The Blame Game: The Effect of Responsibility
and Social Stigma on Empathy for Pain
Jean Decety, Stephanie Echols, and Joshua Correll
Abstracto
■ This investigation combined behavioral and functional neuro-
imaging measures to explore whether perception of pain is
modulated by the targetʼs stigmatized status and whether the
target bore responsibility for that stigma. During fMRI scanning,
participants were exposed to a series of short video clips featuring
age-matched individuals experiencing pain who were (a) similar
to the participant (saludable), (b) stigmatized but not responsible
for their stigmatized condition (infected with AIDS as a result of
an infected blood transfusion), o (C) stigmatized and responsible
for their stigmatized condition (infected with AIDS as a result of
intravenous drug use). Explicit pain and empathy ratings for the
targets were obtained outside of the MRI environment, a lo largo de
with a variety of implicit and explicit measures of AIDS bias. Re-
sults showed that participants were significantly more sensi-
tive to the pain of AIDS transfusion targets as compared with
healthy and AIDS drug targets, as evidenced by significantly higher
pain and empathy ratings during video evaluation and significantly
greater hemodynamic activity in areas associated with pain pro-
cesando (es decir., right anterior insula, anterior midcingulate cortex,
periaqueductal gray). A diferencia de, significantly less activity was ob-
served in the anterior midcingulate cortex for AIDS drug targets
as compared with healthy controls. Más, behavioral differ-
ences between healthy and AIDS drug targets were moderated
by the extent to which participants blamed AIDS drug individuals
for their condition. Controlling for both explicit and implicit
AIDS bias, the more participants blamed these targets, the less
pain they attributed to them as compared with healthy controls.
The present study reveals that empathic resonance is moderated
early in information processing by a priori attitudes toward the
target group. ■
INTRODUCCIÓN
When we witness another individual in pain, do we wince
automáticamente? Or are we more likely to wait to respond
until we determine the cause of the pain, the context of
the situation, or the background of the individual?
The psychological construct of empathy refers to an
intersubjective induction process through which the cog-
nitive and affective experiences of another come to be
shared, without losing sight of the original source of the
experiencia (Decety & Jackson, 2004). In light of multiple
levels of analysis from social and developmental psychol-
ogia, cognitive neuroscience, and clinical neuropsychol-
ogia, it has been proposed that empathy involves both
bottom–up and top–down information processing compo-
nents (Goubert, Craig, & Buysse, 2009; Decety & Moriguchi,
2007). The former refers to the automatic and covert mim-
icry component, which drives emotional contagion during
interpersonal interactions, and the latter to self-regulation
and meta-cognition, which modulates both this automatic
resonance system and subsequent prosocial behaviors.
As the first-hand experience of pain is ubiquitous across
individuals and cultures and there is extensive knowledge
about the physiological mechanisms underlying the pro-
The University of Chicago
cessing of nociceptive information, studying the perception
of pain in others constitutes a valuable and ecologically
valid paradigm for investigating the underpinning of hu-
man empathy.
En años recientes, an accumulating number of fMRI stud-
ies have demonstrated striking similarities in the neural
circuits involved in the processing of both the first-hand
experience of pain and the second-hand experience of
observing other individuals in pain (for a meta-analysis,
see Jackson, Rainville, & Decety, 2006). These studies
have consistently shown that the perception of pain in
others elicits activation of the neural circuit subserving
the processing of the affective and motivational dimen-
sion of pain (Cheng et al., 2007; Gu & Han, 2007; Lamm,
Batson, & Decety, 2007; Moriguchi et al., 2007; Ogino
et al., 2007; Saarela et al., 2007; Zaki, Ochsner, Hanelin,
Apostar, & Mackey, 2007; Jackson, Brunet, Meltzoff, &
Decety, 2006; Botvinick et al., 2005; Jackson, Meltzoff, &
Decety, 2005; Morrison, lloyd, di Pellegrino, & Roberts,
2004; Singer et al., 2004). This neural circuit includes the
dorsal ACC (dACC), the anterior midcingulate cortex
(aMCC), and the anterior insula (AI; Derbyshire, 2000).
The findings from these recent cognitive neuroscience
investigations provide empirical support for observer–
target congruence in pain processing similar to that which
social psychologists have reported for the past 30 años.
Por ejemplo, Hygge (1976) found that when an observer
© 2009 Instituto de Tecnología de Massachusetts
Revista de neurociencia cognitiva 22:5, páginas. 985–997
D
oh
w
norte
yo
oh
a
d
mi
d
yo
yo
/
/
/
/
j
t
t
F
/
i
t
.
:
/
/
F
r
oh
metro
D
h
oh
t
w
t
norte
pag
oh
:
a
/
d
/
mi
metro
d
i
F
t
r
oh
pag
metro
r
C
h
.
s
pag
i
yo
d
v
i
mi
r
mi
r
C
C
t
.
h
metro
a
i
r
mi
.
d
tu
C
oh
oh
metro
C
/
norte
j
a
oh
r
C
t
i
norte
C
/
mi
a
–
pag
r
d
t
i
2
C
2
yo
5
mi
–
9
pag
8
d
5
F
1
/
9
2
3
2
9
/
1
5
5
/
9
9
oh
8
C
5
norte
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
oh
pag
C
d
norte
.
b
2
y
0
gramo
0
tu
9
mi
.
s
t
2
oh
1
norte
2
6
0
6
7
.
S
pag
mi
d
pag
F
mi
metro
b
y
b
mi
gramo
r
tu
2
mi
0
2
s
3
t
/
j
t
.
F
.
/
.
oh
norte
1
8
METRO
a
y
2
0
2
1
witnessed a targetʼs distress, they experienced an increase
in skin conductance similar to the arousal response elicited
by the aversive stimulation itself, demonstrating that ob-
servers are autonomically aroused by a targetʼs distress.
Más, Vaughan and Lanzetta (1980) demonstrated that
observers respond to a targetʼs pain display with similar
expressive behavior. Using EMG recordings from three
facial muscle sites, these authors found that the pattern
and timing of activation of the observerʼs facial muscles
paralleled those of the target expressing pain.
With the abovementioned neuroimaging and physio-
logical findings, there is strong evidence to suggest that
perceiving the pain of others triggers an automatic somatic
sensory-motor resonance mechanism between other and
self, resulting in pain processing in the observer. This shar-
ing of neural circuits between self (observer) and other
(objetivo) provides the foundation for analogical reasoning
and offers a possible, yet partial, route to understanding
otros (Decety & Grèzes, 2006).
Although the neuroscience research in somatic sensory
mimicry provides evidence for a universal neurological
mechanism underlying empathy, it does not address the
effect of a host of social factors that might influence such
an empathic response. Por ejemplo, recent work in social
cognition has shown that both bottom–up and top–down
mechanisms of empathy can be modulated by how the
target is perceived, including how similar the target is to
the observer (es decir., Ames, 2004; Batson et al., 1997), cómo
likable the target is (es decir., Kozak, Marsh, & Wegner, 2006;
Singer et al., 2006), and the group membership of the
objetivo (es decir., Stürmer, Snyder, Kropp, & Siem, 2006; Yabar,
Johnston, Miles, & Peace, 2006). Understanding how such
factors impact the ability to perceive and to respond with
care to the cognitive, affective, and motivational internal
states of another is crucial to understanding the conditions
in which empathy will be expressed (Decety & Batson,
2007).
One way to more fully elucidate how a priori attitudes
may moderate empathy for pain is to explore the effect of
social stigma on the empathic response. Stigmatization of
an individual occurs when that individual is (1) labeled,
(2) negatively stereotyped, (3) discriminated against,
y (4) experiences status loss as a result of their stigma
(Link & Phelan, 2001). Stigmatized individuals possess or
are believed to possess some attribute or characteristic
that conveys a social identity that is devalued in a partic-
ular context (Crocker, Major, & Steele, 1998). Como resultado
of such a devalued and dehumanized out-group status, él
can be predicted that someone would experience less
empathy for an individual who is stigmatized.
A particularly illustrative example of a group of people
who are stigmatized by society is those infected with HIV
or who currently have AIDS. A number of empirical in-
vestigations have documented both explicit and im-
plicit negative attitudes toward people with HIV/AIDS
(para una revisión, see Herek, 1999). Por ejemplo, Neumann,
Hulsenbeck, and Seibt (2004) measured participantʼs
implicit attitudes toward people with AIDS (PWA) usando
both an implicit association test (IAT) and an automatic
approach/avoidance task. Participants demonstrated
a significant and negative implicit association for PWA
and were significantly faster at making avoidance move-
ments than approach movements in response to pictures
of PWA.
Además, attributions of responsibility can modulate
an observerʼs emotional response toward such stigmatized
objetivos. If targets are deemed responsible for their condi-
ción, they are judged with anger and blame and are stig-
matized and socially rejected. Alternately, if targets are not
considered responsible for their condition, they are judged
with relative sympathy and social acceptance (Crandall
& Martinez, 1996). En particular, attributions of respon-
sibility have been shown to moderate attitudes toward
individuals infected with AIDS: participants are less likely
to show compassion for individuals who contracted HIV
through stigmatized behavior (es decir., drug use) than for
people who were infected through other means, como
a blood transfusion (Capitanio & Herek, 1999; Weiner,
Perry, & Magnusson, 1988).
The abovementioned research demonstrates not only
that people infected with HIV/AIDS are negatively viewed
and stigmatized in society but also that attributions of re-
sponsibility for how PWA contracted the disease influences
how they are perceived. Applying this research on stigma-
tized out-groups (such as PWA) to the literature on the
somatic sensory mimicry components of empathy, es
hypothesized that resonance to stigmatized targets will
be moderated by attributions of responsibility.
To investigate this hypothesis, the current study exam-
ined whether the hemodynamic response in the neural
circuits underlying pain processing was modulated by the
stigma of the target and whether the target bore responsi-
bility for his or her stigmatized status. During fMRI scan-
y, white participants were exposed to a series of
short video clips featuring age-matched white individ-
uals experiencing pain who were (a) similar to the par-
ticipant (saludable), (b) stigmatized but not responsible for
their stigmatized condition (infected with AIDS as a result
of an infected blood transfusion from a recent hospital
stay), o (C) stigmatized and held responsible for their
stigmatized condition (infected with AIDS as a result of
intravenous drug use). We predicted that although partici-
pants should show resonance to the pain of all targets
(regardless of group membership), resonance should de-
pend on the targetʼs stigma and his or her responsibility
for acquiring that stigma. Tal como, we predicted reduced
hemodynamic activation in pain processing areas when
viewing stigmatized targets in general as compared with
control targets similar to the participants. Sin embargo, nosotros
predicted that attributions of responsibility would mod-
erate this effect, such that significantly greater hemo-
dynamic activation in pain processing areas would be
observed when viewing not-responsible stigmatized tar-
gets and significantly less activity would be observed for
986
Revista de neurociencia cognitiva
Volumen 22, Número 5
D
oh
w
norte
yo
oh
a
d
mi
d
yo
yo
/
/
/
/
j
t
t
F
/
i
t
.
:
/
/
F
r
oh
metro
D
h
oh
t
w
t
norte
pag
oh
:
a
/
d
/
mi
metro
d
i
F
t
r
oh
pag
metro
r
C
h
.
s
pag
i
yo
d
v
i
mi
r
mi
r
C
C
t
.
h
metro
a
i
r
mi
.
d
tu
C
oh
oh
metro
C
/
norte
j
a
oh
r
C
t
i
norte
C
/
mi
a
–
pag
r
d
t
i
2
C
2
yo
5
mi
–
9
pag
8
d
5
F
1
/
9
2
3
2
9
/
1
5
5
/
9
9
oh
8
C
5
norte
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
oh
pag
C
d
norte
.
b
2
y
0
gramo
0
tu
9
mi
.
s
t
2
oh
1
norte
2
6
0
6
7
.
S
pag
mi
d
pag
F
mi
metro
b
y
b
mi
gramo
r
tu
2
mi
0
2
s
3
t
/
j
.
F
.
.
t
/
oh
norte
1
8
METRO
a
y
2
0
2
1
responsible stigmatized targets. The results of this investi-
gation have important societal significance and will yield a
better understanding of the mechanisms involved in inter-
personal sensitivity and the factors that influence this
capacidad.
MÉTODOS
Participantes
Twenty-six white participants completed the full testing
procedure approved by the Behavioral Sciences Division
Institutional Review Board at the University of Chicago.
Sin embargo, due to magnet-related artifacts in the fMRI
datos, 4 subjects were dropped from all subsequent anal-
yses, resulting in sample of 22 participantes sanos (11
hombres; edad media = 25.2 ± 5.05 años). All subjects were
right-handed and had no prior history of major neuro-
logical, medical, or psychiatric disorders. Además,
all subjects did not personally know anyone with HIV/AIDS
and did not personally know anyone who used intravenous
drogas (currently or in the past). Each participant gave in-
formed consent and was paid for their participation in
este estudio.
Materials
A detailed description of the video stimuli used in this ex-
perimento, as well as the video collection and validation pro-
cedures, can be found in Lamm et al. (2007). Each video
depicted a white individual wearing a white medical
blouse and headphones and sitting in front of a light blue
background curtain. The purpose of this setting was to
imply the hospital environment outlined in the study de-
scription (abajo). To obtain video clips of facial expres-
sions of pain, we videotaped 24 male and female targets
(12 hombres) while they listened to painful, dissonant tone
pares. For the duration of the tone, the individual in the
video portrayed an expression of genuine pain. Video clips
eran 3.5 sec in duration, showing the transition from a
neutral (0.5 segundo) to a pained (3 segundo) facial expression. Video
clips showed a natural pain response in which targets
displayed brow lowering, orbit tightening, and either
cursing/pressing of the lips or opening/stretching of the
mouth. These movements have consistently been attrib-
uted to the facial expression of pain (p.ej., Craig, Prkachin,
& Grunau, 2001). Two clips meeting these criteria were
selected for each target, yielding 48 dynamic video stimuli
of male and female targets expressing pain.
Experimental Procedure
fMRI Data Collection
Using standardized written and verbal instructions, partícipe-
ipants were informed that they would view short video
clips of individuals expressing pain. Participants were told
that all of the individuals in the clips suffer from a middle
ear disorder called tinnitus aurium, which results in a
painful and an unpleasant ringing sound in the ears. Ellos
were told that the individuals acquired the tinnitus aurium
as a complication from a virus that they acquired either
by chance when they were healthy or as a complication
from having HIV/AIDS. Además, participants were
told that these patients contracted HIV as a result of either
(a) an infected blood transfusion or (b) sharing infected
needles used during illegal intravenous drug use. Participe-
pants were informed that they would watch short video
clips of these three groups of individuals listening to un-
pleasant sounds as part of their treatment therapy, and as
semejante, the individuals would be experiencing moderate to
strong pain.
Stimuli were presented via E-Prime software (Psicología
Software Tools, Cª, pittsburgh, Pensilvania) in a mixed-block/
event-related format, with group membership ( saludable,
AIDS transfusion, and AIDS drug) blocked to minimize
task-switching demands. Each block consisted of four
ensayos, with each trial as follows: primero, participants saw a
word cue (“healthy,” “AIDS transfusion,” or “AIDS drug”)
para 1.5 sec to indicate which group the subsequent individ-
ual in the video belonged to. This word cue was followed
by a jittered fixation cross. Próximo, participants viewed a
3.5-sec video clip of the individual in pain. To complete
the trial, participants viewed a second jittered fixation
cross. Both within-trial fixation durations were randomly
jittered (range: 2–5 sec) to prevent stimulus predictability
and to allow independent event-related signal estima-
tion for both the cue and the video clip (Donaldson &
Buckner, 2001). Each block was separated by a fixed 6-sec
interblock interval.
In each group, two different video clips of eight (four
masculino) individuals were shown, Resultando en 16 clips per con-
condición. Each video clip was repeated once; de este modo, participar-
pants viewed 96 video clips in total with 32 trials per
condición. Average pain ratings within condition were
equivalent across the three group conditions (F < 1; SD:
F < 1; ratings based on pretested data; see Lamm et al.,
2007). The assignment of the target individuals to their
group was counterbalanced across participants. This
resulted in three different versions of the experimental
procedure that were pseudorandomly assigned such that
a third of the participants each viewed eight different target
individuals in each of the three groups.
Four consecutive fMRI runs were performed, with
each run consisting of six blocks of four trials each. The
order of the blocks was pseudorandomized so that no
more than two blocks for each condition appeared per
run, and eight blocks per condition were displayed in total.
Before and during the rest period between runs, partici-
pants were verbally instructed to closely attend to each
video clip and were informed that they would be asked
questions about these individuals after the fMRI scanning
session.
Decety, Echols, and Correll
987
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
/
t
.
.
.
f
o
n
1
8
M
a
y
2
0
2
1
Explicit Behavioral Measures
Following fMRI scanning, participants completed a behav-
ioral task using E-Prime (Psychology Software Tools, Inc.)
presentation software. In this task, participants repeated
the viewing procedure previously shown in the fMRI scan-
ner. However, participants were asked to respond to three
questions after each video clip trial. Specifically, they were
asked to evaluate the level of pain and distress that they
thought the individual in the video clip was experiencing
using a visual analog scale ( VAS; left = no pain/distress,
right = severe pain/distress). Participants were then asked
how much distress they themselves felt when watching the
individual in pain using the same VAS (left = no distress,
right = severe distress). Ratings and response times were
recorded for each trail.
Finally, to measure participantʼs emotional responses
to the video clips, participants indicated the degree (1 =
not at all, 7 = extremely) to which they experienced 14
emotional states (Baston, Fultz, & Schoenrade, 1987) for
four randomly selected video clips for each group. Six of
these adjectives measured empathy (sympathetic, soft-
hearted, warm, compassionate, tender, and moved), and
eight of these adjectives measured personal distress
(alarmed, grieved, troubled, distressed, upset, disturbed,
worried, and perturbed). An empathy index was calculated
by averaging participantʼs responses to the six empathy
adjectives, and a personal distress index was calculated
by averaging participantʼs responses to the eight personal
distress adjectives (Baston et al., 1987).
Implicit Behavioral Measures
Following this task, participants completed a computer-
based IAT (Implicit Association Test) to measure implicit
AIDS stigma1 (Greenwald, McGhee, & Schwartz, 1998).
The purpose of the AIDS IAT was to assess unconscious
bias toward PWA that may be veiled in explicit question-
naire measures due to social desirability constraints. For
the AIDS IAT, participants first memorized the faces of four
individuals who were previously classified as healthy and
four individuals who were previously classified as having
AIDS. Then, pictures of the healthy and AIDS-infected indi-
viduals were presented on the computer screen, followed
by positive and negative target words. Participants were
asked to categorize these target words as either positive
or negative. In one block of trials, participants pressed
one key for pictures of the healthy individuals and words
with positive meanings and another key for pictures of
the AIDS-infected individuals and words with negative
meanings. In another block of trials, they pressed one key
for pictures of healthy individuals and words with negative
meanings and pressed a different key for pictures of AIDS-
infected individuals and words with positive meanings. Im-
plicit AIDS bias was defined as the difference in response
latency between these two blocks, and as such, larger val-
ues are indicative of greater implicit bias (Greenwald
et al., 1998). Measures of implicit AIDS bias were com-
puted using the improved scoring algorithm detailed in
Greenwald, Banaji, and Nosek (2003).
Self-report Dispositional Measures
Self-report questionnaires were also used to investigate
the relationship between explicit attitudes toward the
target groups and the behavioral and fMRI measures of
pain perception and empathy. Each of these measures
was completed at least one week before the testing pro-
cedure so as not to influence participantsʼ responses to
the experimental manipulations.2 To assess participantʼs
beliefs about AIDS and HIV, we administered Greenʼs
(1995) attitudes toward HIV scale. In addition, a 10-item
Likert-type scale was administered to investigate partici-
pantsʼ attitudes toward people who use illegal, intra-
venous drugs (Drug Use Questionnaire). In each of the
abovementioned scales, higher scores are associated
with greater endorsement of the respective characteristic
(i.e., more positive attitudes toward PWA and intravenous
drug users). Finally, as a manipulation check, two inde-
pendent Likert-type scales asked participants to sepa-
rately indicate whether the AIDS drug use and the AIDS
transfusion groups were responsible for their illness (1 =
strongly disagree, 7 = strongly agree) and whether
they were to blame for their condition (1 = have only
themselves to blame, 7 = not personally responsible for
their condition). After reverse coding the “blame” item,
responses were summed to create separate “blame” scales
for AIDS drug and AIDS transfusion groups. Higher scores
indicate greater blame for the target AIDS group.
fMRI Data Acquisition
Images were acquired using a whole-body GE 3.0-T MRI
scanner (Horizon LX, Milwaukee, WI). Functional imaging
was obtained using T2*-weighted gradient-echo spiral in/
out pulse sequence. Forty coronal slices of 4.2 mm slice
thickness with a 0.5-mm spatial gap were obtained for
160 repetitions (including three discarded acquisitions at
the onset of each of two runs) using the following param-
eters: repetition time (TR) = 3000 msec, echo time =
28 msec, flip angle = 84°, field of view = 24 cm, matrix =
64 × 64, and in-plane resolution = 3.75 × 3.75 mm.
An axial T1-weighted three-dimensional magnetization-
prepared rapid acquisition gradient-echo anatomical scan
was also acquired for three-dimensional localization (TR =
8 msec, echo time = 3.2 msec, flip angle = 6°, field of
view = 24 cm, matrix = 256 × 192, slice thickness =
1.5 mm, 124 slices).
Data Analysis
Behavioral Data Analysis
In addition to differences due to the general stigma
associated with AIDS, we predicted that attributions
988
Journal of Cognitive Neuroscience
Volume 22, Number 5
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
.
/
f
.
t
.
o
n
1
8
M
a
y
2
0
2
1
of responsibility for AIDS will influence participantsʼ per-
ceptions of pain experienced by PWA. Accordingly, in all
subsequent repeated measures ANOVAs, we decomposed
the three-level within-subject factor group (AIDS trans-
fusion, healthy, and AIDS drug use) into two orthogonal
contrasts. Our first contrast of interest was designed to cap-
ture differences in pain perception due to stigma alone and
as such, compared perceptions of healthy targets to per-
ceptions of the AIDS targets combined. The orthogonal
contrast concerned the distinction between AIDS transfu-
sion and AIDS drug use and thus specifically addressed
the role of attributions of responsibility in pain percep-
tion for stigmatized targets. Follow up analyses included
planned pairwise comparisons designed to explore the
nature of the relationship between each AIDS target group
and the healthy controls.
To investigate whether implicit and explicit attitudes
toward people with HIV/AIDS in general and the tar-
get groups in particular moderate pain and emotion
evaluations, we performed multiple regression analy-
ses with attitudes toward HIV, blame, and AIDS IAT
variables as predictors. It was predicted that group differ-
ences in pain perception would emerge as a result of
participantʼs implicit and explicit attitudes toward these
target groups.
Image Processing and Analysis
Image processing was carried out with SPM5 ( Wellcome
Department of Imaging Neuroscience, London, UK),
implemented in MATLAB 7.0 (Mathworks Inc., Sherborn,
MA). Preprocessing of the data included correction for
head motion (realignment to the first image volume), nor-
malization to the EPI template provided in SPM5, and
smoothing using a 6-mm FWHM isotropic Gaussian
kernel. Event-related responses were assessed by creating
fixed-effects general linear models for each subject. Regres-
sors of interest included the target cues and the pain
videos for each group (AIDS transfusion, healthy, and AIDS
drug use). The pain videos comprised of 0.5 sec of neu-
tral expression, followed by 3.0 sec of pained expression,
and the 3.0-sec TR was synchronized to the onset of
pain that occurred 0.5 sec into in each video clip. However,
pain video regressors were analyzed at the onset of the neu-
tral expression clip to capture the ecologically valid transi-
tion from neutral to pain.3 Regressors were convolved with
a canonical hemodynamic response function (hrf ) and its
temporal and dispersion derivatives. The latter derivatives
were incorporated into the model to account for poten-
tial differences in neural and hemodynamic responses
to the differing groups of video stimuli (Lamm et al.,
2007; Friston et al., 1998). Following model estimation,
contrasts were calculated for each subject to assess within-
subject differences in perceptions of pain by target group.
Contrasts were as follows: pain > fixation, healthy > fixa-
ción, AIDS transfusion > fixation, AIDS drug use > fixa-
ción. The resulting pairwise contrast images were then
entered into second level random-effects repeated mea-
sures ANOVAs. Except where noted, a voxel-level thresh-
old of p < .001 for group contrasts, uncorrected for
multiple comparisons (with an extent threshold of 10
continuous voxels), was used to identify significant activity
changes in pain-related regions and other regions of
a priori interest based on previous fMRI studies using sim-
ilar facial stimuli (Lamm et al., 2007; Saarela et al., 2007;
Simon, Craig, Miltner, & Rainville, 2006; Botvinick et al.,
2005). These included regions associated with theory of
mind (TPJ and STS) and emotion regulation [i.e., dACC,
medial prefrontal cortex (mPFC), orbital midfrontal cortex
(oMFC), bilateral inferior frontal gyri (IFG)]. Activations
were overlaid on a representative high-resolution structural
T1-weighted image from a single subject from the SPM5
canonical image set, coregistered to the Montreal Neuro-
logical Institute (MNI) space.
In addition to whole-brain analyses, specific ROI (region
of interest) analyses were computed with the MarsBaR tool-
box in SPM5. To more closely examine the hypothesized
differences in pain perception by target group, we selected
ROIs in areas previously demonstrated to be associated with
processing facial expressions of pain (Lamm et al., 2007;
Saarela et al., 2007; Simon et al., 2006; Botvinick et al.,
2005). These ROIs included the AI, the aMCC, the perigenu
cingulate cortex (pgCC), and the periaqueductal gray (PAG).
Furthermore, to explore the extent to which emotion
regulation may be differentially involved in pain perception
by target group, ROIs were selected in areas associated with
emotion regulation and cognitive control, including the
dACC, the oMFC, and the bilateral IFG (Kim & Hamann,
2007; Ochsner et al., 2002).
All ROI were functionally defined as 6-mm spherical re-
gions (3-mm radius) centered on the subject-specific
peak coordinate showing a significant main effect of pain
(collapsed across group membership) versus fixation. Func-
tional ROI coordinates overlapped corresponding ana-
tomical regions and fell within the range of coordinates
reported in two recent meta-analyses on fMRI studies on
pain empathy (Jackson, Rainville, et al., 2006) and on em-
pathy, theory of mind, and perspective taking (Decety &
Lamm, 2007).
Estimates of percent signal change were extracted for
each ROI by target group and were submitted to 1 × 3
(group: AIDS transfusion, healthy, and AIDS drug use) re-
peated measures ANOVAs. As with the behavioral pain
ratings, the contrasts of interest within the omnibus F
test concerned the distinction between the healthy and
the AIDS targets combined and between AIDS trans-
fusion and AIDS drug use targets. Follow-up analyses ex-
plored the nature of the relationship between each AIDS
target group and the healthy control condition. As with
the behavioral data, zero-order correlations and multiple
regression analyses were performed to investigate whether
implicit and explicit attitudes toward people with HIV/AIDS
in general and the target groups in particular moderate
Decety, Echols, and Correll
989
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
f
/
.
.
t
.
o
n
1
8
M
a
y
2
0
2
1
Table 1. Mean and SD Scores for the Dispositional Measures
Mean (SD)
Cronbachʼs α
Attitudes toward HIV
Blame for AIDS drug
13.8 (10.2)
10.4 (2.95)
Blame for AIDS transfusion
2.91 (2.39)
Drug Use Questionnairea
26.9 (6.26)
AIDS IAT
0.532 (0.278)
.86
.75
.95
.74
aItems specifically related to treatment (Items 7 and 10) were deleted
from the Drug Use Questionnaire to provide the adequate interitem
reliability reported above.
the abovementioned hemodynamic responses to each
target group.
BEHAVIORAL RESULTS
Validation of Study Assumptions
Consistent with our predictions, participants believed
that PWA as a result of intravenous drug use were signif-
icantly more to blame for their condition than PWA as a
result of an infected blood transfusion, t(21) = 9.97, p <
.001. Results from the AIDS IAT also supported predic-
tions about attitudes toward the target groups: the AIDS
IAT showed that, on average, participants demonstrated
a negative bias toward PWA relative to healthy people,
t(21) = 7.93, p < .001. Descriptive statistics of these tests
and the self-report measures can be viewed in Table 1.
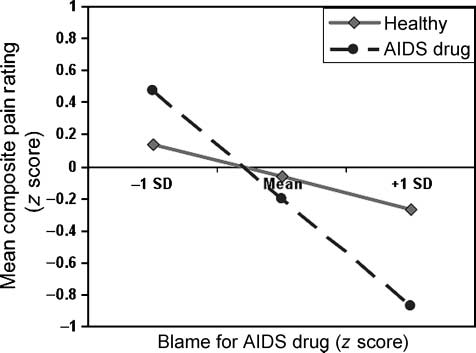
Figure 2. Effect of blame on mean composite pain ratings across
groups, controlling for implicit AIDS bias and explicit attitudes
toward HIV. Participants who blamed PWA as a result of drug use
for their condition attributed significantly less pain to AIDS drug use
individuals than healthy individuals, t(18) = 2.83, p = .01, whereas
participants who did not blame PWA as a result of drug use for their
condition tended to attribute more pain to AIDS drug use individuals
as compared with healthy individuals, t(18) = −1.55, p = .14.
sonal distress and empathy scales of Baston et al. (1987)
were highly correlated within group (all r > .60, pag < .001).
Consequently, composite pain ratings and composite emo-
tion ratings were computed separately for AIDS transfu-
sion, healthy, and AIDS drug use groups. No significant
participant gender differences were found in pain and
in emotion evaluations across group; as a result, analyses
were collapsed across gender.
Video Evaluations
Video evaluations were z transformed using the mean and
the SD from the combined group ratings. Pain and distress
VAS ratings, and the personal distress VAS ratings and per-
Main Effects
Analysis of composite pain ratings showed that partici-
pants rated the pain of the individuals depicted in the
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
f
.
.
t
/
.
o
n
1
8
M
a
y
2
0
2
1
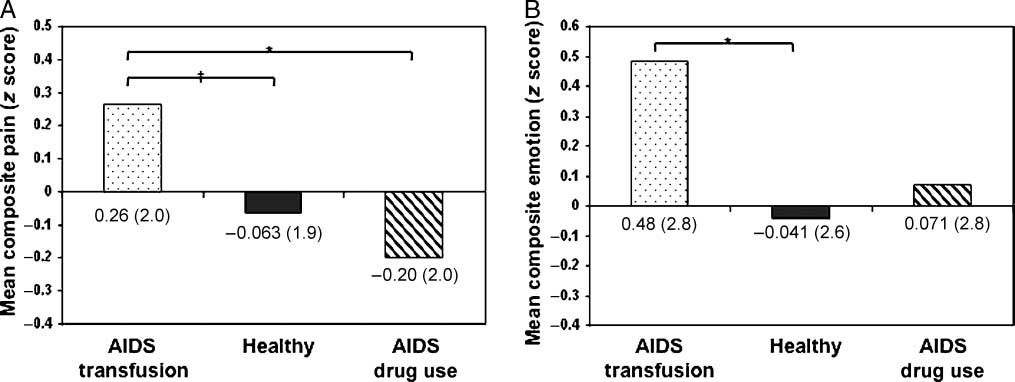
Figure 1. Means and SDs of video evaluations for (A) composite pain ratings (z score) and (B) composite emotion ratings (z score). Results
from significant contrasts of interests are highlighted (*p = .05; †
p = .08).
990
Journal of Cognitive Neuroscience
Volume 22, Number 5
videos differently as a function of the targetʼs group label.
The contrast comparing perceptions of pain of healthy
targets to AIDS targets was not significant, t(21) =
−0.71, p > .15. Sin embargo, in line with our attribution pre-
dictions, participants rated the pain of AIDS transfusion
targets as greater than the pain of AIDS drug use targets,
t(21) = 2.18, pag = .04. Follow-up planned comparisons
showed that although the pain of AIDS transfusion targets
was perceived as marginally greater than that of healthy
controls, t(21) = 1.81, pag = .08, the pain of AIDS drug use
targets was not perceived to be significantly different from
that of healthy targets, t(21) = 0.84, p > .15 (Figura 1A).
Analyses of the composite emotion ratings revealed a
similar but weaker effect such that participants reported
a trend toward experiencing more empathy and personal
distress for AIDS transfusion targets than AIDS drug use
objetivos, t(21) = 1.66, pag = .11. The orthogonal contrast
(healthy vs. the combined AIDS targets) was significant,
t(21) = −2.57, pag = .02. Sin embargo, planned comparisons
showed that this effect was primarily driven by the fact
that participants reported greater empathy and personal
distress in response to AIDS transfusion targets than
healthy targets, t(21) = 3.10, pag < .01, whereas reactions
to healthy and AIDS drug use targets did not differ, t(21) =
0.62, p > .15 (Figura 1B).
Moderation Analyses
When investigating the relationship between AIDS drug
use predictors (es decir., AIDS IAT, attitudes toward HIV, blame
for AIDS drug use, and attitudes toward drug users) y
the discrepancy in pain ratings between healthy and AIDS
drug use targets, only blame for AIDS drug use emerged
as a significant zero-order predictor for the difference in
pain ratings between healthy and AIDS drug use targets,
r= .52, pag = .01 (all other | r | < .38, p > .15). Más-
encima, when controlling for explicit attitudes toward HIV,
both the AIDS IAT, b = .33, t(18) = 2.28, pag = .04, y
the blame for AIDS drug use, b = .470, t(18) = 2.79, pag =
.01, emerged as significant predictors of the difference in
pain ratings between healthy and AIDS drug individuals
(all other | b | < .03, t < 1, p > .15).4 De este modo, (a) the more
participants demonstrated a negative implicit association
toward PWA in general and (b) the more they explicitly
reported that targets in the AIDS drug use condition were
personally to blame for their condition, the less pain they
attributed to AIDS drug individuals relative to healthy in-
dividuals (ver figura 2).
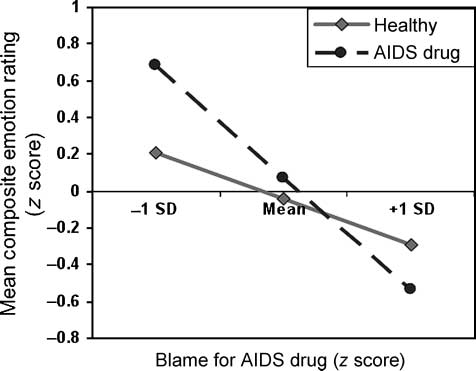
Similarmente, only blame for AIDS drug use emerged as a
marginally significant zero-order predictor for the differ-
ence in empathy and personal distress ratings between
healthy and AIDS drug use targets, r= .391, pag = .07 (todo
otro | r | < .26, p > .15). Sin embargo, when controlling
for explicit attitudes toward HIV and AIDS IAT, el efecto
of blame for AIDS drug use, b = .36, t(18) = 1.61, pag =
.13 (all other | b | < .2, t < 1, p > .15) was reduced and
emerged as a trending predictor of the difference in empa-
thy and personal distress ratings between healthy and AIDS
drug individuals.5 Thus, the more participants reported
that targets in the AIDS drug use condition were personally
responsible for their stigma, the less likely they were to ex-
press empathy and personal distress while observing those
targets relative to healthy targets (ver figura 3).
Notablemente, neither implicit AIDS bias (AIDS IAT), explicit
attitudes toward HIV, or blame for AIDS transfusion did
not emerged as a significant predictors of the difference
between AIDS transfusion and healthy targets on either
composite pain ratings or composite emotion ratings, | b |
< .2, t < 1, p < .15.
D
o
w
n
l
o
a
d
e
d
fMRI RESULTS
Network of Areas Involved in the Processing of Pain
Collapsing across group, analyses showed that observing
individuals in pain was associated with activation in a num-
ber of regions involved in the processing of the sensory and
affective content of the videos. Bilateral activation was de-
tected in the medial and lateral occipital cortex, including
the fusiform gyrus. In addition, increased hemodynamic
activity was found in the neural circuit underpinning first-
hand processing of pain, including AI, dACC, supplemen-
tary motor cortex, and PAG. Activation was also observed
in the pgCC and oMFC and bilaterally in the IFG, mPFC,
TPJ, and STS (see Table 2). Similar patterns of activity
were also observed when comparing each target group to
fixation baseline.
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
t
/
.
.
f
.
o
n
1
8
M
a
y
2
0
2
1
Figure 3. Effect of blame on mean composite emotion ratings
across groups, controlling for implicit AIDS bias and explicit attitudes
toward HIV. Participants who did not blame PWA as a result of drug
use for their condition tended to experience more empathy and
personal distress in response to the pain of AIDS drug use individuals
than healthy individuals, t(18) = −1.66, p = .12. No mean differences
in composite emotion ratings where observed between AIDS drug
use and healthy individuals for participants who blamed AIDS drug
use individuals for their condition.
Decety, Echols, and Correll
991
Table 2. Regions That Demonstrate Significant Hemodynamic Signal Change during the Observation of Targets in Pain Collapsed
across Group, as Compared with Baseline Fixation Cross ( p < .001, k > 10)
MNI Coordinates
Regiones del cerebro
R AI
L AI
R perigenual cingulate cortex
R dACC
L medial pFC
L superior frontal gyrus/L dorsal aMCC
R superior frontal gyrus/dorsal midcingulate cortex
L orbital midfrontal gyrus
L IFG
R IFG
R temporal-parietal junction/midtemporal gyrus
R middle temporal gyrus
R fusiform gyrus
L fusiform gyrus
R PAG
L = left hemisphere; R = right hemisphere.
ak = 0.
X
36
−26
−40
−26
8
2
−2
−6
12
−4
−52
−46
52
50
60
62
50
38
−34
2
y
24
30
26
26
40
30
42
18
−2
34
24
24
32
20
−38
−50
−10
−70
−62
−22
z
−8
0
−4
−10
2
36
26
52
58
−22
0
20
4
24
−4
0
−18
−14
−14
−12
t
4.50
3.75
3.60
3.70
3.73a
3.82
4.13
4.02a
3.82a
3.85a
4.68
5.40
6.65
3.72
3.02
4.07
3.62
4.91
3.75
4.76a
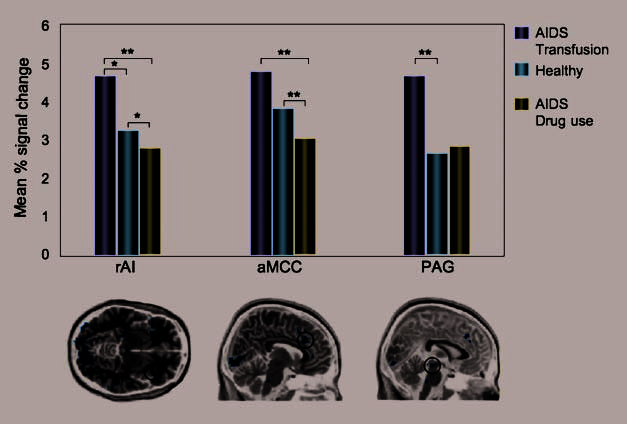
ROI Associated with Pain Perception
Right AI
The contrast comparing hemodynamic activation in the
right AI between healthy and AIDS targets was not signifi-
cant, t(21) = 1.21, p > .15. Sin embargo, the orthogonal con-
trast between AIDS transfusion and AIDS drug use
showed significantly greater hemodynamic activity in
the right AI in response to the pain of AIDS transfusion
targets as compared with AIDS drug use targets, t(21) =
2.45, pag = .02. Follow-up analyses showed marginally
more right AI activity when participants viewed AIDS
transfusion as compared with healthy targets, t(21) =
1.95, pag = .07, and when viewing healthy targets as com-
pared with AIDS drug use targets, t(21) = 1.94, pag = .07.
Anterior Midcingulate Cortex
The contrast comparing aMCC activity when observing the
pain of healthy and AIDS targets combined was not signifi-
cant, t(21) = 0.084, p > .15. Sin embargo, significant signal
change was detected in the aMCC when participants
watched painful facial expressions of AIDS transfusion tar-
gets as compared with AIDS drug use targets, t(21) = 2.59,
pag = .02. As expected, significantly more aMCC activity was
found when participants viewed healthy targets as com-
pared with AIDS drug use targets, t(21) = 2.09, pag = .05.
No significant signal change was detected in the aMCC
when participants viewed AIDS transfusion and healthy
objetivos, t(21) = 1.00, p > .15 (Mesa 3).
Periaqueductal Gray
A nonsignificant trend was found in the PAG in response
to the pain of AIDS transfusion targets as compared with
AIDS drug use targets, t(21) = 1.57, pag = .13. Curiosamente,
the orthogonal contrast comparing PAG activity between
healthy and AIDS targets was significant, t(21) = −2.33,
pag = .03; sin embargo, this result was primarily due to a signifi-
cant difference in PAG activity between AIDS transfusion
992
Revista de neurociencia cognitiva
Volumen 22, Número 5
D
oh
w
norte
yo
oh
a
d
mi
d
yo
yo
/
/
/
/
j
F
/
t
t
i
t
.
:
/
/
F
r
oh
metro
D
h
oh
t
w
t
norte
pag
oh
:
a
/
d
/
mi
metro
d
i
F
t
r
oh
pag
metro
r
C
h
.
s
pag
i
yo
d
v
i
mi
r
mi
r
C
C
t
.
h
metro
a
i
r
mi
.
d
tu
C
oh
oh
metro
C
/
norte
j
a
oh
r
C
t
i
norte
C
/
mi
a
–
pag
r
d
t
i
2
C
2
yo
5
mi
–
9
pag
8
d
5
F
1
/
9
2
3
2
9
/
1
5
5
/
9
9
oh
8
C
5
norte
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
oh
pag
C
d
norte
.
b
2
y
0
gramo
0
tu
9
mi
.
s
t
2
oh
1
norte
2
6
0
6
7
.
S
pag
mi
d
pag
F
mi
metro
b
y
b
mi
gramo
r
tu
2
mi
0
2
s
3
t
/
j
.
t
/
F
.
.
oh
norte
1
8
METRO
a
y
2
0
2
1
Mesa 3. Mean Coordinates, Estadísticas descriptivas, and Results for Nine 1 × 3 (Group: Healthy, AIDS Transfusion, and AIDS Drug Use)
Repeated Measures ANOVAs Comparing Average Percent Signal Change When Observing Pain > Fixation across Group Condition
MNI Coordinates
Group Mean (Dakota del Sur)
Brain Region
AI
aMCC
pgCC
dACC
PAG
oMFC
IFG
R
l
R
R
R
R
R
R
l
X
38
−33
6
7
2
2
1
48
−46
y
21
22
23
41
42
−28
43
26
20
z
−4
−3
26
6
25
−18
−15
7
9
Coordinates by subject are available upon request.
*pag = .05.
**pag = .01.
***pag = .10.
Healthy
AIDS Transfusion
AIDS Drug Use
F
3.44 (3.08)
3.31 (2.90)
4.21 (4.34)
3.65 (3.53)
4.23 (3.46)
3.22 (3.33)
3.96 (4.01)
5.88 (3.00)
5.91 (6.07)
4.90 (4.93)
3.83 (4.33)
5.06 (5.44)
4.17 (5.05)
4.87 (3.41)
4.88 (5.42)
4.72 (5.33)
7.76 (6.29)
6.45 (5.93)
2.94 (2.67)
3.16 (2.69)
3.27 (3.75)
2.81 (2.88)
3.70 (2.55)
3.56 (3.18)
4.35 (5.26)
6.08 (4.23)
4.90**
0.66
3.43*
1.66
1.73
3.23*
0.67
2.48***
6.12 (4.77)
0.19
and healthy targets, t(21) = 2.29, pag = .04, as PAG activity
when watching healthy and AIDS drug use targets was not
significantly different, t(21) = −0.836, p > .15 (Cifra 4).
ROI Associated with Emotion Regulation
Right IFG
A similar pattern of results was observed in the right IFG:
A nonsignificant difference was observed in the right IFG
in response to the pain of AIDS transfusion targets as com-
pared with AIDS drug use targets, t(21) = 1.49, pag = .15.
The orthogonal contrast comparing right IFG activity be-
tween healthy and AIDS targets was marginally significant,
t(21) = 1.80, pag = .09, due to a marginally significant differ-
ence in right IFG activity between AIDS transfusion and
healthy targets, t(21) = 1.93, pag = .07. Right IFG activity
when watching healthy and AIDS drug use targets did
not significantly differ, t(21) = −0.33, p > .15.
ROI Moderation Analyses
When investigating the relationship between the AIDS
drug use predictors (es decir., AIDS IAT, attitudes toward
HIV, blame for AIDS drug use, and attitudes toward drug
users) and the hemodynamic activity observed when
viewing AIDS drug use targets, AIDS IAT emerged as a
Cifra 4. ROI demonstrating
significant differences in
percent signal change by
target group. Results from
significant contrasts of
interests are highlighted
(*p ≤ .05; **pag < .10).
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
.
f
.
.
t
/
o
n
1
8
M
a
y
2
0
2
1
Decety, Echols, and Correll
993
significant zero-order predictor for activity in the right
IFG (r = .45, p = .04) and attitudes toward drug use
emerged as a significant zero-order predictor for activity
in the mPFC (r = .65, p = .001; all other regions | r | <
.38, p > .08). Sin embargo, when the aforementioned AIDS
drug use predictors were included in multiple regression
analyses to assess whether they moderated the difference
in hemodynamic activity between healthy and AIDS drug
use targets, no significant predictors emerged for any of
the ROI investigated (all t < 1, p > .15).
Notablemente, when investigating the relationship between
the AIDS transfusion predictors (es decir., AIDS IAT, attitudes
toward HIV, blame for AIDS transfusion) and the hemo-
dynamic activity observed when viewing AIDS transfusion
objetivos, only attitudes toward HIV emerged as a significant
zero-order correlate for hemodynamic activity in the dACC
when watching AIDS transfusion individuals (r= .42, pag =
.05; all other regions | r | < .39, p > .08). Además, cuando
controlling for blame for aids transfusion and AIDS IAT,
attitudes toward HIV emerged as a significant predictor
for the difference in hemodynamic activity between
healthy and AIDS transfusion individuals in the left AI,
b = −1.7, t(18) = −2.4, pag = .03, all other | b | < 1, t(18)
< .15, and dACC, b = −1.7, t(21) = −3.2, p < .01 (all other
| b | < 1.3, p < .15). Furthermore, the difference in hemo-
dynamic activity observed in the PAG when viewing healthy
controls as compared with AIDS transfusion remained sig-
nificant when controlling for these AIDS transfusion pre-
dictors, b = −1.7, t(21) = −2.3, p = .04 (all other | b | <
1.1, p < .15). Thus, the more participants expressed posi-
tive attitudes toward HIV, the more hemodynamic activity
was observed in the left AI, dACC, and PAG when view-
ing AIDS transfusion individual as compared with healthy
controls.
DISCUSSION
When witnessing another person experiencing pain, the
scope of observerʼs reaction can range from concern for
personal safety, including feelings of alarm, fear, and avoid-
ance, to concern for the other person, including compas-
sion, sympathy, and caregiving (Goubert et al., 2009). It is
important to explore the interpersonal factors that affect
oneʼs perceptions of pain to understand and to predict
how an observer will empathize and react to anotherʼs
distress. Using both behavioral and brain measures, the
present investigation explored whether an observersʼ per-
ception of a targetʼs pain was modulated by stigmatization
of the target and whether the target bore responsibility for
his or her stigmatized status.
Attributions of Responsibility and Empathy for Pain
Consistent with our hypothesis regarding attributions
of responsibility for oneʼs stigmatized status, behavioral
results showed that participants were significantly more
sensitive to the pain of targets who were not responsible
for their stigmatized condition (people who contracted
AIDS as the result of a blood transfusion) than either con-
trols (healthy individuals) or targets who were held respon-
sible for their condition (those who contracted AIDS
through illegal drug use). In addition, participants ex-
pressed more empathy and personal distress in response
to the pain of people who were not responsible for their
stigmatized condition as compared with controls. Impor-
tantly, the differences between reactions to healthy controls
and targets that were held responsible for their condi-
tion depended on individual differences in attributions of
blame. The more participants blamed AIDS drug use targets
for their condition, the less pain and empathy they reported
when viewing their distress (compared with controls).
Demonstrating congruence across behavioral and
functional neuroimaging methodologies, these video eval-
uations were supported by the modulation of the hemo-
dynamic response by target group. ROI analyses in areas
previously associated with both first- and second-hand
pain perception showed significant differences in percent
signal change between AIDS transfusion, healthy, and AIDS
drug use targets. Participants demonstrated the greatest
hemodynamic activity in areas involved in pain resonance
when viewing AIDS transfusion individuals, often respond-
ing more to these targets than to either the healthy con-
trols or the AIDS drug use targets. By contrast, the AIDS
drug use targets prompted lower levels of resonance than
the control condition in the aMCC. Combined, results indi-
cated that attributions of responsibility moderated both the
explicit evaluations and the hemodynamic activity under-
lying empathic resonance.
Substantial behavioral evidence has shown that individ-
uals demonstrate negative attitudes toward AIDS victims,
particularly those who are considered to be responsible
for their disease (i.e., Devine, Plant, & Harrison, 1999;
Weiner et al., 1988). The present investigation demon-
strates that this negative evaluation may affect the percep-
tion of these targetsʼ pain. These findings suggest that the
perception of pain is not the exclusive domain of automatic
bottom–up processing of nociceptive information (Fan &
Han, 2008; Preston & de Waal, 2002), but that somatic
sensorimotor resonance is profoundly modulated by top–
down considerations, including how observers concep-
tualize both the situation and the person who is expressing
pain. It is interesting to note, however, that different pat-
terns of variables predicted participantʼs behavioral and
brain responses (i.e., blame for AIDS drug use predicted
a decreased sensitivity to the pain of AIDS drug use targets
in behavioral pain ratings, but not in areas of the brain
associated with pain processing). Additional research is
necessary to elucidate the complex relationship between
cover and overt information processing in social cognition.
AIDS Transfusion: A Special Case
Notably, the abovementioned differences in pain and em-
pathy ratings between controls (healthy) and stigmatized
994
Journal of Cognitive Neuroscience
Volume 22, Number 5
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
.
.
t
/
.
f
o
n
1
8
M
a
y
2
0
2
1
targets that were not held responsible for their condition
(AIDS transfusion) remained even when controlling
for either implicit or explicit attitudes about PWA. In fact,
positive attitudes toward AIDS were associated with in-
creased hemodynamic activity in the areas associated
with pain processing when viewing AIDS transfusion targets
only as compared with controls. This may indicate that
AIDS transfusion targets were considered to be a subtype
of the general AIDS category and, thus, viewed as not repre-
sentative of the stigmatized group as a whole (Hewstone,
Macrae, Griffiths, & Milne, 1994). As such, the pain of AIDS
transfusion individuals may have warranted additional
sympathy and understanding relative to healthy controls
as befitting their objectively disadvantaged health situation.
In corroboration with this hypothesis, we found trends
in neural regions associated with emotion regulation
(Posner, Rothbart, & Sheese, 2007; Ochsner et al. 2002)
when viewing AIDS transfusion targets as compared with
other target groups. Participants tended to exhibit more
signal change in the right inferior frontal cortex when view-
ing AIDS transfusion individuals relative to AIDS drug use
individuals. In line with the hypothesis that AIDS transfu-
sion targets were subtyped within the AIDS category and
not stigmatized per se, this trend may indicate the relative
increase in cognitive control required to process AIDS
transfusion targets as a disadvantaged group worthy of
sympathy and understanding (over and above that of
healthy controls). Future research will need to address
the relative contribution of top–down and bottom–up fac-
tors that modulate the pain resonance system.
AIDS Stigma and Empathy for Pain
Our hypothesis predicting reduced hemodynamic activity
toward stigmatized targets in general as compared with
healthy controls was not supported by either behavioral
nor neuroimaging data, as evidenced by a series of non-
significant differences in video evaluations and underlying
hemodynamic activity between the healthy targets and
the AIDS targets combined. Instead, effects appear to be
primarily driven by attributions of responsibility for acquir-
ing said stigma. However, it is possible that the effect of
attributions of responsibility was particularly emphasized
in this investigation by a design that explicitly blocked
AIDS transfusion and AIDS drug use targets separately
from healthy targets. This may have biased observers to
treat AIDS transfusion and AIDS drug use targets as separate
entities and reduced the emphasis on the general stigma
associated with AIDS. It is possible that when confronted
with an AIDS victim in a real-world setting, (i) how the
individual contracted the disease will not be readily appar-
ent, and (ii) such attributions of responsibility may not
modulate how the individual is perceived to the same ex-
tent as observed in this investigation.
On a related note, previous studies investigating the neu-
rological underpinnings of stigma have examined how such
stimuli elicit disgust-like reactions in the observer and as
such result in activation in the amygdala (e.g., Krendl,
Macrae, Kelley, Fugelsang, & Heatherton, 2006). Our data
do not appear to elicit this visceral response, potentially
due to (a) the length of our stimuli presentation, (b) the
abovementioned fact that general stigma associated with
AIDS stigma was not emphasized in the design of this ex-
periment, and (c) that instead of using visually arousing
stimuli, all of the targets in the video clips shared many
visual characteristics with the participants themselves (i.e.,
targets were age matched to a college sample, white,
etc.). Instead, in the current investigation, a targetʼs stig-
matization was communicated by a simple word label and
thus was not necessarily expected to generate an auto-
matic avoidance response.
Limits of the Current Investigation and Future
Directions of Research
In addition to the design constraints outlined above,
there are other features of the present investigation that
should be taken into account when considering the ex-
ternal validity of the findings. For example, a limitation
of this investigation may lie in the explicit measurement
of AIDS bias and intravenous drug use. In such a liberal
intellectual community as the University of Chicago, both
explicit (i.e., rules and regulations of conduct) and implicit
social norms exist that endorse empathy and censure pre-
judice. Thus, it is possible that a self-presentation bias
may have prevented participants from reporting the true
extent of their feelings toward PWA and intravenous drug
users on the self-report measures, video evaluations, and
even in their resonance to the targetsʼ pain. This self-
presentation bias may have particularly influenced partici-
pantsʼ responses to AIDS drug use targets as compared
with healthy controls and may have contributed to the
lack of mean level differences between these groups on
most behavioral and hemodynamic measures. This self-
presentation bias, should it exist, could limit the likelihood
of detecting and replicating a significant relationship
between explicit measures of empathy and prejudice and
behavioral and hemodynamic responses toward different
groups of people expressing pain.
Further, participants were primarily young adults
drawn from the student population of the University of
Chicago, a private postsecondary education institution.
As Herek (1999) states that “younger and better educated
respondents consistently manifest lower levels of AIDS
stigma than older respondents and those with lower
education” (p. 1104), it is possible that the attitudes to-
ward persons with AIDS generally, and AIDS drug use in
particular, reflected in this study are more liberal than the
attitudes of the general population. The fact that the cur-
rent investigation did result in significant differences in
pain resonance across stigmatized target group despite
these population and design considerations may speak
to the strength of the reported findings. However, this
is an empirical question that should be investigated by
Decety, Echols, and Correll
995
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
t
t
f
/
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
/
.
f
.
.
t
o
n
1
8
M
a
y
2
0
2
1
selecting a larger and more representative sample of the
population as a whole.
Finally, the present investigation explored how individual
differences in attitudes and attributions of responsibility
moderated participantsʼ perceptions of pain, operation-
alized by both explicit video evaluations and somatosen-
sory resonance observed during fMRI. However, it is yet
unclear as to how this shared perception (or lack thereof )
is related to the documented helping disparities between
in- and out-group members (i.e., Stürmer et al., 2006).
Thus, future directions of research will attempt to directly
relate shared resonance and empathic accuracy to helping
behaviors for both in- and out-group members.
Conclusion
By employing a unique combination of attitudinal, behav-
ioral, and functional neuroimaging measures, the present
investigation explored the effect of attributions of re-
sponsibility and social stigma on empathy for pain. It is
the hope that such an interdisciplinary perspective will
reveal manifestations of congruence (and incongruence)
between attitudes, behavior, and the brain and will provide
important insight in current models of empathy and pain
processing.
Acknowledgments
The study was supported by an NSF (BCS-0718480) award to J. D.
We would also like to thank Claus Lamm and Michael Sargent
for their invaluable help with data analysis and the members of
the Correll and Decety research laboratories for their feedback
in the study design and manuscript.
Reprint requests should be sent to Prof. Jean Decety, Depart-
ments of Psychology and Psychiatry, The University of Chicago,
5848 South University Avenue, Chicago, IL 60637, or via e-mail:
decety@uchicago.edu.
Notes
1. To investigate whether participantʼs behavioral or hemody-
namic responses to the PWA were influenced by a bias against
homosexuality (a characteristic previously associated with HIV/
AIDS), we conducted a sexuality IAT to measure implicit bias
against homosexuality. Although results showed that participants
demonstrated a negative bias toward homosexuality relative to
heterosexuality, t(21) = 3.24, p < .003, implicit homosexuality
bias failed to predict the difference in pain or emotion ratings or
hemodynamic activity between healthy and AIDS drug use targets
or healthy and AIDS transfusion targets.
2. To investigate whether dispositional empathy, emotion con-
tagion, or motivation to control prejudice moderated participants
empathic resonance to the targets by group, we administered
the perspective-taking subscale of the Interpersonal Reactivity
Index (Davis, 1994), the Emotion Contagion Scale (Doherty,
1997), and an AIDS-specific version of Plant and Devineʼs (1998)
five-item Internal Motivation to Control Prejudice Questionnaire.
However, these trait variables failed to predict the difference
in pain or emotion ratings, or hemodynamic activity between
healthy and AIDS drug use targets or healthy and AIDS transfusion
targets. Furthermore, these trait variables failed to significantly
mediate the pattern of responses observed in all multiple regres-
sion analyses.
3. Pain video regressors were also modeled beginning at the
pain expression 0.5 sec after the onset of the clip, yielding similar
results with slightly smaller signal strength.
4. AIDS IAT and blame for AIDS drug use remained significant
predictors of the difference in composite pain ratings between
healthy and AIDS drug individuals when controlling for attitudes
toward drug use.
5. The addition of the attitudes toward drug use scale to the
model increases the significance of blame for AIDS drug use as
a predictor to from p = .13 to p = .05.
REFERENCES
Ames, D. (2004). Inside the mind readerʼs tool kit: Projection
and stereotyping in mental state inference. Journal of
Personality and Social Psychology, 87, 340–353.
Baston, D., Fultz, J., & Schoenrade, P. (1987). Distress and
empathy: Two qualitatively distinct vicarious emotions
with different motivational consequences. Journal of
Personality, 55, 19–39.
Batson, D., Sager, K., Garst, E., Kang, M., Rubchinsky, K.,
& Dawson, K. (1997). Is empathy-induced helping due
to self-other merging? Journal of Personality and Social
Psychology, 73, 495–509.
Botvinick, M., Jha, A., Bylsma, L. M., Fabian, S. A., Solomon,
P. E., & Prkachin, K. M. (2005). Viewing facial expression
of pain engages cortical areas involved in the direct
experience of pain. Neuroimage, 25, 312–319.
Capitanio, J. P., & Herek, G. M. (1999). AIDS-related stigma
and attitudes towards injecting drug users among Black
and White Americans. American Behavioral Scientist,
42, 1144–1157.
Cheng, Y., Lin, C., Liu, H. L., Hsu, Y., Lim, K., Hung, D., et al.
(2007). Expertise modulates the perception of pain in
others. Current Biology, 17, 1708–1713.
Craig, K. D., Prkachin, K., & Grunau, R. (2001). The facial
expression of pain. In D. C. Turk & R. Melzack (Eds.),
Handbook of pain assessment (2nd ed., pp. 153–169).
New York: Guilford.
Crandall, C., & Martinez, R. (1996). Culture, ideology, and
anti-fat attitudes. Personality and Social Psychology Bulletin,
22, 1165–1176.
Crocker, J., Major, B., & Steele, C. (1998). Social stigma. In
D. Gilbert, S. T. Fiske, & G. Lindzey (Eds.), The handbook
of social psychology (4th ed., Vol. 2, pp. 504–553).
New York: McGraw-Hill.
Davis, M. (1994). Empathy: A social psychological approach.
Madison: Westview Press.
Decety, J., & Batson, C. D. (2007). Social neuroscience
approaches to interpersonal sensitivity. Social Neuroscience,
2, 151–157.
Decety, J., & Grèzes, J. (2006). The power of imagination:
Imagining oneʼs own and otherʼs behavior. Brain Research,
1079, 4–14.
Decety, J., & Jackson, P. L. (2004). The functional architecture
of human empathy. Behavioral and Cognitive
Neuroscience Reviews, 3, 71–100.
Decety, J., & Lamm, C. (2007). The role of the right
temporoparietal junction in social interaction: How
low-level computational processes contribute to
meta-cognition. Neuroscientist, 13, 580–593.
Decety, J., & Moriguchi, Y. (2007). The empathic brain and
its dysfunction in psychiatric populations: Implications
for intervention across different clinical conditions.
Biopsychosocial Medicine, 1, 22–65.
996
Journal of Cognitive Neuroscience
Volume 22, Number 5
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
/
f
.
.
t
.
o
n
1
8
M
a
y
2
0
2
1
Derbyshire, S. W. G. (2000). Exploring the pain “neuromatrix.”
Current Review of Pain, 6, 467–477.
Devine, P., Plant, E., & Harrison, K. (1999). The problem of
“us” versus “them” and AIDS stigma. American Behavioral
Scientist, 42, 1208–1224.
Doherty, R. W. (1997). The emotional contagion scale: A
measure of individual differences. Journal of Nonverbal
Behavior, 21, 131–154.
Donaldson, D. I., & Buckner, R. L. (2001). Effective paradigm
design. In P. Jezzard, P. M. Mathews, & S. M. Smith
(Eds.), Functional MRI: An introduction to methods
(pp. 177–195). Oxford: Oxford University Press.
Fan, Y., & Han, S. (2008). Temporal dynamic of neural
mechanisms involved in empathy for pain: An event-related
brain potential study. Neuropsychologia, 46, 160–173.
Friston, K. J., Fletcher, P., Josephs, O., Holmes, A. P., Rugg,
M. D., & Turner, R. (1998). Event-related fMRI: Characterizing
differential responses. Neuroimage, 7, 30–40.
Goubert, L., Craig, K. D., & Buysse, A. (2009). Perceiving
others in pain: Experimental and clinical evidence on the
role of empathy. In J. Decety & W. Ickes (Eds.), The social
neuroscience of empathy (pp. 153–165). Cambridge, MA:
MIT Press.
Green, G. (1995). Attitudes towards people with HIV: Are
they as stigmatizing as people with HIV perceive them
to be? Social Sciences Medicine, 41, 557–568.
Greenwald, A., Banaji, M., & Nosek, B. (2003). Understanding
and using the implicit association test: I. An improved
scoring algorithm. Journal of Personality and Social
Psychology, 85, 197–216.
Greenwald, A., McGhee, J., & Schwartz, J. (1998). Measuring
individual differences in social cognition: The implicit
association test. Journal of Personality and Social
Psychology, 74, 1464–1480.
Gu, X., & Han, S. (2007). Attention and reality constraints on
the neural processes of empathy for pain. Neuroimage,
36, 256–267.
Herek, G. M. (1999). AIDS and stigma. American Behavioral
Scientist, 42, 1102–1112.
Hewstone, M., Macrae, C. N., Griffiths, R., & Milne, A. (1994).
Cognitive models of stereotype change: 5. Measurement,
development, and consequences of subtyping. Journal of
Experimental Social Psychology, 30, 505–526.
Hygge, S. (1976). Information about the modelʼs unconditioned
stimulus and response in vicarious classical conditioning.
Journal of Personality and Social Psychology, 33, 764–777.
Jackson, P. L., Brunet, E., Meltzoff, A. N., & Decety, J. (2006).
Empathy examined through the neural mechanisms
involved in imagining how I feel versus how you feel
pain. Neuropsychologia, 44, 752–761.
Jackson, P. L., Meltzoff, A. N., & Decety, J. (2005). How do
we perceive the pain of others: A window into the neural
processes involved in empathy. Neuroimage, 24, 771–779.
Jackson, P. L., Rainville, P., & Decety, J. (2006). To what extent
do we share the pain of others? Insight from the neural
bases of pain empathy. Pain, 125, 5–9.
Kim, S. H., & Hamann, S. (2007). Neural correlates of positive
and negative emotion regulation. Journal of Cognitive
Neuroscience, 19, 776–798.
Kozak, M., Marsh, A., & Wegner, W. (2006). What do I think
youʼre doing? Action identification and mind attribution.
Journal of Personality and Social Psychology, 90, 543–555.
Krendl, A. C., Macrae, C. N., Kelley, W. M., Fugelsang, J. A.,
& Heatherton, T. F. (2006). The good, the bad, and the
ugly: An fMRI investigation of the functional anatomic
correlates of stigma. Social Neuroscience, 1, 5–15.
Lamm, C., Batson, C. D., & Decety, J. (2007). The neural
substrate of human empathy: Effects of perspective-taking
and cognitive appraisal. Journal of Cognitive Neuroscience,
19, 42–58.
Link, B., & Phelan, J. (2001). Conceptualizing stigma. Annual
Review of Sociology, 27, 363–385.
Moriguchi, Y., Decety, J., Ohnishi, T., Maeda, M., Mori, T.,
Nemoto, K., et al. (2007). Empathy and judging otherʼs
pain: An fMRI study of alexithymia. Cerebral Cortex, 17,
2223–2234.
Morrison, I., Lloyd, D., di Pellegrino, G., & Roberts, N. (2004).
Vicarious responses to pain in anterior cingulate cortex:
Is empathy a multisensory issue. Cognitive, Affective,
and Behavioral Neuroscience, 4, 270–278.
Neumann, R., Hulsenbeck, K., & Seibt, B. (2004). Attitudes
towards people with AIDS and avoidance behavior:
Automatic and reflective bases of behavior. Journal
of Experimental Social Psychology, 40, 543–550.
Ochsner, K. M., Bunge, S. A., Gross, J. J., & Gabrieli, J. D.
(2002). Rethinking feelings: An fMRI study of the cognitive
regulation of emotion. Journal of Cognitive Neuroscience,
14, 1215–1229.
Ogino, Y., Nemoto, H., Inui, K., Saito, S., Kakigi, R., & Goto,
F. (2007). Inner experience of pain: Imagination of pain
while viewing images showing painful events forms
subjective pain representation in human brain. Cerebral
Cortex, 17, 1139–1146.
Plant, E. A., & Devine, P. G. (1998). Internal and external
motivation to respond without prejudice. Journal
of Personality and Social Psychology, 75, 811–832.
Posner, M. I., Rothbart, M. K., & Sheese, B. E. (2007).
The anterior cingulate gyrus and the mechanism of
self-regulation. Cognitive, Affective, and Behavioral
Neuroscience, 7, 391–397.
Preston, S., & de Waal, F. (2002). Empathy: Its ultimate and
proximate bases. Behavioral and Brain Sciences, 25, 1–72.
Saarela, M. V., Hlushchuk, Y., Williams, A. C., Schurmann, M.,
Kalso, E., & Hari, R. (2007). The compassionate brain:
Humans detect intensity of pain from anotherʼs face.
Cerebral Cortex, 17, 230–237.
Simon, D., Craig, K. D., Miltner, W., & Rainville, P. (2006).
Brain responses to dynamic facial expressions of pain.
Pain, 126, 309–318.
Singer, T., Seymour, B., OʼDoherty, J., Kaube, H., Dolan,
R. J., & Frith, C. D. (2004). Empathy for pain involves the
affective but not sensory components of pain. Science,
303, 1157–1161.
Singer, T., Seymour, B., OʼDoherty, J. P., Stephan, K. E.,
Dolan, R. J., & Frith, C. D. (2006). Empathic neural responses
are modulated by the perceived fairness of others.
Nature, 439, 466–469.
Stürmer, S., Snyder, M., Kropp, A., & Siem, B. (2006).
Empathy-motivated helping: The moderating role of
group membership. Personality and Social Psychology
Bulletin, 32, 943–956.
Vaughan, K. B., & Lanzetta, J. T. (1980). Vicarious instigation
and conditioning of facial expressive and autonomic
responses to a modelʼs expressive display of pain.
Journal of Personality and Social Psychology, 38,
909–923.
Weiner, B., Perry, R. P., & Magnusson, J. (1988). An attributional
analysis of reactions to stigmas. Journal of Personality
and Social Psychology, 55, 738–748.
Yabar, Y., Johnston, L., Miles, L., & Peace, V. (2006). Implicit
behavioral mimicry: Investigating the impact of group
membership. Journal of Nonverbal Behavior, 30, 97–113.
Zaki, J., Ochsner, K., Hanelin, J., Wager, T., & Mackey, S. (2007).
Different circuits for different pain: Patterns of functional
connectivity reveal distinct networks for processing pain
in self and others. Social Neuroscience, 2, 276–291.
Decety, Echols, and Correll
997
D
o
w
n
l
o
a
d
e
d
l
l
/
/
/
/
j
f
/
t
t
i
t
.
:
/
/
f
r
o
m
D
h
o
t
w
t
n
p
o
:
a
/
d
/
e
m
d
i
f
t
r
o
p
m
r
c
h
.
s
p
i
l
d
v
i
e
r
e
r
c
c
t
.
h
m
a
i
r
e
.
d
u
c
o
o
m
c
/
n
j
a
o
r
c
t
i
n
c
/
e
a
-
p
r
d
t
i
2
c
2
l
5
e
-
9
p
8
d
5
f
1
/
9
2
3
2
9
/
1
5
5
/
9
9
o
8
c
5
n
/
1
2
0
7
0
6
9
9
7
2
4
1
6
2
6
/
6
j
o
p
c
d
n
.
b
2
y
0
g
0
u
9
e
.
s
t
2
o
1
n
2
6
0
6
7
.
S
p
e
d
p
f
e
m
b
y
b
e
g
r
u
2
e
0
2
s
3
t
/
j
f
/
.
.
.
t
o
n
1
8
M
a
y
2
0
2
1