or who witness emergency situations
often report using mobile phones to coordinate responses with people who have
access to landline telephones, particularly family and friends (Mechael, 2006).
Increasingly, people carry mobile phones as a way to ensure that they can stay safe
and secure, especially in case of emergency; daher, safety and security are becoming
a part of the technology’s social image (Agar, 2003; Ling, 2004), especially in low-
and middle-income countries with growing numbers of mobile phone users
(Mechael, 2006).
It is important to note that the benefits of mHealth can only be maximized if
all of the elements in the network, including health facilities and professionals, Sind
seen as accessible. In my study in Egypt, I found that people frequently mentioned
six limitations to maximized use of mobile phones for health: (1) cost, (2) percep-
tions of risk, (3) reliability of telephone systems in health facilities, (4) safety, lia-
bility, and cost recovery for unknown contacts as well as information and services
provided at a distance, (5) lack of understanding and use of range of functions
available through mobile phones, Und (6) poor quality of health services (Mechael,
2006).
In that study, one respondent, a pediatric surgeon and professor with a private
clinic, summarized the sentiments of most health professionals. He explained how
he makes efficient use of mobile phone calls for emergencies and general health
service coordination, but still prefers a landline for consultations:
If it is an emergency they [other doctors] call me. Auch, if a colleague
needs me to help him with a surgery, he calls me. They can reach me any-
108
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
The Case for mHealth in Developing Countries
where…. It has facilitated … communications and shortened distances
between my colleagues, my patients, and my students. They can reach me
anytime and anywhere…. I prefer to use the telephone [für] long calls, Wenn
I am going to discuss something with a colleague in a medical case. Aber
if I don’t find him, I have to use the mobile to tell him to call me where I
Bin, meaning that the call from the mobile doesn’t exceed a minute. In
one day I can use the mobile to receive calls and make calls for 5 Zu 6 min-
utes in total. (Mechael, 2006, P. 164)
It is critical to understand such calling preferences and patterns in order to under-
stand the natural role of mobile phones within the health sector. Once we see the
natural patterns, we can begin to formally integrate the technology in order to
maximize health benefits. Overcoming barriers is a strong feature within the liter-
ature on technology for health and development in poor countries; the primary
objective is to ensure effective use of the technology to improve outcomes. Das
area of technology study explores aspects of barriers such as literacy level, hierar-
chical access to technology, appropriate infrastructure to support the use of tech-
nology, and cultural factors that inhibit the use of technology (Mechael, 2006). A
key barrier is cost. Throughout developing countries, efforts are being made to
alleviate some of the cost burden facing health professionals; one approach is giv-
ing them a stipend for their mobile phones. A more formalized approach is used
in Ghana: physicians registered with the Ghana Medical Association can have
unlimited calling through the mobile service operator OneTouch.
While mobile phones are being used throughout the world to support health
activities and organic uses, they also serve as an excellent foundation for formal-
ized programming. A primary area where direct two-way communication can sig-
nificantly improve health care is in reducing maternal mortality. One approach is
to create referral systems that combine communication and access to emergency
Transport, as well as consultative relationships between birth attendants, mid-
wives, and obstetricians so they can better manage labor and delivery complica-
tionen. In addition to personal two-way communication, newly developed automat-
ed systems can provide recorded health-related information.
Formal mHealth initiatives
The more formalized uses of mobile phones and other technologies for health can
be divided into two broad categories: mHealth as an extension of eHealth, Und
mHealth as a subset of mServices. mHealth as an extension of eHealth broadly
encompasses the formal integration of mobile devices within the health sector; als
a subset of mServices, mHealth is used to engage the general public in health-relat-
ed activities. Examples of the former are text-message appointment reminders,
data-collection systems, remote patient-monitoring devices, and mobile medical
records: formalized uses that sit within or are generated by the health sector.
mHealth as an extension of eHealth often begins with small pilot projects that,
if successful and well-funded, may then be replicated and scaled up to larger pop-
Innovationen / Winter 2009
109
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
ulations or sets of facilities. But this progression has been slow. Health-related call
centers and hotlines, mass mobilization campaigns, and mobile phone-based
games fall within the realm of mServices, as they are often provided through
mobile phone operators in partnership with NGOs and software development
firms. While it is more difficult to assess the direct health outcomes of mServices,
they are proving to have a broader reach with a modest investment within a short-
er period of time.
All these factors are making it increasingly important to examine the linkages
between mobile technologies and health, to explore opportunities for larger-scale
implementations, and to engage in research that will enable the health sector to
become more strategic as it leverages enhanced connectivity and increased access
to mobile phones, both within the health sector and across the general population.
In order to maximize health benefits, it is crucial to establish the field of mHealth,
at least temporarily, as an extension and integral part of eHealth, as well as one of
a newly emerging range of mServices. As mobile technology becomes strategically
integrated and implemented at a noticeable scale over a period of time, the field of
mHealth will no longer be necessary, and will revert back to a generalized approach
to the use of emerging technology for health.
mHEALTH AS AN EXTENSION OF eHEALTH
Beyond basic voice communication, data access for health is primarily focused on
the transmission of static text, but it can also extend to interactive decision support
Algorithmen, other visual image information, and to communication capabilities, als
email and SMS features become integrated into basic mobile service. A recent
commentary in the Lancet highlights the need for actively managed efforts to
reduce child and maternal mortality through better use of data; it heralds the
uptake of mobile phones and declining costs of computers as strategic opportuni-
Krawatten (Shankar, Bartlett et al., 2008).
Außerdem, as Brough Turner wrote in a recent report on mobile citizen
media in developing countries, mobile phones are becoming smarter and the
increasing availability of mobile broadband provides more opportunities for real-
time monitoring of a broad range of health data (Verclas & Mechael, 2008).
Integrating the use of GIS and GPS with mobile technologies adds a geographical
mapping component that lets users “tag” voice and data communication to a par-
ticular location or series of locations. This functionality is already being used for
disease surveillance to better mitigate outbreaks and to map gaps in demand for
services and service providers so they can make better informed allocations of
resources. The Nokia Data Gathering platform, as deployed in Amazonia in Brazil
to collect health-related data—although proprietary and built for optimal use on
Nokia phones—is one such application that combines data collection with map-
ping functionality.
These combined capabilities offer potential solutions to health-related prob-
lems in low- and middle-income countries; before mobile phones had spread so
110
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
The Case for mHealth in Developing Countries
widely, the use of information and communication technologies such as comput-
ers and the Internet was hampered by limited access to landline telephones for
dial-up connections and electricity. Mobile communication technologies are
already being used to facilitate access to emergency health services, to survey infec-
tious diseases, to map and research health facilities and services, and in decision
support and mobile telemedicine.
Darüber hinaus, sensor-aided telemedicine devices should generate significant cost
savings for the health sector by reducing the number of patient visits to health
facilities and enhancing doctors’ ability to detect problems that require treatment.
When this happens, as Fuscaldo (2004) puts it, the patient becomes the point-of-
care, rather than the doctor or the hospital. For low- and middle-income coun-
versucht, many such solutions will likely become available in urban centers and then
be used for the extended care of the elderly as the global population ages (Lacal,
2003). Im Gegensatz, rural areas, where infectious disease continues to be the prior-
ity and human resources are limited, will require more basic technological solu-
tionen, such as voice-based tele-consultation between health care providers and cit-
izens (Mechael, 2006).
A comprehensive report from the wireless industry (Wireless Healthcare,
2005) lists 101 specific health-related activities that can be conducted using mobile
Telefone; it highlights many of the newly emerging opportunities to take advantage
of the health sector’s increased access to the technology. Among the many exam-
ples are reminders about appointments and medication, the use of a SIM card to
hold medical data, peer support for patients via mobile phones, support for health
professionals making a diagnosis, and many types of data collection, along with
using phones to control inventory and to contact emergency services.
Such documentation, Jedoch, provides very little specific evidence on how
the use of mobile phones leads to improved health outcomes (Kaplan, 2006;
Vodafone, 2006). The evidence base in relation to mobile phones and health is lim-
ited, largely because the technology is so often integrated as part of a broader
health intervention, and the role of telephones is not necessarily a critical aspect of
the particular study. According to a policy paper from Vodafone (2006), recent
studies of mobile phones and health have largely focused on the potential benefits
of the technology within the health sector and on their use in developed, eher
than developing, Länder. Darüber hinaus, the paper notes, many of the existing stud-
ies look at how the voice and text functions improve access and efficiency within
health care and how young people can access confidential health-related informa-
tion. As other reviewers observe, many of the examples of applications are in the
pilot stage and have yet to be implemented or evaluated on a significant scale.
In a more thorough review, Jedoch, Kaplan (2006) explored studies, primari-
ly conducted in developed countries, that looked at direct interventions in which
mobile and landline telephones were used to address a wide range of health con-
ditions and situations, including diabetes (patient blood sugar level monitoring),
breast cancer (telephone counseling), tuberculosis (adherence to medication),
treatment compliance for a variety of conditions, attendance at health facility
Innovationen / Winter 2009
111
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
appointments, depression outcomes, immunization rates, asthma management,
and smoking cessation. Kaplan specifically explored how people used mobile
phones for the “express purpose of supporting or altering one or more health out-
comes” (P. 2). The studies he found were primarily small pilot projects that offered
mixed results in terms of demonstrating the potential of landlines and mobile
phones to serve as a support for more effective delivery of health care services.
The main feature of mobile phones that has been most significantly docu-
mented in the context of health is text messaging, which has garnered increasing
attention in the United Kingdom, the United States, Norwegen, and Sweden as a
means of reminding patients about their appointments (The Economist, 2006).
The preliminary results from such studies indicate that more people show up at
their scheduled appointments, yielding significant savings in health costs for facil-
ities and practitioners. In this case, the benefit is related to costs rather than to
health outcomes.
A related use of text messaging for health is the SimPill system, initially devel-
oped in South Africa to manage TB patient treatment compliance. A device
attached to a medicine bottle sends a text message to a central computer database
when the cap is removed. When the cap is not removed according to the specified
treatment regimen, the system sends a text message to the patient, with a reminder
to take the medication; thus it may improve treatment compliance (Der Ökonom,
2005). SMS text messaging has also been highlighted as a preferred means of com-
munication for those mobilizing support and communicating during emergency
and disaster situations, largely because the landline networks may not be reliable
(GSM Association, 2005).
SMS is also being used increasingly in data collection systems that use encod-
ed SMS strings; organizations such as UNICEF use them to manage the supply
chain and monitor key health-related data, such as the availability and quality of
pit latrines for preventing diarrhea. Open Source developers have also responded
to the overwhelming demand for data collection systems by developing PDA plat-
forms that are increasingly being migrated to smart phones, including EpiHandy
and EpiSurveyor. OpenRosa, a community of java-based mobile phone develop-
ers, has formed to reduce the duplication of efforts and to ensure that common
standards are adopted. And both corporate and social interests are driving the
development of more robust data collection platforms, such as Nokia Data
Gathering, mentioned above, which recently completed a trial in the Brazilian
Amazon with health workers; through a partnership with the Ministry of Health,
it will be implemented on a national scale.
Mobile phones are also being used within the rollout of broader health-relat-
ed technology systems. Zum Beispiel, Voxiva has developed a proprietary system
called TracNet; it enables health care workers in Rwanda to use their mobile
phones to send health monitoring reports to a centralized database for real-time
health information analysis on HIV and AIDS.2 TracNet was designed to leverage
the existing telephone infrastructure, which includes an inadequate landline infra-
Struktur, more plentiful mobile phones, and some satellite telecommunications
112
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
The Case for mHealth in Developing Countries
Systeme. The program, which tracks patient diagnostic and treatment information
in Rwanda, is among the first of its kind to be implemented on a national scale; Es
covers 75 percent of the country’s 340 clinics (32,000 Patienten) and allows health
care workers to access patient information even when they have moved from one
clinic to another (Crampton, 2007).
But no one solution is available everywhere. Infolge, health administrators
and technology developers have started combining different technologies based on
the environments where they are used. Zum Beispiel, in South Africa a shortage of
qualified pharmacists is creating a serious bottleneck in treating people with HIV
and AIDS, and rural clinics often cannot distribute medication. Cell-Life, a recog-
nized leader in the mHealth field, developed a system that combines a cell phone,
the Internet, and computers in various locations; it allows pharmacists in better-
equipped clinics to package drugs for rural clinics that do not have a pharmacist
(Mechael & Sloninsky, 2008). Ähnlich, a project with which I have been involved,
the Millennium Villages Project, which operates in ten countries in Africa, is inte-
grating mobile technologies as part of a broad-based mHealth strategy in partner-
ship with Ericsson and key operators; it aims to extend existing eHealth systems to
support the work of community health workers and facility-based staff to achieve
the MDGs for health from the ground up. A consortium of Open Source develop-
ers and program implementers, currently known as the OpenMobile Consortium,
is forming to develop a toolkit of mobile phone-based applications that can be
used in a similar ecosystem approach; their focus goes beyond health to all aspects
of social development in low- and middle-income countries. Many of these plat-
Formen, when applied to mHealth, span eHealth as well as mServices.
mHEALTH WITHIN mSERVICES
In a recent push to identify “the M-PESA of mHealth,” the business community
has been eager to assess the case for mHealth as part of a broader range of
mServices. The business case for mHealth will likely come in two streams. Der erste
will identify revenue-generating services and applications that provide a profitable
return on investment, as people buy specialized handsets and subscribe to value-
added services, or networks carry increasing amounts of voice and data traffic.
Viewed as a win-win for industry and health, in this stage more hotlines and call
centers will be created that allow people to access general and targeted health infor-
mation and to use text messaging creatively for social mobilization. A key benefit
of call centers is that they require little investment up front but have the potential
for a broad reach.
One such call center in a developing country context is the health-related
extension of the Grameen Bank’s Village Phone Program, called the Grameen
Healthline, which launched in November 2005.3 The system provides a number
for the general public; it connects an individual to a registered physician who pro-
vides advice and referrals for both emergency and routine health conditions. Der
costs of the call are subsidized, but paid by the caller. As of October 2007, the pro-
Innovationen / Winter 2009
113
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
gram was providing medical advice to approximately 10,000 callers per day.
Beyond voice, a few emerging programs are using text messaging to engage the
general public for health promotion. Ein Beispiel, in Mbarara, Uganda, is a part-
nership between the AIDS Information Center (AIC) in Uganda and Zain, a local
mobile phone network operator, in collaboration with Text to Change, a non-
governmental organization that uses a bulk short message service platform for
HIV/AIDS education (IRIN PlusNews, 2008). The pilot program, launched on
Februar 14, 2008, sent an introductory SMS to a list of 15,000 subscribers asking
if they would like to participate in a no-cost interactive quiz about HIV, Und
etwa 2,500 participated (IRIN PlusNews, 2008).
The aim of the program was to increase voluntary counseling and testing for
HIV; in fact, HIV testing at AIC’s central facility in the Mbarara district increased
von 100 percent over the six-week period of the trial program. The project could
also track knowledge about HIV through people’s responses (IRIN PlusNews,
2008). This shows how valuable it is to strengthen the health sector’s capacity to
develop mobile technology-based solutions and to help operators provide more
comprehensive and affordable services to the health sector. Many more such proj-
ects are needed. This platform can also provide other subscription-based services
that will generate revenue alongside its social purpose for self-sustainability.
The second business stream will explore the social marketing of technology to
the health sector in a way that encourages governments to invest in mHealth-relat-
ed services so they can both reduce the cost burden of service delivery and improve
health outcomes. Here a key effort will be exploring how mobile technologies and
related services can be integrated within government strategies to strengthen
health systems. As companies involved in mobile telecommunications increasing-
ly seek to expand their market to the health sector, they will have to develop a prac-
tical way to use technology to solve key health-related problems and then scale
them up so they both create efficiencies and generate positive health outcomes.
For middle- and low-income countries, where health care resources are often
stretched already, it becomes even more critical to begin by defining the problem,
exploring existing technology solutions, and then identifying and testing the most
appropriate solution, or a combination of solutions. Such efforts are best
approached as a public-private partnership between governments, non-govern-
mental organizations, and telecommunications companies.
These points lead to my set of recommendations for implementing mHealth at
the national scale:
• Assess the current state of eHealth, telemedicine, and mHealth. Then use these
assessments to identify informal/organic practices and formal mHealth imple-
mentations, opportunities to strengthen or extend existing eHealth systems to
more remote areas, and gaps in information and communication flows that can
be supported through mobile technologies.
• Identify and document existing eHealth/telemedicine initiatives and systems, Zu
ensure that they are interoperable and use an ecosystem approach, sowie
formal and informal mHealth practices.
114
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
The Case for mHealth in Developing Countries
• Identify priority diseases and health conditions, including country-specific
MDG targets, and explore critical pathways for integrating or extending tech-
nology.
• Examine and document current workflow and working relationships (informa-
tion and communication).
• Identify the role of voice and visual data or other media and channels.
• Identify eHealth capacity and business cases for services including software
customization, project management, monitoring and evaluation.
• Develop a short- and long-term strategic plan, implementation plan, and budg-
et and define roles and responsibilities as well as mechanisms for accountabili-
ty.
• Develop guidelines, policies, and accountability systems.
• Establish targets and measures of success.
• Monitor and evaluate and adapt to findings and changing environment.
Three factors will likely contribute to making mHealth solutions scalable, als
would be true for any sort of service: (1) increased demand for the services from
consumers; (2) strategic partnerships between industry, governments, imple-
menters, and researchers to support large-scale implementation and evaluation of
bottom-up and top-down mHealth systems and applications, Und (3) an enabling
policy and operational environment. Zum Beispiel, one mHealth system that shows
promise for implementation at national scale is a current effort in Tanzania to link
an Open Source mobile data collection platform with the computerized District
Health Information System (DHIS), and also with clinical records databases; Die
database can then submit data to the DHIS to allow decentralized but comprehen-
sive reporting of household and clinic-based data.
CONCLUSION
The specific potential of mHealth lies in its ability to offer opportunities for direct
voice communication (particularly valuable given the literacy and language capac-
ity in many countries) along with capabilities for information transfer that previ-
ous technologies did not offer. This is predominantly beneficial for work in remote
areas where the mobile phone, and now increasingly the wireless infrastructure,
can reach more people more quickly. As a result of such technological advances,
the capacity for improved access to information and two-way communication
becomes available at the point of need and for healthcare workers at the point of
care. Mobile communication technologies are tools that can be leveraged to sup-
port existing workflows within the health sector and between the health sector and
the general public.
Studies on technology and health provide a critical lens through which to
review existing technological trends and applications, and four findings from those
studies are particularly important here. Erste, mobile technologies are not objec-
tives, but tools that should be applied in order to achieve local, National, Und
regional health objectives (Shields, Chetley et al., 2005) and to help improve the
Innovationen / Winter 2009
115
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
lives of individuals (SatelLife, 2005). Zweite, we do not have enough impact data
to understand how mobile technologies are influencing health outcomes, so a chal-
lenge remains: how to identify and replicate best practices (Mechael & Sloninsky,
2008). We will need more impact evaluation in order to move beyond discussions
of the potential impact that they might have and anecdotal examples of how they
are already being used. Dritte, mobile technologies are only as good as the infor-
mation and communication to which they provide access (Shields, Chetley et al.,
2005). It is crucial to have access to reliable and relevant content that reflects con-
ditions in low- and middle-income countries at the right time (Mechael &
Sloninsky, 2008). Endlich, we need to move away from pilot programs and case
studies to more formal applications and more thorough studies that can establish
the foundation for national programs and policies (Shields, Chetley et al., 2005).
The use of mobile communication technologies for health, or mHealth, is a
newly evolving sub-field within eHealth and mServices. The future of mHealth
will depend on the establishment of a critical knowledge and evidence base that
will enable health administrators and policymakers to make better informed deci-
sions about how to invest limited health resources in technology. To make this hap-
pen, projects will need to be implemented at a large enough scale to generate
results, using research protocols that can demonstrate where, Wie, and why
mHealth works best.
The starting point for considering the potential impact of ICT should be a
broad-based assessment of organic mHealth practices and health-related needs. Bei
the global scale, it can begin with broad-based health priorities such as the
Millennium Development Goals, Roll-back Malaria,4 Stop-TB,5 and improving
human resources for health, unter anderen. These efforts highlight concrete aims
and objectives, with specific targets that countries have adopted within their
national health strategies. At the moment, there is significant momentum and con-
vergence to create an enabling environment for mHealth with high-profile part-
nerships and media coverage. There is even a growing spirit of “co-opetition” for
telecommunications companies, as an industry colleague mused: even those who
traditionally are economic rivals can together support a fairer operating environ-
ment for social entrepreneurs, NGOs, and government social services. The oppor-
tunities for leveraging the potential of technology form an endless list of possibil-
ities both to create efficiencies within health systems in poor countries and to pos-
itively influence health outcomes, while also creating new revenue streams for
telecommunications hardware, Software, and voice and data service providers.
At the close of 2008, as an outgrowth of the first ever, week-long consultation
on mHealth, hosted by the Rockefeller Foundation and convened by the UN
Foundation and Vodafone Group Foundation, discussions and actions have
focused on creating a neutral coordinating and advocacy body to take on this
mHealth call to action. It is my sincere hope that the current wellspring of inter-
est in mHealth will advance the current state of anecdotal potential, translating it
into tangible improvements in health for years to come.
116
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
The Case for mHealth in Developing Countries
Endnotes
1. http://www.internetworldstats.com/stats.htm.
2. http://www.voxiva.com/rwanda.asp.
3. http://www.grameenphone.com/index.php?id=106.
4. http://www.rbm.who.int/.
5. http://www.stoptb.org/.
Verweise
Agar, J. (2003). Constant Touch: A Global History of the Mobile Phone. Cambridge, England: Icon
Books Ltd.
Crampton, T. (Marsch 5, 2007). “Wireless Technology Speeds Health Services in Rwanda.” New York
Times. http://www.nytimes.com/2007/03/05/technology/05wireless.html
Fuscaldo, D. (Dezember 15, 2004). “Soon, Cellphones Will Monitor the Vital Signs of the
Chronically Ill.” The Wall Street Journal On-line.
http://www.wirelesslifesciences.org/pdfs/WSJ1_12152004_Cellphones.pdf
GSM Association (2005). The Role of Mobiles in Disasters and Emergencies. London: GSM
Association.
Harrison, G., S. Zaghloul, et al. (1993). “Breastfeeding and Weaning in a Poor Urban Neighborhood
in Cairo, Ägypten: Maternal Belief and Perceptions.” Social Science and Medicine 38(8): 1063-1069.
IRIN PlusNews (2008). “Uganda: Using mobile phones to fight HIV.”
http://www.plusnews.org/Report.aspx?ReportId=80176
Istepanian, R. (2004). “Introduction to the Special Section on M-Health: Beyond Seamless Mobility
and Global Wireless Health-care Connectivity.” IEEE Transactions on Information Technology in
Biomedicine 8(4): 405-413.
Istepanian, R. and J. Lacal (2003). “Emerging Mobile Communication Technologies for Health:
Some Imperative notes on m-Health.” Paper presented at the 25th International Conference of the
IEEE Engineering in Medicine and Biology Society, Cancun, Mexiko.
Kaplan, W. A. (2006). “Can the ubiquitous power of mobile phones be used to improve health out-
comes in developing countries?” Globalization and Health 2(9): 1-14.
Lacal, J. (2003). “Cell Phones and telemedicine.” Paper presented at the Fifth International
Workshop on Enterprise Networking and Computing in the Healthcare Industry, Santa Monica,
Kalifornien.
Ling, R. (2004). The mobile connection: The cell phone’s impact on society. London: Morgan
Kaufmann.
Mechael, P. (2006). Exploring Health-related Uses of Mobile Phones: An Egyptian Case Study. PhD
Thesis completed at London School of Hygiene and Tropical Medicine.
Mechael, P. and D. Sloninsky (2008). “Towards the Development of an mHealth Strategy: A
Literature Review.” Working paper. New York: Earth Institute at Columbia University.
Micevska, M. (2005). “Telecommunications, Public Health, and Demand for Health-Related
Information and Infrastructure.” Information Technology and International Development 2(3): 57-
72.
SatelLife (2005). Handhelds for Health: SatelLife’s Experiences in Africa and Asia. Watertown, MA:
SatelLife.
Shankar, A., L. Bartlett, et al. (2008). “Delivery on MDG 5 by active management with data.” The
Lancet 371(April 12, 2008).
Shields, T., A. Chetley, et al. (2005). ICT in the health sector: Summary of the online consultation.
Innovationen / Winter 2009
117
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023
Patricia N. Mechael
InfoDev Working Paper. www.infodev.org/en/Document.84.aspx
Der Ökonom (September 15, 2005). “The doctor in your pocket.”
Der Ökonom (Marsch 24, 2006). “A text a day.”
UNICEF (2008A). Progress for Children: A World Fit for Children Statistical Review. New York:
UNICEF.
UNICEF (2008B). Progress Report for Children: A Report Card on Maternal Mortality. New York:
UNICEF.
United Nations (2000). “United Nations Millennium Declaration” (General Assembly Resolution
55/2). New York: United Nations.
Verclas, K. and P. Mechael (2008). A Mobile Voice: The Use of Mobile Phones in Citizen Media. Neu
York: MobileActive.org.
Vodafone (2006). The role of mobile phones in increasing accessibility and efficiency in healthcare.
London: Vodafone.
Wireless Healthcare (2005). 101 Things to do with a Mobile Phone in Healthcare.
World Health Organization (1946). The Constitution of the World Health Organization. Genf:
WHO.
World Health Organization (1978). Declaration of Alma-Ata. International Conference on Primary
Health Care, Alma-Ata, UdSSR. Genf: WHO.
World Health Organization (2005). eHealth Tools and Services: Needs of Member States. Genf:
WHO.
World Health Organization (2006). The World Health Report 2006: Working Together for Health.
Genf: WHO.
118
Innovationen / Winter 2009
Von http heruntergeladen://direct.mit.edu/itgg/article-pdf/4/1/103/704309/itgg.2009.4.1.103.pdf by guest on 07 September 2023