INVESTIGACIÓN
Epileptogenic Networks in
Extra Temporal Lobe Epilepsy
Gerard R. Hall1
, Frances Hutchings1, Jonathan Horsley1, Callum M. Simpson1,
Yujiang Wang1,2,3, Jane de Tisi2,4, Anna Miserocchi2, Andrew W. McEvoy2, Sjoerd B. Vos5,
Gavin P. Winston2,6, John S. Duncan2,4, and Peter N. Taylor1,2,3
1CNNP Lab, Interdisciplinary Computing and Complex BioSystems Group, School of Computing,
Newcastle University, Newcastle upon Tyne, Reino Unido
2Department of Epilepsy, UCL Queen Square Institute of Neurology, Londres, Reino Unido
3Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, Reino Unido
4UCL/ UCLH NIHR University College London Hospitals Biomedical Research Centre, Londres, Reino Unido
5Centre for Microscopy, Characterisation, and Analysis, University of Western Australia, Nedlands, Australia
6Department of Medicine, Division of Neurology, Queen’s University, Kingston, Canada
Palabras clave: Extra temporal lobe epilepsy, Diffusion MRI, Epileptogenic zone, Structural connectivity,
Resection, Seizure, Tractography, Connectome, Red
ABSTRACTO
Extra temporal lobe epilepsy (eTLE) may involve heterogenous widespread cerebral networks.
We investigated the structural network of an eTLE cohort, at the postulated epileptogenic zone
later surgically removed, as a network node: the resection zone (RZ). We hypothesized
patients with an abnormal connection to/from the RZ to have proportionally increased
abnormalities based on topological proximity to the RZ, in addition to poorer post-operative
seizure outcome. Structural and diffusion MRI were collected for 22 eTLE patients pre- y
post-surgery, and for 29 healthy controls. The structural connectivity of the RZ prior to surgery,
measured via generalized fractional anisotropy (gFA), was compared with healthy controls.
Abnormal connections were identified as those with substantially reduced gFA (z < −1.96). For
patients with one or more abnormal connections to/from the RZ, connections with closer
topological distance to the RZ had higher proportion of abnormalities. The minority of the
seizure-free patients (3/11) had one or more abnormal connections, while most non-seizure-
free patients (8/11) had abnormal connections to the RZ. Our data suggest that eTLE patients
with one or more abnormal structural connections to/from the RZ had more proportional
abnormal connections based on topological distance to the RZ and associated with reduced
chance of seizure freedom post-surgery.
AUTHOR SUMMARY
Focal epilepsy describes seizures that originate at one or more location. A significant
proportion of cases, however, are unresponsive to drug treatment; therefore, surgery remains
an important and effective treatment in stopping seizures. We wanted to further understand the
nature of these networks associated with epilepsy and how they contribute to post-surgical
outcome. Our research asked three questions: Does distance to the clinically suspected site
of the epilepsy increase the likelihood of network abnormality? Can an upstream abnormal
connection to a region increase the chance of abnormal connections downstream? Can
the presence of abnormal connections explain post-operative outcome in terms of seizure
a n o p e n a c c e s s
j o u r n a l
Citation: Hall, G. R., Hutchings, F.,
Horsley, J., Simpson, C. M., Wang, Y.,
de Tisi, J., Miserocchi, A., McEvoy,
A. W., Vos, S. B., Winston, G. P.,
Duncan, J. S., & Taylor, P. N. (2023).
Epileptogenic networks in extra
temporal lobe epilepsy. Network
Neuroscience. Advance online
publication. https://doi.org/10.1162
/netn_a_00327
DOI:
https://doi.org/10.1162/netn_a_00327
Supporting Information:
https://doi.org/10.1162/netn_a_00327
Received: 21 December 2022
Accepted: 22 June 2023
Corresponding Author:
Gerard R. Hall
gerard.hall@newcastle.ac.uk
Handling Editor:
Olaf Sporns
Copyright: © 2023
Massachusetts Institute of Technology
Published under a Creative Commons
Attribution 4.0 International
(CC BY 4.0) license
The MIT Press
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
/
.
/
t
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Epileptogenic networks in extra temporal lobe epilepsy
Focal epilepsy:
Major type of epilepsy where
symptoms are generated from a
particular location of the brain.
Seizure onset zone (SOZ):
The true location(s) in the brain
where seizures originate and from
where they can subsequently spread.
Resection zone (RZ):
The location of the brain that has
been removed by surgical resection.
Extra temporal lobe epilepsy (eTLE):
A subtype of focal epilepsy that is
situated in regions other than the
temporal lobe.
freedom? We hope our work will shed light on epileptogenic networks and potentially
stimulate new ideas and discussions to investigate brain networks in epilepsy.
INTRODUCTION
Epilepsy is a major neurological condition affecting over 50 million people worldwide. Char-
acterized by recurring spontaneous seizures, with transient changes in awareness and/or
behavior, epilepsy can lead to long-term cognitive, neurobiological, psychosocial morbidity,
and premature mortality (Fisher et al., 2014). Focal epilepsy accounts for 60% of adult epi-
lepsy and describes seizures as originating from a particular location in the brain, termed
the seizure onset zone (SOZ) (Tellez-Zenteno & Hernandez-Ronquillo, 2012). Epilepsy surgery
involves the resection of the area thought to be involved in generating seizures, with the sub-
sequent resected area termed the resection zone (RZ). Temporal lobe epilepsy (TLE) resections
are most common, with the remaining third of focal epilepsies arising outside the temporal
lobe (Chowdhury, Silva, Whatley, & Walker, 2021; Delev et al., 2019). Extratemporal lobe
epilepsy (eTLE) may arise from numerous sites in the brain and, inevitably, cohorts are
heterogenous.
Imaging modalities have provided valuable insights into eTLE, from analyzing the structure
of pathology to help classify and understand eTLE subtypes (Hong, Bernhardt, Schrader,
Bernasconi, & Bernasconi, 2016; Wagstyl et al., 2022), to reporting alterations in widespread
functional networks across the brain (Carboni et al., 2020; Hong et al., 2019; Kini et al.,
2019; Ridley et al., 2015), to identifying distant structural networks that result in long-term
seizure freedom if disconnected (Giampiccolo et al., 2023). Diffusion MRI (dMRI) has been
important in understanding the role of structural networks in epilepsy. Focal epilepsies affect
a widespread network rather than a localized zone (Englot, Konrad, & Morgan, 2016), from spe-
cific connections (Giampiccolo et al., 2023) to widespread global changes (Tavakol et al.,
2019). A recent large-scale multicenter study (21 cohorts, 1,249 total patients) reported wide-
spread reductions in dMRI measures of fractional anisotropy (FA) in 36 of 38 major connective
tracts when comparing all epilepsy types against controls (Hatton et al., 2020). Changes in
connective tracts were also present in TLE and eTLE with no visual MRI pathology. Left and
right TLE were associated with lower FA in 20 and 19 connective regions, respectively; those
with eTLE had lower FA in 33 connective regions, compared with controls. These findings
support the importance of understanding network mechanisms in focal epilepsy and suggest
that connectivity changes are widespread, in eTLE and TLE.
Connectivity abnormalities in TLE are better understood than in eTLE. In TLE, specific
changes in white matter connections have been identified and reproduced across studies,
and in some cases have been shown to be widespread (Ashraf-Ganjouei et al., 2019; Chiang,
Levin, Wilde, & Haneef, 2016; Hatton et al., 2020). Structural connectivity in TLE has also
been linked to epilepsy duration (Chiang et al., 2016; Owen et al., 2021). Structural network
disorganization has been associated with increased cognitive deficits in TLE, and it is more
closely associated to changes in cognition than morphological abnormalities (Hatton et al.,
2020). Many studies used network connectivity to predict patient outcomes from epilepsy sur-
gery (Bonilha et al., 2006; Kreilkamp, Weber, Richardson, & Keller, 2017; Munsell et al., 2015;
Sinha et al., 2021; Taylor et al., 2018), finding that incomplete resection of white matter abnor-
malities is associated with worse seizure outcomes (Kreilkamp et al., 2017; Sinha et al., 2021).
Despite the multitude of TLE studies, it is not clear whether widespread network abnormalities
relate to patient outcome in eTLE.
Network Neuroscience
2
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
/
.
/
t
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
t
.
/
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Epileptogenic networks in extra temporal lobe epilepsy
ILAE score:
A score that describes post-surgical
seizure recurrence, ranging from 1
(no seizures or auras) to 6 (significant
increase in seizures and auras after
surgery).
Compared with TLE, less is known about brain network (re)organization in eTLE. One major
reason for this knowledge gap is that TLE diagnosis is far more common. Furthermore, TLE is
more homogenous in localization comprising just the temporal lobe, and usually the hippo-
campus. In contrast, eTLE can appear in any part of any other lobe. These factors make group
studies in eTLE challenging, and novel approaches are needed to take this heterogeneity of
localization into account.
The current study addresses three goals: (a) Develop a method to investigate the network
connectivity of the RZ, irrespective of eTLE RZ location. (b) Identify network abnormalities in
structural connectivity of the RZ prior to surgery. (c) Determine whether the presence of
abnormal RZ connectivity pre-surgery influences post-operative seizure outcome.
MATERIAL AND METHODS
Participants
We studied 22 individuals with drug-resistant eTLE who underwent pre-surgical evaluation
and subsequent resection, and 29 healthy controls. None had previous neurosurgery. MRI
scanning was obtained before and 3–4 months after surgery. All participants were scanned
with the same acquisition protocol. Sixteen patients had focal cortical dysplasia, with the
remaining patients having gliosis (n = 4), cavernoma (n = 1), and dysembryoplastic neuro-
epithelial tumor (n = 1). Seizure outcome after surgery was classified with the International
League Against Epilepsy (ILAE) (Wieser et al., 2001) seizure outcome scale up to 6 years
post-surgery. The last reported ILAE score for each patient was used as their symptom status
post-surgery. Post-surgical seizure outcome was defined as the following: ILAE score of 1 or 2
as free of disabling seizures, and ILAE score of 3 or more as non-seizure-free. Outcome groups
did not differ in duration of follow-up (p = .24, two-tail Mann-Whitney test).
MRI Acquisition and Preprocessing
T1-weighted (T1w) and diffusion-weighted MRI were obtained using a 3T GE Signa HDx scan-
ner equipped with an 8-channel phased array coil. Pre- and post-surgical T1w imaging was
performed with an IR-FSPGR acquisition with the following parameters (TE = 3.04 ms, TR =
37.68 s, 170 contiguous, 1.1-mm-thick coronal slices containing 256 × 256 matrix, 0.9375 ×
0.9375 mm in-plane resolution). Diffusion MRI was collected using a cardiac triggered single
shot EPI acquisition (TE = 73 ms, TR = heart-rate dependent, b-value of 1,200 mm2 [δ = 21 ms,
Δ = 29 ms, using maximum gradient strength of 40 mT m−1], 52 directions with 6 B0s. Overall
60 axial slices were collected, each 2.4 mm thick containing 96 × 96 matrix, zero-filled to
128 × 128, 1.875 × 1.875 mm in-plane resolution). All post-operative scans were collected
within 12 months after surgery.
All patient pre-operative T1w structural scans underwent the standard recon-all pipeline
from the FreeSurfer toolbox (version 6.0.1) (Fischl, 2012). We used the Lausanne atlas
(Hagmann et al., 2008) to parcellate the brain into 128 regions of interest. Post-operative
T1w structural scans then underwent a rigid-body linear registration (6 DOF) using FSL’s FLIRT
(Jenkinson, Bannister, Brady, & Smith, 2002; Jenkinson & Smith, 2001) to the corresponding
pre-operative T1w output from FreeSurfer. Once the post-operative image was aligned with the
pre-operative T1w image, tissue removed during surgery was delineated in the pre-operative
space using FSLView. All patient resection masks were drawn manually to account for possible
changes in morphometry of the remaining tissue (i.e., sagging and/or shrinking resulting from
removal of neighboring supporting structure and/or oedema). Locations and overlap of the
Network Neuroscience
3
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
/
/
t
.
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
t
/
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Epileptogenic networks in extra temporal lobe epilepsy
resection masks between seizure outcome and all patients is displayed in Supplementary
Figure S1.
Patient pre-op and healthy control diffusion-weighted images (DWI) were initially corrected
for signal drift (Vos et al., 2017), then eddy current and movement artifacts were corrected
using the eddy_correct tool, and b-vectors were rotated accordingly (Jenkinson, Beckmann,
Behrens, Woolrich, & Smith, 2012). The DWI were input into DSI studio (version
08.11.2020) and underwent the standard q-space diffeomorphic reconstruction (QSDR) (Yeh
& Tseng, 2011) with a diffusion sampling length ratio of 1.25. All reconstructions were aligned
and normalized to the ICBM152 template using a linear registration consisting of an affine
transformation (12 degrees of freedom) and nonlinear registration using diffeomorphic map-
ping. Images were then interpolated to a 1.875 mm isotropic resolution using a cubic spline
(Yeh et al., 2018).
dMRI Postprocessing
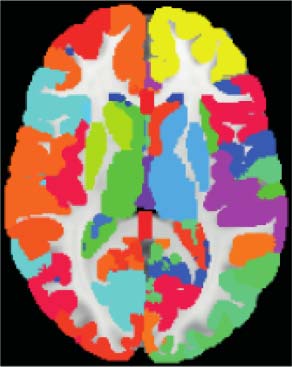
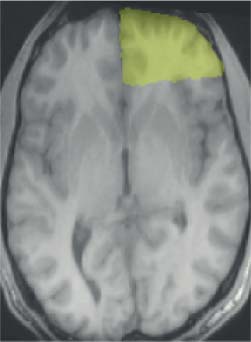
The following steps are illustrated in Figure 1. Each manually drawn resection mask was
imported as an additional region in the Lausanne atlas originally consisting of 128 cortical
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
.
/
t
/
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
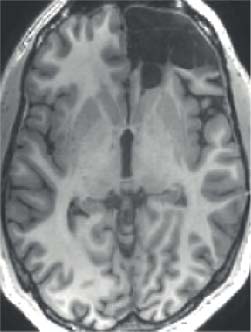
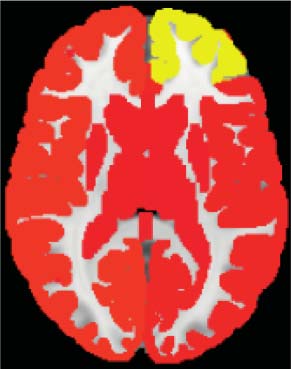
Figure 1. Methods to compare abnormality of the RZ prior to surgery, in a heterogenous eTLE cohort. (Step 1) Resection zone (RZ) delineated
in the post-operative T1w scan. (Step 2) The mask is manually drawn in the pre-operative T1w space using the post-operative T1w scan as an
anatomical reference. (Steps 3 and 4) Resection mask is imported into the atlas as a new region, removing previous areas in that location. (Step
5) Connectivity matrix is built for each patient and controls to the corresponding specific patient atlas created in Steps 1–4. Tractography
streamlines are imported from the HCP842 population average. GFA is used as a measure inferring connectivity strength. (Step 6) Connectivity
strengths for connections to the specific resection location for an individual patient are compared with the same RZ area for the control group.
The z-score is then generated by comparing the individual patient with the controls as a measure of abnormality. (Step 7) Z-scores are com-
pared between patients to perform group analyses (e.g., of seizure outcome, proportion of abnormal connections).
Network Neuroscience
4
Epileptogenic networks in extra temporal lobe epilepsy
Tractography:
A technique that models diffusion
MRI data into a three-dimensional
representation of white matter fiber
connections.
Generalized fractional anisotropy
(gFA):
A measure of the diffusion shape in
terms of anisotropy. It is similar to
fractional anisotropy but calculated
using the orientation distribution
function.
Abnormal connection:
A connection that has gFA lower than
the 5th percentile of the control
distribution for that connection.
and subcortical regions (Hagmann et al., 2008) to create a specific atlas for each individual
patient (Figure 1, Step 4). We imported the HCP tract template (Yeh et al., 2018) instead of
building our own tractography to infer connectivity for four major reasons: (a) Our dMRI
data had relatively low angular resolution. (b) Our data had a non-isotropic-sized voxel
resolution. (c) Using standardized tracts aided in the replicability of z-scores for normative
mapping between patients and controls. (d) Atlas tracts were manually inspected by expe-
rienced neuroanatomists. Following from large-scale epilepsy studies reporting widespread
reductions of FA in all epilepsies (Hatton et al., 2020), structural connectomes were built
using generalized fractional anisotropy (gFA) as a measure of connectivity strength, as gFA
provides more robust estimations of anisotropic diffusion at crossing fibers than does frac-
tional anisotropy (Glenn, Helpern, Tabesh, & Jensen, 2015) (Figure 1, Step 5). Streamlines
ending in gray matter for regions were counted as connected. Using the HCP842 tracts to
infer connectivity coupled with gFA as a measure of connective strength, structural connec-
tomes were built for each patient and for the control group, with each corresponding
patient atlas.
To remove the confound of age on gFA, we modeled the effect of age using a robust linear
regression model from the control group and regressed out the effect for all patients (n = 22)
and controls (n = 29). After correction, connectivity to a region of interest such as the RZ was
analyzed between an individual patient and their controls to generate a z-score representing
the relative abnormality pre-surgery. All z-scores were calculated at each individual
connection.
Statistical Testing
As the resection location and size widely varied between patients, we analyzed the proportion
of abnormal connections relative to the total number of connections (proportion of abnormal-
ity). Following from previous large-scale multicenter research and systematic reviews reporting
a reduction of diffusion anisotropy in epilepsy (Hatton et al., 2020; Slinger, Sinke, Braun, &
Otte, 2016), abnormal connections were defined as those with substantially reduced gFA,
under the 5th percentile (z-score less than −1.96).
To analyze a topological distance effect from the RZ for abnormal connections, patients
with at
least one single abnormal connection were included in a hierarchical model
(Figure 2D). With patient as a random effect, we analyzed the magnitude of connection
abnormality against connection type. The connection type was specified as follows: Primary
connections were those directly connected to/from the RZ, while secondary connections were
those with direct connections to nodes that have a primary connection but not to the RZ. This
process was repeated with topological distance to tertiary, and ultimately to quaternary
connections that were topologically far from the RZ. All connections were specified as either
primary, secondary, tertiary, or quaternary.
We tested whether nodes directly connected to the RZ via an abnormal connection had
more abnormal onward connections. We used a paired t test to analyze the proportion of
abnormal connections between nodes that were directly connected to the resection tissue
via a normal (normal node) or abnormal (abnormal node) connection. Lastly, to test
whether a group difference in post-operative seizure freedom was evident between patients
with one or more abnormal connections to/from the RZ, we used a chi-square test to test
differences in seizure outcome between patients who had one or more abnormal connec-
tions compared with patients having no abnormal connections to/from the pre-surgical
resection area.
Network Neuroscience
5
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
.
/
/
t
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Epileptogenic networks in extra temporal lobe epilepsy
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
.
t
/
/
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
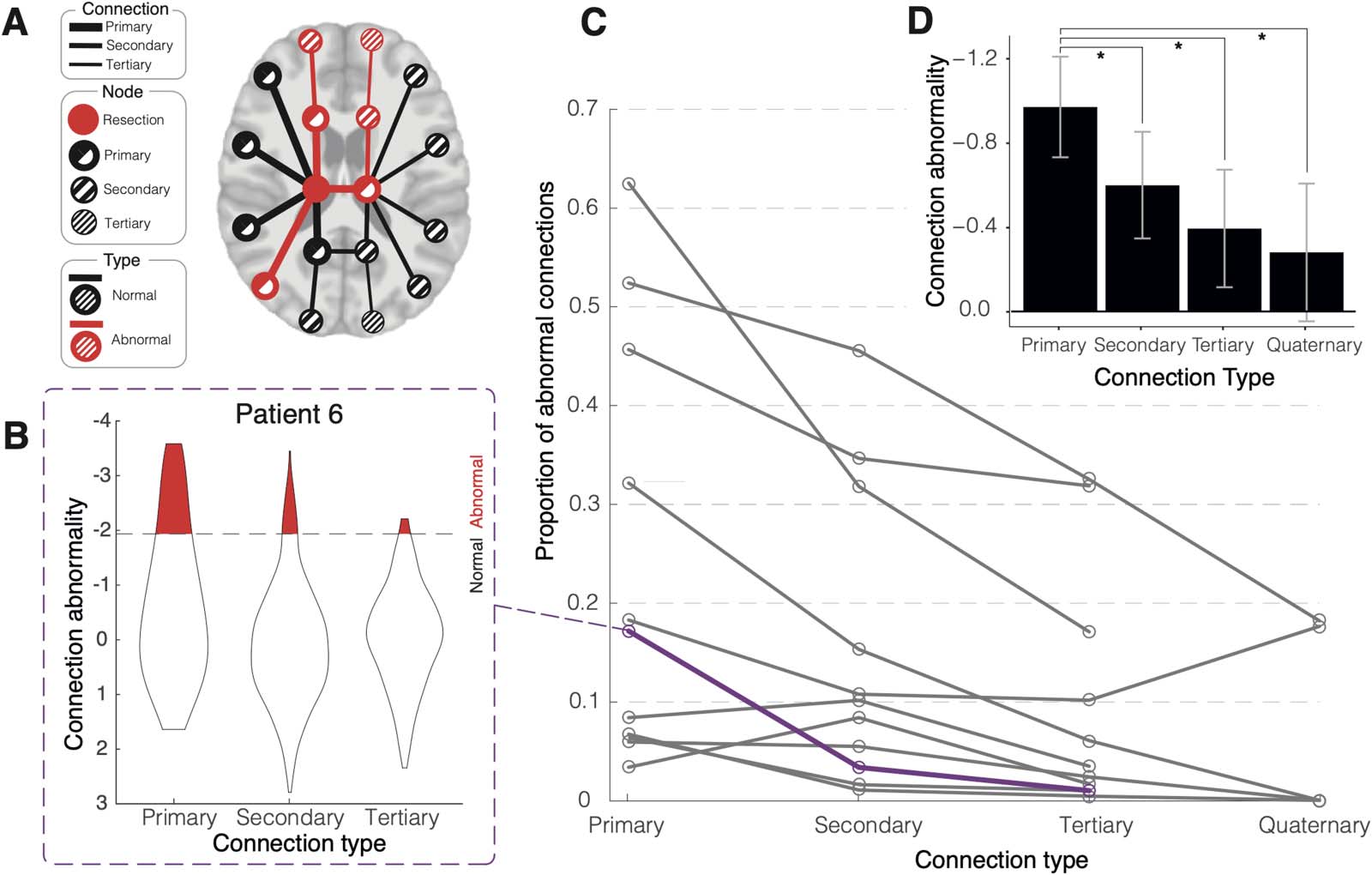
Figure 2. Proportion of abnormal connections decreases with greater topological distance from the resection zone (RZ). (A) Illustration
displaying reduced proportional abnormality further from the RZ. In this schematic illustration, three of seven direct RZ connections are abnor-
mal, representing 42.8% of all primary connections. There are five secondary connections (i.e., connections one step removed from the RZ), of
which two (40%) are abnormal. Of the three tertiary connections, only one (33.3%) is abnormal. (B) Example violin plot of all z-score
connections between differing nodal distances for a single patient highlighted in panel C. Abnormal threshold set at z < −1.96. (C) Proportion
of abnormal connections for each patient (n = 11 had at least one abnormal primary connection) at each nodal distance to RZ. Greater network
distance from RZ is associated with fewer abnormalities. The purple line indicates the example patient from panel B. Patients without any
abnormal primary connections are omitted for clarity. (D) Hierarchical modeling of the patients in panel C. Connections to primary nodes had
significantly more abnormal values compared with subsequent node connections, when accounting for patient as a random intercept, thus
confirming the visual impression of panel C (p < .05).
RESULTS
Connectivity Abnormalities Decrease as Topological Distance Increases for Patients With at Least a
Single Abnormal Connection to the RZ
We sought to investigate whether topological distance to/from RZ related to connection abnor-
mality. We therefore categorized network connections as primary, secondary, tertiary, and
quaternary. For the patients with one or more abnormal connections to/from the RZ zone
(n = 11), none had connections beyond quaternary, meaning that the maximum path length
to/from the resection was four (Figure 2).
Half of patients (11/22) had one or more abnormal primary connections with the RZ as
determined from pre-operative dMRI data. The post-operative MRI is only used to identify
the location of the RZ as a node in the network. In an example patient (Figure 2B), there
were 41 connections direct to the RZ. Of these 41 direct primary connections, 7 (17%) were
abnormal (z < −1.96). There were 482 secondary connections, 16 (3%) of which were
abnormal (z < −1.96). Lastly, there were 409 tertiary connections from the RZ and 4 (1%)
were abnormal (z < −1.96).
The proportion of abnormal connections decreases as topological distance from RZ
increases in 8 out of 11 patients (Figure 2C). We also quantified the relationship between topo-
logical distance from resection and connection abnormality in a non-thresholded approach
Network Neuroscience
6
Epileptogenic networks in extra temporal lobe epilepsy
using a hierarchical statistical model. This model used patient as a random effect, to account
for patient heterogeneity. With connection type defined as above, our hierarchical analysis
(Figure 2D) confirmed significantly greater abnormality in the average primary connection
(mean = −0.97, SE = ±0.24), as compared with secondary (mean = −0.60, SE = ±0.25, p =
.001), tertiary connections (mean = −0.39, SE = ±0.28, p = .002), and quaternary connections
(mean = −0.28, SE = ±0.33, p = .014). These results confirm that the magnitude of connectivity
abnormalities decreases as topological distance from the resection increases.
Abnormalities in Downstream Connections of Nodes Connected to the RZ
We analyzed whether regions connected via an upstream abnormal connection to the RZ
were more likely to have downstream abnormal connections than regions with a normal
upstream connection (Figure 3A). As we were comparing normal and abnormally connected
regions to the RZ, we focused on the 11 patients with at least one or more abnormal primary
RZ connections.
There were more abnormal connections for nodes connected via an upstream abnormal
versus upstream normal connection (t(10) = −4.04, p = .002). This suggests that regions
connected to the RZ via an abnormal connection were more likely to contain abnormal
subsequent connections. This finding also suggests a potential spreading effect of abnormal
connections from the RZ throughout the wider network.
Widespread Abnormalities Are More Common in Patients With Poorer Surgical Outcome
Our final analysis investigated whether the presence of one or more abnormal connections
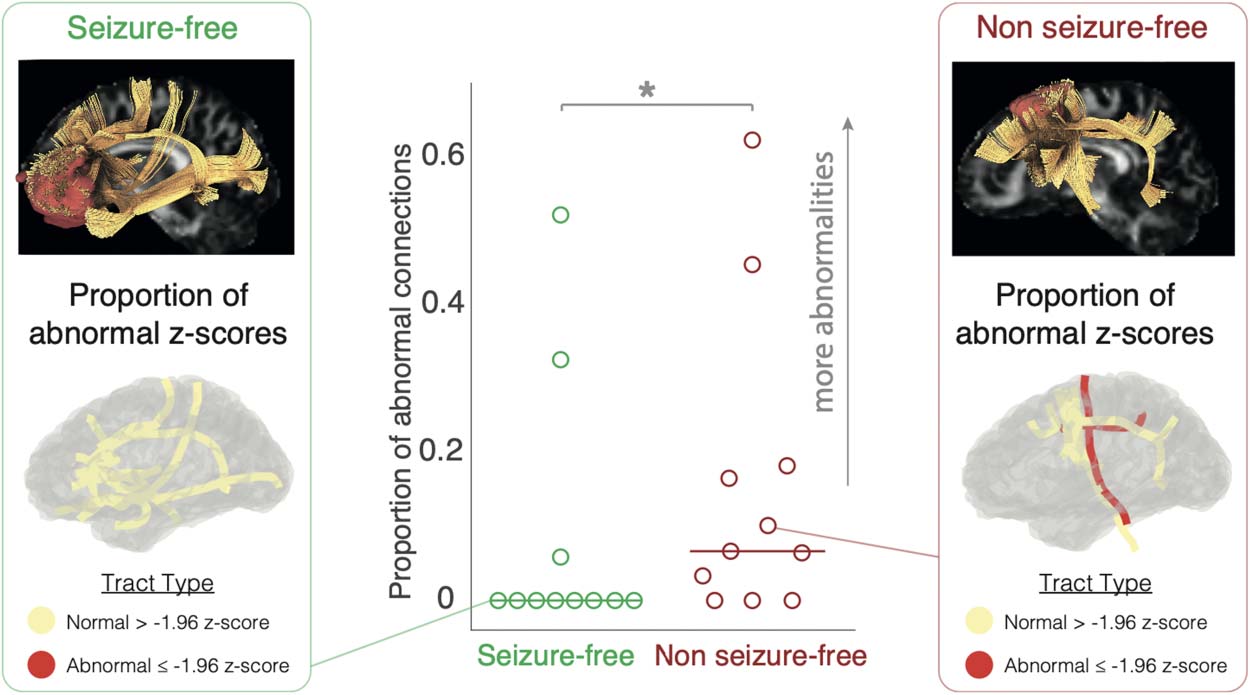
with the RZ prior to surgery was linked to seizure freedom post-surgery. Three of the 11
seizure-free patients had abnormal connections with the RZ (Figure 4, center panel). In con-
trast, 8/11 non-seizure-free patients had abnormal connections to the RZ (X2 = 4.55, p = .033)
(Figure 4).
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
t
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
/
/
.
t
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Figure 3. Nodes connected to the RZ have more abnormalities in downstream connections if the
upstream connection was abnormal. (A) Illustrative example. Nodes are displayed as circles and
lines as connections, abnormal connections and nodes are highlighted in red. A node was defined
as abnormal if its upstream connection to the RZ was abnormal. (B) Results from patients with at
least one abnormal connection with RZ. There was a higher proportion of abnormal connections if
the upstream node had an abnormal connection to the RZ (p < .05, paired t test).
Network Neuroscience
7
Epileptogenic networks in extra temporal lobe epilepsy
Figure 4. Group difference in resection zone connectivity and seizure outcome. A majority of
seizure-free patients did not have a single abnormal connection to/from the RZ (8/11); in contrast,
a majority of non-seizure-free patients had one or more abnormal connections (8/11). An example
patient (left and right panel) from each group is highlighted to illustrate the difference between
groups. The top part of each example displays a sagittal view of the RZ in red, connected tracts
in yellow, and a fractional anisotropy map overlaid on the background. The bottom part illustrates
on a 3D glass brain surface the same example tracts highlighted as either normal (yellow) or abnor-
mal (red). * p < .05.
DISCUSSION
We employed a novel method to compare connectivity of the RZ in a heterogenous cohort of
eTLE patients. There were three main findings: First, in patients with an abnormal connection
at the RZ, the proportion of abnormal connections reduced as topological distance increased
from the RZ. Second, regions with an abnormal connection to the RZ had more abnormal
subsequent connections than did regions without an abnormal RZ connection. Third, patients
with pre-operative abnormal connections with the RZ were less likely to be seizure free after
surgery.
Half of the eTLE group had one or more abnormal connections with the RZ. We hypothe-
sized that if the RZ was a central node in a spreading pathological network, the proportion of
abnormal connections would reduce the further removed connections were from it. Our first
analysis confirmed this hypothesis, showing that proportional reductions were evident in the
number of abnormal connections the further removed connections were from the RZ. This
suggests that if the RZ has at least one or more abnormal connection, it is a potential epicenter
of abnormal connections in the epileptogenic network. These findings concur with studies of
structural and functional connectivity, suggesting the epileptogenic zone can affect large-scale
networks (Hatton et al., 2020; W. Liu, Yue, Gong, Zhou, & Wu, 2021). Similar findings of
widespread network abnormalities have been made in focal epilepsies (Gleichgerrcht et al.,
2021; M. Liu, Concha, Lebel, Beaulieu, & Gross, 2012; Owen et al., 2021; Sinha et al., 2021;
Tsuda et al., 2018).
Abnormal connections were more likely to occur if they connected to regions with abnor-
mal connections to the RZ. This suggests that abnormality reduces the further removed con-
nections are from the RZ and is more likely to connect from prior abnormal connected regions
than from normal connections. With recent findings of widespread abnormal structural net-
works reported in Alzheimer’s (Lee et al., 2022), Huntington’s (Poudel, Harding, Egan, &
Epileptogenic zone (EZ):
Often encompassing the seizure
onset zone, EZ refers to the brain
areas indispensable for the
generation of seizures.
Network Neuroscience
8
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
t
.
/
/
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
.
t
/
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Epileptogenic networks in extra temporal lobe epilepsy
Georgiou-Karistianis, 2019), and Parkinson’s disease (Pandya et al., 2019), it would be inter-
esting to investigate whether a similar abnormal spread is present in other diseases.
The finding that patients with abnormal connectivity at the RZ were less likely to be seizure
free suggests the existence of a distributed epileptogenic network. Previous studies have
similarly found that widespread structural abnormalities in TLE were associated with a poor
seizure outcome also (Bonilha et al., 2015; Sinha et al., 2021). Furthermore, widespread
functional abnormalities were related to outcome in a recent eTLE study using magnetoence-
phalographic data (Owen et al., 2022). Taken together, these findings suggest that more
widespread structural and functional abnormalities beyond the RZ are associated with poorer
post-surgical outcomes.
The findings raise further questions on the nature of abnormality in eTLE networks. First,
longitudinal network studies in eTLE would be useful to elucidate dynamic changes in net-
works, as was recently done in TLE (da Silva et al., 2020; M. Liu et al., 2013). Second, the
relationship between abnormal connectivity between regions, and the pathology of those
regions, is poorly understood. In TLE a relationship has been demonstrated between nodal
atrophy and connectivity abnormality (Horsley et al., 2022); however, this relationship is unex-
plored in eTLE. Third, although most seizure-free patients had no abnormal connections with
the RZ, this does not imply there were no abnormalities within the RZ. It would be useful to
investigate local white matter tracts within RZ (Chen, Wang, Kopetzky, Butz-Ostendorf, &
Kaiser, 2021; Schilling et al., 2022; Shastin et al., 2022). Finally, the postulated epileptogenic
zone defined as the RZ may not represent the true epileptogenic foci. It is possible the abnor-
mal connections predominately associated with the post-operative non-seizure-free patients
could instead represent a more widespread epileptogenic network, and thus the RZ incom-
pletely covers the full epileptogenic zone (EZ). This mechanism of surgical failure, due to
incomplete resection, was recently suggested in another eTLE study (Owen et al., 2023). It
would therefore be interesting to investigate this hypothesis further by analyzing the structural
connectivity in multifocal epilepsy. It would also be worth in future work to analyze the loca-
tion of the RZ, particularly if a certain lobe is more prone to abnormal connectivity. Although
these findings raise further questions on the nature of abnormal networks in eTLE, we note that
the main analysis was conducted on a relatively small sample size, which may impact the
reliability and generalizability of the findings. We therefore encourage replication in larger
samples in future.
Importing the HCP842 tractography atlas (Yeh et al., 2018) helped standardize and provide
accurate white matter connections; furthermore, this technique can be useful in the presence
of pathology that may interrupt tractography (da Silva et al., 2020; Horsley et al., 2022; Sinha
et al., 2021). In addition, using gFA as a measure of connectivity strength, rather than the more
widely used FA, gave a more robust measure of diffusion anisotropy between connections with
complex diffusion profiles, particularly for voxels that contain crossing fibers (Glenn et al.,
2015). Lastly, inferring connections from streamlines that terminate in two regions, rather than
passing through regions, aligns with our hypothesis of connection spread, as each connection
would have nonoverlapping streamlines. This research supports a role for dMRI measures to
detect changes in eTLE and highlights potential network biomarkers that are predictive of
seizure outcome after surgery.
ACKNOWLEDGMENTS
We thank members of the Computational Neurology, Neuroscience, and Psychiatry Lab (https://
www.cnnp-lab.com) for discussions on the analysis and manuscript. We are grateful to the
Network Neuroscience
9
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
/
.
/
t
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
.
/
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Epileptogenic networks in extra temporal lobe epilepsy
Epilepsy Society for supporting the Epilepsy Society MRI scanner. The authors acknowledge
the facilities and scientific and technical assistance of the National Imaging Facility, a National
Collaborative Research Infrastructure Strategy (NCRIS) capability, at the Centre for Micros-
copy, Characterisation, and Analysis, University of Western Australia.
SUPPORTING INFORMATION
Supporting information for this article is available at https://doi.org/10.1162/netn_a_00327.
AUTHOR CONTRIBUTIONS
Gerard R. Hall: Conceptualization; Formal analysis; Investigation; Methodology; Project
administration; Visualization; Writing – original draft; Writing – review & editing. Frances
Hutchings: Formal analysis; Writing – review & editing. Jonathan Horsley: Formal analysis;
Validation; Writing – review & editing. Callum M. Simpson: Formal analysis; Validation; Writing –
review & editing. Yujiang Wang: Conceptualization; Investigation; Validation; Writing – review
& editing. Jane de Tisi: Data curation. Anna Miserocchi: Data curation; Writing – review &
editing. Andrew W. McEvoy: Data curation; Writing – review & editing. Sjoerd B. Vos: Data
curation; Writing – review & editing. Gavin P. Winston: Data curation; Writing – original draft.
John S. Duncan: Data curation; Writing – review & editing. Peter N. Taylor: Conceptualiza-
tion; Data curation; Funding acquisition; Methodology; Project administration; Resources;
Supervision; Validation; Visualization; Writing – review & editing.
FUNDING INFORMATION
Peter N. Taylor, UK Research and Innovation (https://dx.doi.org/10.13039/100014013), Award
ID: MR/T04294X/1. Yujiang Wang, UK Research and Innovation (https://dx.doi.org/10.13039
/100014013), Award ID: MR/ V026569/1. Gavin P. Winston, Medical Research Charities
Group (https://dx.doi.org/10.13039/100012891), Award ID: G0802012. Gavin P. Winston,
Medical Research Charities Group (https://dx.doi.org/10.13039/100012891), Award ID:
MR/M00841X/1. Sjoerd B. Vos, NCRIS. Jane de Tisi, National Institute for Health and Care
Research (https://dx.doi.org/10.13039/501100000272). Anna Miserocchi, National Institute
for Health and Care Research (https://dx.doi.org/10.13039/501100000272). Andrew W.
McEvoy, National Institute for Health and Care Research (https://dx.doi.org/10.13039
/501100000272). Gavin P. Winston, National Institute for Health and Care Research (https://
dx.doi.org/10.13039/501100000272). John S. Duncan, National Institute for Health and Care
Research (https://dx.doi.org/10.13039/501100000272). Callum M. Simpson, EPSRC. Jonathan
Horsley, EPSRC.
REFERENCES
Ashraf-Ganjouei, A., Rahmani, F., Aarabi, M. H., Sanjari
Moghaddam, H., Nazem-Zadeh, M. R., Davoodi-Bojd, E., &
Soltanian-Zadeh, H. (2019). White matter correlates of disease
duration in patients with temporal lobe epilepsy: Updated review
of literature. Neurological Sciences, 40(6), 1209–1216. https://
doi.org/10.1007/s10072-019-03818-2, PubMed: 30868482
Bonilha, L., Jensen, J. H., Baker, N., Breedlove, J., Nesland, T., Lin,
J. J., … Kuzniecky, R. I. (2015). The brain connectome as a per-
sonalized biomarker of seizure outcomes after temporal lobec-
tomy. Neurology, 84(18), 1846–1853. https://doi.org/10.1212
/ WNL.0000000000001548, PubMed: 25854868
Bonilha, L., Rorden, C., Appenzeller, S., Coan, A. C., Cendes, F., &
Li, L. M. (2006). Gray matter atrophy associated with duration of
temporal lobe epilepsy. NeuroImage, 32(3), 1070–1079. https://
doi.org/10.1016/j.neuroimage.2006.05.038, PubMed: 16872843
Carboni, M., De Stefano, P., Vorderwülbecke, B. J., Tourbier, S.,
Mullier, E., Rubega, M., … Vulliemoz, S. (2020). Abnormal
directed connectivity of resting state networks in focal epilepsy.
NeuroImage: Clinical, 27, 102336. https://doi.org/10.1016/j.nicl
.2020.102336, PubMed: 32679553
Chen, X., Wang, Y., Kopetzky, S. J., Butz-Ostendorf, M., & Kaiser,
M. (2021). Connectivity within regions characterizes epilepsy
Network Neuroscience
10
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
/
t
/
.
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
/
.
t
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Epileptogenic networks in extra temporal lobe epilepsy
duration and treatment outcome. Human Brain Mapping, 42(12),
3777–3791. https://doi.org/10.1002/ hbm.25464, PubMed:
33973688
Chiang, S., Levin, H. S., Wilde, E., & Haneef, Z. (2016). White
matter structural connectivity changes correlate with epilepsy
duration in temporal lobe epilepsy. Epilepsy Research, 120,
37–46. https://doi.org/10.1016/j.eplepsyres.2015.12.002,
PubMed: 26709881
Chowdhury, F. A., Silva, R., Whatley, B., & Walker, M. C. (2021).
Localisation in focal epilepsy: A practical guide. Practical Neu-
rology, 21(6), 481–491. https://doi.org/10.1136/practneurol-2019
-002341, PubMed: 34404748
da Silva, N. M., Forsyth, R., McEvoy, A., Miserocchi, A., de Tisi, J.,
Vos, S. B., … Taylor, P. N. (2020). Network reorganisation follow-
ing anterior temporal lobe resection and relation with
post-surgery seizure relapse: A longitudinal study. NeuroImage:
Clinical, 27, 102320. https://doi.org/10.1016/j.nicl.2020
.102320, PubMed: 32623138
Delev, D., Oehl, B., Steinhoff, B. J., Nakagawa, J., Scheiwe, C.,
Schulze-Bonhage, A., & Zentner, J. (2019). Surgical treatment
of extratemporal epilepsy: Results and prognostic factors. Neuro-
surgery, 84(1), 242–252. https://doi.org/10.1093/neuros/nyy099,
PubMed: 29618099
Englot, D. J., Konrad, P. E., & Morgan, V. L. (2016). Regional and global
connectivity disturbances in focal epilepsy, related neurocognitive
sequelae, and potential mechanistic underpinnings. Epilepsia,
57(10), 1546–1557. Retrieved from https://onlinelibrary.wiley
.com/doi/pdfdirect/10.1111/epi.13510?download=true. https://doi
.org/10.1111/epi.13510, PubMed: 27554793
Fischl, B. (2012). FreeSurfer. NeuroImage, 62(2), 774–781. https://
doi.org/10.1016/j.neuroimage.2012.01.021, PubMed: 22248573
Fisher, R. S., Acevedo, C., Arzimanoglou, A., Bogacz, A., Cross,
J. H., Elger, C. E., … Glynn, M. (2014). ILAE official report: A
practical clinical definition of epilepsy. Epilepsia, 55(4),
475–482. Retrieved from https://onlinelibrary.wiley.com/doi
/pdfdirect/10.1111/epi.12550?download=true. https://doi.org/10
.1111/epi.12550, PubMed: 24730690
Giampiccolo, D., Binding, L. P., Caciagli, L., Rodionov, R., Foulon,
C., de Tisi, J., … Miserocchi, A. (2023). Thalamostriatal discon-
nection underpins long-term seizure freedom in frontal lobe epi-
lepsy surgery. Brain, 146(6), 2377–2388. https://doi.org/10.1093
/brain/awad085, PubMed: 37062539
Gleichgerrcht, E., Greenblatt, A. S., Kellermann, T. S., Rowland, N.,
Vandergrift, W. A., Edwards, J., … Bonilha, L. (2021). Patterns of
seizure spread in temporal lobe epilepsy are associated with dis-
tinct white matter tracts. Epilepsy Research, 171, 106571. https://
doi.org/10.1016/j.eplepsyres.2021.106571, PubMed: 33582534
Glenn, G. R., Helpern, J. A., Tabesh, A., & Jensen, J. H. (2015).
Quantitative assessment of diffusional kurtosis anisotropy. NMR
in Biomedicine, 28(4), 448–459. https://doi.org/10.1002/nbm
.3271, PubMed: 25728763
Hagmann, P., Cammoun, L., Gigandet, X., Meuli, R., Honey, C. J.,
Wedeen, V. J., & Sporns, O. (2008). Mapping the structural core
of human cerebral cortex. PLOS Biology, 6(7), e159. https://doi
.org/10.1371/journal.pbio.0060159, PubMed: 18597554
Hatton, S. N., Huynh, K. H., Bonilha, L., Abela, E., Alhusaini, S.,
Altmann, A., … McDonald, C. R. (2020). White matter
abnormalities across different epilepsy syndromes in adults: An
ENIGMA-Epilepsy study. Brain, 143(8), 2454–2473. https://doi
.org/10.1093/brain/awaa200, PubMed: 32814957
Hong, S.-J., Bernhardt, B. C., Schrader, D. S., Bernasconi, N., &
Bernasconi, A. (2016). Whole-brain MRI phenotyping in
dysplasia-related frontal lobe epilepsy. Neurology, 86(7),
643–650. https://doi.org/10.1212/wnl.0000000000002374,
PubMed: 26764030
Hong, S.-J., Lee, H.-M., Gill, R., Crane, J., Sziklas, V., Bernhardt,
B. C., … Bernasconi, A. (2019). A connectome-based mechanis-
tic model of focal cortical dysplasia. Brain, 142(3), 688–699.
https://doi.org/10.1093/brain/awz009, PubMed: 30726864
Horsley, J. J., Schroeder, G. M., Thomas, R. H., de Tisi, J., Vos, S. B.,
Winston, G. P., … Taylor, P. N. (2022). Volumetric and structural
connectivity abnormalities co-localise in TLE. NeuroImage: Clin-
ical, 35, 103105. https://doi.org/10.1016/j.nicl.2022.103105,
PubMed: 35863179
Jenkinson, M., Bannister, P., Brady, M., & Smith, S. (2002).
Improved optimization for the robust and accurate linear registra-
tion and motion correction of brain images. NeuroImage, 17(2),
825–841. https://doi.org/10.1016/s1053-8119(02)91132-8,
PubMed: 12377157
Jenkinson, M., Beckmann, C. F., Behrens, T. E., Woolrich, M. W., &
Smith, S. M. (2012). FSL. NeuroImage, 62(2), 782–790. https://
doi.org/10.1016/j.neuroimage.2011.09.015, PubMed: 21979382
Jenkinson, M., & Smith, S. (2001). A global optimisation method
for robust affine registration of brain images. Medical Image
Analysis, 5(2), 143–156. https://doi.org/10.1016/s1361
-8415(01)00036-6, PubMed: 11516708
Kini, L. G., Bernabei, J. M., Mikhail, F., Hadar, P., Shah, P.,
Khambhati, A. N., … Litt, B. (2019). Virtual resection predicts
surgical outcome for drug-resistant epilepsy. Brain, 142(12),
3892–3905. https://doi.org/10.1093/ brain/awz303, PubMed:
31599323
Kreilkamp, B. A., Weber, B., Richardson, M. P., & Keller, S. S.
(2017). Automated tractography in patients with temporal lobe
epilepsy using TRActs Constrained by UnderLying Anatomy
(TRACULA). NeuroImage: Clinical, 14, 67–76. https://doi.org/10
.1016/j.nicl.2017.01.003, PubMed: 28138428
Lee, W. J., Brown, J. A., Kim, H. R., La Joie, R., Cho, H., Lyoo,
C. H., … Alzheimer’s Disease Neuroimaging Initiative. (2022).
Regional Aβ-tau interactions promote onset and acceleration of
Alzheimer’s disease tau spreading. Neuron, 110(12), 1932–1943
e1935. https://doi.org/10.1016/j.neuron.2022.03.034, PubMed:
35443153
Liu, M., Concha, L., Lebel, C., Beaulieu, C., & Gross, D. W. (2012).
Mesial temporal sclerosis is linked with more widespread white
matter changes in temporal lobe epilepsy. NeuroImage: Clinical,
1(1), 99–105. https://doi.org/10.1016/j.nicl.2012.09.010,
PubMed: 24179742
Liu, M., Gross, D. W., Wheatley, B. M., Concha, L., & Beaulieu, C.
(2013). The acute phase of Wallerian degeneration: Longitudinal
diffusion tensor imaging of the fornix following temporal lobe
surgery. NeuroImage, 74, 128–139. https://doi.org/10.1016/j
.neuroimage.2013.01.069, PubMed: 23396161
Liu, W., Yue, Q., Gong, Q., Zhou, D., & Wu, X. (2021). Regional
and remote connectivity patterns in focal extratemporal lobe
Network Neuroscience
11
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
/
/
t
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
.
/
/
t
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
/
t
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3
Q1
Epileptogenic networks in extra temporal lobe epilepsy
epilepsy. Annals of Translational Medicine, 9(14), 1128. https://
doi.org/10.21037/atm-21-1374, PubMed: 34430569
Munsell, B. C., Wee, C. Y., Keller, S. S., Weber, B., Elger, C., da
Silva, L. A., … Bonilha, L. (2015). Evaluation of machine learning
algorithms for treatment outcome prediction in patients with epi-
lepsy based on structural connectome data. NeuroImage, 118,
219–230. https://doi.org/10.1016/j.neuroimage.2015.06.008,
PubMed: 26054876
Owen, T. W., Schroeder, G. M., Janiukstyte, V., Hall, G. R.,
McEvoy, A., Miserocchi, A., … Taylor, P. N. (2022). MEG abnor-
malities highlight mechanisms of surgical failure in neocortical
epilepsy. arXiv:2207.06518. https://doi.org/10.1111/epi.17503,
PubMed: 36617392
Owen, T. W., Schroeder, G. M., Janiukstyte, V., Hall, G. R.,
McEvoy, A., Miserocchi, A., … Taylor, P. N. (2023). MEG abnor-
malities and mechanisms of surgical failure in neocortical epi-
lepsy. Epilepsia, 64(3), 692–704. https://doi.org/10.1111/epi
.17503, PubMed: 36617392
Owen, T. W., Tisi, J., Vos, S. B., Winston, G. P., Duncan, J. S., Wang,
Y., & Taylor, P. N. (2021). Multivariate white matter alterations
are associated with epilepsy duration. European Journal of Neu-
roscience, 53(8), 2788–2803. https://doi.org/10.1111/ejn.15055,
PubMed: 33222308
Pandya, S., Zeighami, Y., Freeze, B., Dadar, M., Collins, D. L.,
Dagher, A., & Raj, A. (2019). Predictive model of spread of
Parkinson’s pathology using network diffusion. NeuroImage,
192, 178–194. https://doi.org/10.1016/j.neuroimage.2019.03
.001, PubMed: 30851444
Poudel, G. R., Harding, I. H., Egan, G. F., & Georgiou-Karistianis,
N. (2019). Network spread determines severity of degeneration
and disconnection in Huntington’s disease. Human Brain Map-
ping, 40(14), 4192–4201. https://doi.org/10.1002/ hbm.24695,
PubMed: 31187915
Ridley, B. G., Rousseau, C., Wirsich, J., Le Troter, A., Soulier, E.,
Confort-Gouny, S., … Guye, M. (2015). Nodal approach reveals
differential impact of lateralized focal epilepsies on hub reorga-
nization. NeuroImage, 118, 39–48. https://doi.org/10.1016/j
.neuroimage.2015.05.096, PubMed: 26070261
Schilling, K., Archer, D. B., Rheault, F., Lyu, I., Huo, Y., Cai, L. Y., …
Anderson, A. W. (2022). Superficial white matter across the life-
span: Volume, thickness, change, and relationship with cortical
features. bioRxiv. https://doi.org/10.1101/2022.07.20.500818,
PubMed: 35018374
Shastin, D., Genc, S., Parker, G. D., Koller, K., Tax, C. M., Evans, J.,
… Chamberland, M. (2022). Surface-based tracking for short
association fibre tractography. NeuroImage, 260, 119423.
https://doi.org/10.1016/j.neuroimage.2022.119423, PubMed:
35809886
Sinha, N., Wang, Y., Moreira da Silva, N., Miserocchi, A., McEvoy,
A. W., de Tisi, J., … Taylor, P. N. (2021). Structural brain network
abnormalities and the probability of seizure recurrence after
epilepsy surgery. Neurology, 96(5), e758–e771. https://doi.org
/10.1212/ WNL.0000000000011315, PubMed: 33361262
Slinger, G., Sinke, M. R., Braun, K. P., & Otte, W. M. (2016). White
matter abnormalities at a regional and voxel level in focal and
generalized epilepsy: A systematic review and meta-analysis.
NeuroImage: Clinical, 12, 902–909. https://doi.org/10.1016/j
.nicl.2016.10.025, PubMed: 27882296
Tavakol, S., Royer, J., Lowe, A. J., Bonilha, L., Tracy, J. I., Jackson,
G. D., … Bernhardt, B. C. (2019). Neuroimaging and connec-
tomics of drug-resistant epilepsy at multiple scales: From focal
lesions to macroscale networks. Epilepsia, 60(4), 593–604.
https://doi.org/10.1111/epi.14688, PubMed: 30889276
Taylor, P. N., Sinha, N., Wang, Y., Vos, S. B., de Tisi, J., Miserocchi,
A., … Duncan, J. S. (2018). The impact of epilepsy surgery on the
structural connectome and its relation to outcome. NeuroImage:
Clinical, 18, 202–214. https://doi.org/10.1016/j.nicl.2018.01
.028, PubMed: 29876245
Tellez-Zenteno, J. F., & Hernandez-Ronquillo, L. (2012). A review
of the epidemiology of temporal lobe epilepsy. Epilepsy Research
and Treatment, 2012, 630853. https://doi.org/10.1155/2012
/630853, PubMed: 22957234
Tsuda, K., Tsuji, T., Ishida, T., Takahashi, S., Yamada, S., Ohoshi, Y.,
… Ukai, S. (2018). Widespread abnormalities in white matter
integrity and their relationship with duration of illness in tempo-
ral lobe epilepsy. Epilepsia Open, 3(2), 247–254. https://doi.org
/10.1002/epi4.12222, PubMed: 29881803
Vos, S. B., Tax, C. M., Luijten, P. R., Ourselin, S., Leemans, A., &
Froeling, M. (2017). The importance of correcting for signal drift in
diffusion MRI. Magnetic Resonance in Medicine, 77(1), 285–299.
https://doi.org/10.1002/mrm.26124, PubMed: 26822700
Wagstyl, K., Whitaker, K., Raznahan, A., Seidlitz, J., Vértes, P. E.,
Foldes, S., … Adler, S. (2022). Atlas of lesion locations and post-
surgical seizure freedom in focal cortical dysplasia: A MELD
study. Epilepsia, 63(1), 61–74. https://doi.org/10.1111/epi
.17130, PubMed: 34845719
Wieser, H. G., Blume, W. T., Fish, D., Goldensohn, E., Hufnagel, A.,
King, D., … Commission on Neurosurgery of the International
League Against Eilepsy. (2001). ILAE Commission Report. Proposal
for a new classification of outcome with respect to epileptic seizures
following epilepsy surgery. Epilepsia, 42(2), 282–286. Retrieved
from https://www.ncbi.nlm.nih.gov/pubmed/11240604. https://doi
.org/10.1046/j.1528-1157.2001.35100.x, PubMed: 11240604
Yeh, F. C., Panesar, S., Fernandes, D., Meola, A., Yoshino, M.,
Fernandez-Miranda, J. C., … Verstynen, T. (2018). Population-
averaged atlas of the macroscale human structural connectome
and its network topology. NeuroImage, 178, 57–68. https://doi
.org/10.1016/j.neuroimage.2018.05.027, PubMed: 29758339
Yeh, F. C., & Tseng, W. Y. (2011). NTU-90: A high angular resolu-
tion brain atlas constructed by q-space diffeomorphic reconstruc-
tion. NeuroImage, 58(1), 91–99. https://doi.org/10.1016/j
.neuroimage.2011.06.021, PubMed: 21704171
Network Neuroscience
12
l
D
o
w
n
o
a
d
e
d
f
r
o
m
h
t
t
p
:
/
/
d
i
r
e
c
t
.
m
i
t
.
t
/
/
e
d
u
n
e
n
a
r
t
i
c
e
-
p
d
l
f
/
d
o
i
/
/
.
t
/
1
0
1
1
6
2
n
e
n
_
a
_
0
0
3
2
7
2
1
5
2
8
3
1
n
e
n
_
a
_
0
0
3
2
7
p
d
t
/
.
f
b
y
g
u
e
s
t
t
o
n
0
7
S
e
p
e
m
b
e
r
2
0
2
3